Article Text

Abstract
Background/aims To characterise the baseline prevalence of subretinal fluid (SRF) and its effects on anatomical and visual acuity (VA) outcomes in diabetic macular oedema (DME) and retinal vein occlusion (RVO) following anti-vascular endothelial growth factor (VEGF).
Methods This is a retrospective cohort study of 122 DME and 54 RVO patients who were initiated on anti-VEGF therapy with real-world variable dosing. The DME and RVO cohorts were subclassified based on the presence of SRF at presentation. Snellen VA was measured and converted to logarithm of the minimum angle of resolution (LogMAR). Changes in VA and central subfield thickness (CST) were assessed up to 24 months.
Results SRF was present in 22% and 41% in DME and RVO patients, respectively. In the DME subcohort, eyes with SRF showed an improvement of 0.166 logMAR (1.7 Snellen chart lines) at 12 months and 0.251 logMAR (2.6 Snellen chart lines) at 24 months, which were significantly greater compared with those of the non-SRF group. A significantly greater reduction in CST was noted in the SRF eyes compared with the non-SRF eyes at 3 months and 1 month in the DME and RVO subcohorts, respectively.
Conclusion Baseline SRF is a good marker for a greater reduction in CST in both DME and RVO, but an improvement in VA associated with SRF may be only noted in DME.
- Retina
- Treatment Medical
- Vision
Data availability statement
Data are available upon reasonable request. Parties interested in data access should contact JP (jeffjy.park@mail.utoronto.ca).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patients with diabetic macular oedema (DME) and retinal vein occlusion (RVO) demonstrate variable response to anti-vascular endothelial growth factor (VEGF) therapy. Presence of subretinal fluid (SRF) may serve as a prognostic marker for treatment outcomes, but the direction of effect is still controversial.
WHAT THIS STUDY ADDS
This is the first study to study the prevalence of SRF in DME and RVO concurrently in the same tertiary retina centre. Following a real-world variable dosing of anti-VEGF, baseline SRF was associated with rapid resolution of macular oedema in both DME and RVO, but improvement in visual acuity was associated with SRF only in DME.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The results of this study are hypothesis-generating and may spur further research investigating mechanistic explanation for the development of SRF and its impact on visual prognosis. This study may aid in clinical decision making for ophthalmologists treating DME and RVO.
Introduction
Diabetic macular oedema (DME) and retinal vein occlusion (RVO) are important causes of vision impairment in patients of working age with approximately 103 million, 19 million and 28 million people globally affected by diabetic retinopathy, clinically significant DME and RVO, respectively.1–4 In both DME and RVO, the mainstay of treatment for macular oedema is intravitreal injection of anti-vascular endothelial growth factor (VEGF) agents.5–7 Despite the well-documented success and safety of anti-VEGF agents, there is variability in response to therapy, with some patients experiencing an incomplete response or developing pharmacological resistance.8 9
One factor that may be associated with differential response to anti-VEGF agent is the presence of subretinal fluid (SRF), which is the accumulation of serous fluid in the subretinal space in the absence of retinal breaks or tears. The prevalence of SRF ranges from 18% to 32% in DME10–13 and 40% to 57% in RVO,14–17 suggesting a complex disease pathophysiology that involves the breakdown of the outer retinal-blood barrier. Several studies have evaluated the prognostic utility of SRF at baseline.10–21 Notably, a previous study of DME patients in the RISE and RIDE trials demonstrated that SRF at baseline was correlated with better visual outcomes and resolution of retinal thickening on optical coherence tomography (OCT) after 24 months of therapy.21 In a post hoc analysis from BRAVO and CRUISE trials, SRF at baseline did not influence the visual outcomes of RVO after 12 months of ranibizumab.17 In a separate post hoc analysis for BRAVO/CRUISE patients followed up to 2 years, a large amount of SRF was associated with central subfield thickness (CST)≤250 μm in branch RVO, while absence of SRF was associated with CST≤250 μm in central RVO.18 These pivotal trials, however, evaluate the effects of mandatory monthly injections of a single agent as opposed to real-world variable dosing. Furthermore, the current literature is still controversial regarding the effects of baseline SRF on the visual outcomes and response to therapy, and most data were obtained at 1 year or less.10 12 13 17
Herein, we study the prevalence of SRF in both DME and RVO to determine the effects of SRF on the anatomical and visual outcomes in eyes treated with real-world variable dosing regimen of intravitreal anti-VEGF agents for macular oedema. We also evaluate the prognostic utility of baseline SRF for long-term treatment outcomes in DME and RVO patients and characterise both the eye with SRF and fellow eye in patients requiring anti-VEGF injections.
Materials and methods
Study participants
This is a single-centre, retrospective study of all consecutive adult patients (≥18 years old) with DME or RVO who initiated anti-VEGF for macular oedema between 1 January 2016 and 31 December 2017 at St. Michael’s Hospital, Unity Health Toronto. All cases with macular oedema involving the fovea due to either DME or RVO on baseline OCT imaging were included. Those with other vitreoretinal disorders, macular oedema due to other retinal diseases such as age-related macular degeneration (AMD) and history of intravitreal injections prior to the study period were excluded.
Baseline clinical characteristics
All cases were separated into two subcohorts based on the diagnosis of DME or RVO. Baseline characteristics including age, sex, systemic diseases, presence of DME or RVO, disease laterality and lens status were abstracted using electronic medical records. Prior to starting intravitreal injections, all patients at our centre undergo a comprehensive ophthalmic examination including the measurement of visual acuity (VA), slit lamp examination, dilated fundus examination and OCT to characterise the extent of retinal disease.
OCT imaging evaluation
The OCT imaging at baseline, 1, 3, 6, 12 and 24 months was reviewed for all included eyes. The presence of SRF was ascertained by the anatomical separation of the neurosensory retina and the RPE. The presence of epiretinal membrane (ERM) was confirmed by the hyper-reflective layer on the inner limiting membrane. Quantitative parameters including central subfield thickness (CST), macular cube volume (MCV) and cube average thickness (CAT) were obtained from the computational software output.
Patients were stratified into SRF versus non-SRF group based on the presence or absence of SRF on baseline OCT. For each patient in the SRF group, the eye with SRF was determined to be the study eye. In cases of bilateral SRF, the eye with the first presentation of disease or first intravitreal injection was noted as the study eye. In the non-SRF group, the eye with intraretinal fluid (IRF) was determined to be the study eye for each patient, while for bilateral IRFs the eye with the first presentation of disease or first intravitreal injection was noted as the study eye.
Clinical outcomes following intravitreal anti-VEGF
All patients received intravitreal injections of bevacizumab, ranibizumab or aflibercept. As per standard practice in our practice, efforts are made to see the patients every month regardless of the treatment regimen. Switching between anti-VEGF agents occurred if patients failed to respond to therapy and experienced adverse effects among other patient or provider-related factors. Patients with RVO received three initial loading doses followed by a treat-and-extend regimen with retreatment decisions largely based on the individual clinician’s judgement of disease activity. Patients with DME were treated according to the protocol adapted from the Diabetic Retinopathy Clinical Research Network Protocol T given the first-year results of the study.5 Briefly, DME patients received monthly injections unless VA was 20/20 with CST below 305 µm for males and 290 µm for females, and there was no change in response to previous two injections.5 At 6 months, an injection was withheld if no change after two consecutive injections and only resumed if VA or CST worsened.5 Injections were given pro re nata (PRN) once macula was dry with resolution of oedema.
The primary outcome of this study was VA measured using Snellen chart with habitual or pinhole correction. Snellen visual acuities were converted to logMAR for the purpose of statistical analysis. Counting fingers, hand motions, light perception and no light perception were converted to logMAR values of 2.0, 2.4, 2.7 and 3.0, respectively. A clinically significant improvement in VA was defined as improvement equal to or greater than 0.097 logMAR (equivalent to 1 line) from baseline. Secondary outcomes included the percent change of CST from baseline, number of intravitreal anti-VEGF, follow-up length and type and incidence of secondary therapy.
Statistical analysis
Descriptive statistics was used to summarise baseline characteristics, prevalence of SRF, visual outcomes, anatomical outcomes, follow-up duration and injection frequency. Continuous variables were reported using means and SD, while categorical variables were reported using frequency and proportions. Range was reported for the follow-up duration. Independent samples t-test was performed for continuous variables and χ2 test was performed for categorical variables, comparing the patient baseline characteristics and outcome variables between the SRF and non-SRF groups within each of the DME and RVO subcohorts. A binary logistic regression analysis was conducted to compare the prevalence of bilateral macular oedema between SRF and non-SRF groups. A linear regression was conducted with SRF status as the independent variable and logMAR VA change from baseline as the dependent variable. Based on a priori variable selection, clinically important variables including age, sex, lens status and logMAR VA at baseline were selected as covariates in the linear regression analysis. Odds ratio (OR), mean difference and 95% CIs were calculated to determine whether a significant difference existed in the sample means or proportions between SRF and non-SRF groups. A p value of <0.05 was considered for statistical significance. Data was analysed using SPSS V.27 (SPSS).
Patient and public involvement
The development and design of the protocol involved consultation with academic ophthalmologists and members of the scientific community that consume literature in the field of ophthalmology. The challenges experienced by patients who received intravitreal therapy for retinal disorders influenced the development of the research question. The results from this study will be disseminated to local and national ophthalmology communities including professional societies and journals.
Results
Baseline characteristics
A total of 122 patients with DME and 54 patients with RVO were included in the analysis. Baseline patient and eye characteristics are summarised in table 1. In the DME subcohort, patients with SRF had significantly fewer number of proliferative diabetic retinopathy (PDR) in the study eye (n=3, 11%) compared with the non-SRF group (n=29, 31%; p=0.043). Patients with SRF were more likely to have bilateral macular oedema at baseline (OR, 2.7; 95% CI: 1.1, 6.4; p=0.027). There were significant differences in the baseline OCT parameters between the SRF group and the non-SRF group. The study eyes of SRF patients had a mean CST that was 108 µm greater (95% CI: 42, 174; p=0.002), MCV that was 1.49 mm3 greater (95% CI: 0.51, 2.46; p=0.004) and CAT that was 41 µm greater (95% CI: 14, 68; p=0.004) than those of the non-SRF group. The fellow eye of SRF patients had a mean CST that was 60 µm greater (95% CI: 6, 113; p=0.031).
Baseline patient demographics and eye characteristics for DME and RVO
In the RVO subcohort, the study eyes of SRF patients had a mean CST that was 134 µm greater (95% CI: 59, 209; p=0.001), while their fellow eyes had a mean MCV that was 0.60 mm3 greater (95% CI: 0.08, 1.12; p=0.021) and CAT that was 17 µm greater (95% CI: 3, 31; p=0.018) compared with the respective eyes of the non-SRF group.
Prevalence of SRF
At baseline, SRF was present in 27 eyes (22%) and 22 eyes (41%) in the DME and RVO subcohorts, respectively (table 2). Five patients (19%) with DME had bilateral SRF, while only one RVO patient (5%) had bilateral SRF. The largest reduction in the prevalence of SRF was observed at 1 month for both subcohorts. By 24 months, the prevalence of SRF in the study eye decreased to 3% for both DME and RVO.
Prevalence of SRF in study and fellow eyes with DME and RVO
VA outcomes
Table 3 shows VA at baseline and at follow-up points after intravitreal anti-VEGF injections. DME eyes with SRF demonstrated a mean VA at 24 months that was significantly higher compared with baseline (p=0.016), while RVO eyes with SRF demonstrated a mean VA at 12 months that was significantly higher compared with baseline (p=0.048). No significant differences between baseline and follow-up VA were observed for non-SRF eyes in either diagnostic subcohort.
Visual acuities at baseline and at follow-up for study eyes with DME and RVO
Figure 1A and B shows the change in logMAR VA from baseline up to 24 months for DME and RVO subcohorts, respectively. In the DME subcohort, study eyes with SRF demonstrated a mean reduction in logMAR VA of 0.166 (1.7 Snellen chart lines) at 12 months and 0.251 (2.6 Snellen chart lines) at 24 months, which were significantly greater compared with the mean logMAR VA reduction of the non-SRF group. The difference in logMAR VA change compared with the non-SRF group was −0.170 (1.8 Snellen chart lines; 95% CI: −0.337, –0.003; p=0.046) at 12 months and −0.329 (3.4 Snellen chart lines; 95% CI: −0.569, –0.090; p=0.008) at 24 months. After adjusting for age, sex, lens status and baseline VA, there was evidence to suggest that the association between baseline SRF and the change in logMAR VA remains significant at 12 months (beta coefficient, −0.170; 95% CI: −0.337, –0.003; p=0.046) and at 24 months (β, −0.329; 95% CI: −0.569, –0.090; p=0.008). There was no evidence of difference in the effect of baseline SRF on VA outcomes demonstrated in the RVO subcohort.
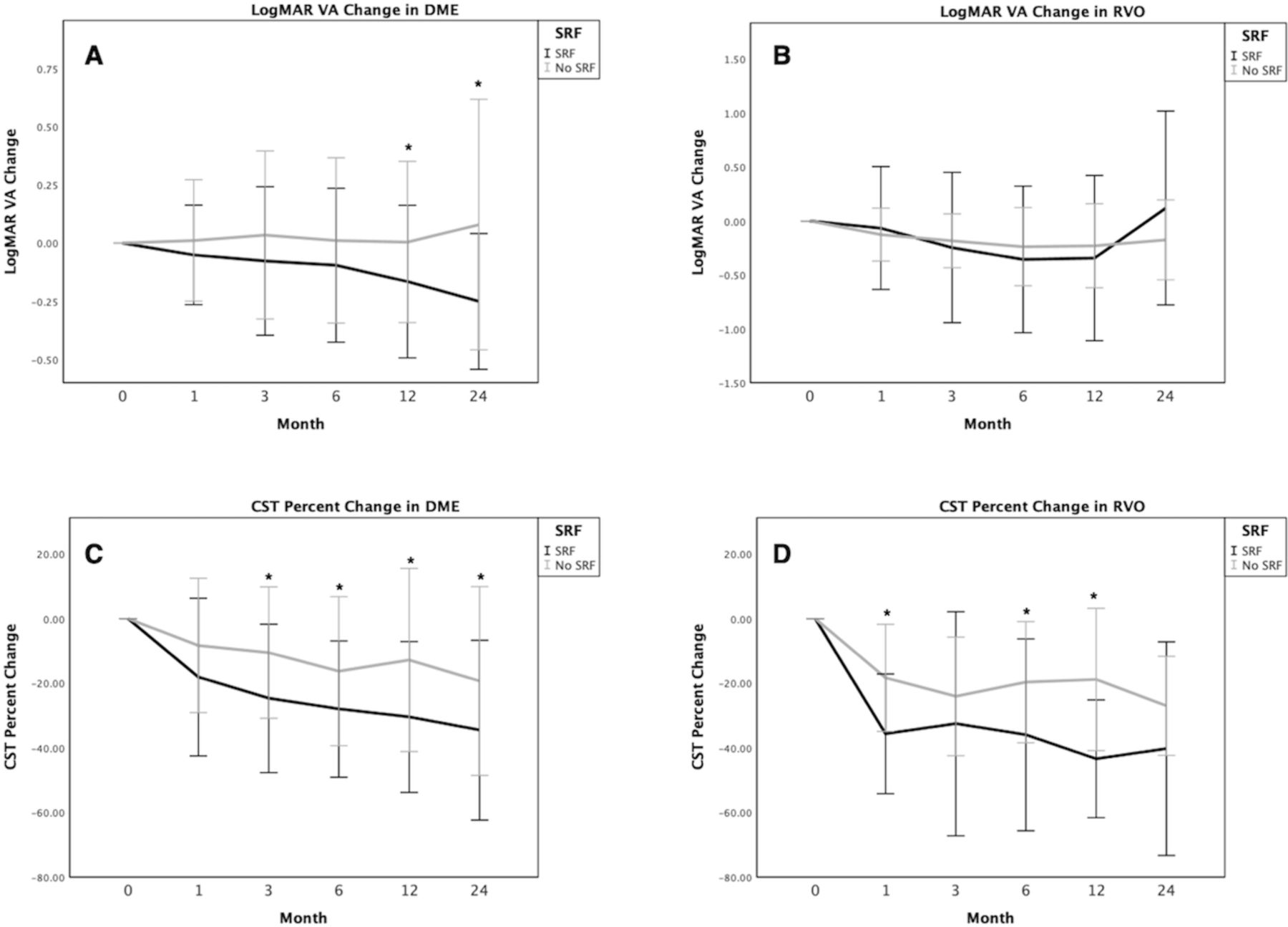
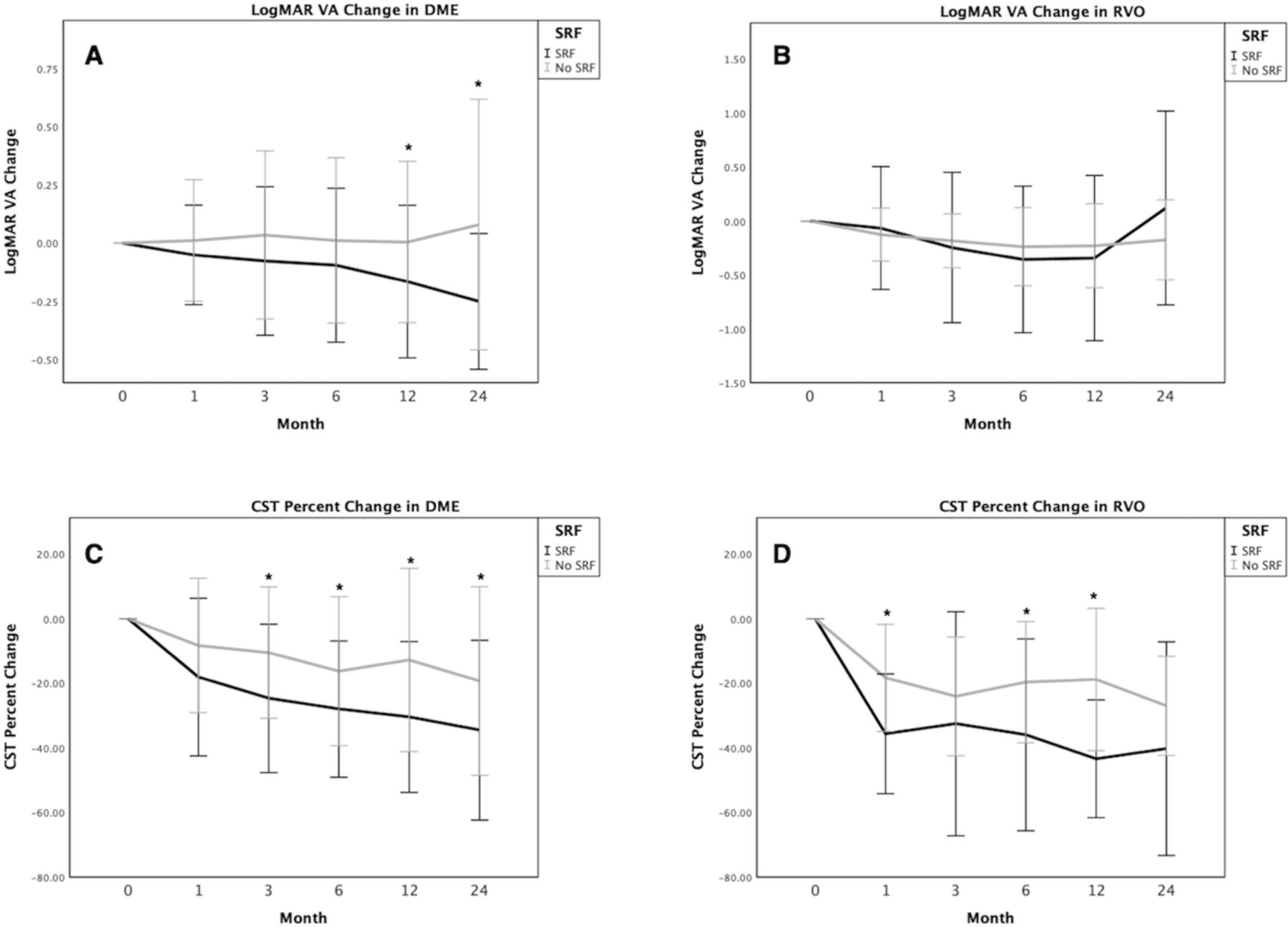{kind=link}
Visual and anatomic recovery in DME and RVO following anti-VEGF treatment. A and B show change in logMAR VA from baseline. Significant differences (p<0.05) in mean logMAR VA change were observed between DME patients with SRF and without SRF at 12 and 24 months. C and D show per cent change in CST from baseline. Eyes with SRF demonstrated greater reduction in CST from baseline compared with those without SRF for both diagnostic subcohorts. Created using SPSS. *p<0.05. Errors bars represent SD. CST, central subfield thickness; DME, diabetic macular oedema; LogMAR, logarithm of the minimum angle of resolution; RVO, retinal vein occlusion; SRF, subretinal fluid; VA, visual acuity.
In the DME subcohort, 16 patients (73%) with baseline SRF and 24 patients (36%) without baseline SRF achieved a clinically significant VA improvement ≥0.097 logMAR (1 Snellen chart line) at 24 months. However, 3 patients (14%) with baseline SRF and 16 patients (24%) without SRF lost vision compared with baseline. Meanwhile in the RVO subcohort, 8 patients (67%) with baseline SRF and 11 patients (42%) without baseline SRF achieved a clinically significant VA improvement at 24 months. Compared with baseline, 3 patients (25%) and 7 patients (27%) lost vision.
Anatomical outcomes
Figure 1C and D shows the per cent change in CST from baseline up to 24 months for DME and RVO subcohorts, respectively. In the DME subcohort, the per cent change in CST of the SRF study eyes was significantly reduced than that of the non-SRF eyes at and after 3 months. Notably, the CST was reduced by 25% at 3 months, which is 14% more (95% CI: 4, 24; p=0.007) than the change in non-SRF eyes. At 24 months, CST was reduced by 35%, which is 15% (95% CI: 1, 29; p=0.037) more than the change in non-SRF eyes.
In the RVO subcohort, SRF eyes demonstrated a percentage reduction in CST of 36% which is 17% more (95% CI: 5, 28; p=0.002) than the non-SRF eyes at 1 month. At 12 months, mean CST was 43% reduced which is 25% more (95% CI: 12, 37; p<0.001). No statistically significant difference in the mean CST reduction was observed between SRF and non-SRF eyes at 24 months.
Follow-up duration and treatments
In the DME subcohort, patients with SRF had a significantly longer follow-up duration of 22.3±5.0 months compared with the non-SRF group with 19.4±7.2 months (p=0.018). At 24 months, the mean number of injections for DME was 9.7±5.1 in the SRF group and 8.2±5.3 in the non-SRF group. In the RVO subcohort, patients with SRF had a follow-up duration of 20.7±5.5 months, while the non-SRF group were followed up for 21.4±5.7 months. At 24 months, the mean number of injections for DME was 12.5±5.9 in the SRF group and 12.0±5.4 in the non-SRF group.
None of the SRF eyes received intravitreal corticosteroids, and the incidence of panretinal photocoagulation and pars plana vitrectomy was very low in the follow-up period for both DME and RVO (online supplemental table 1), which summarises secondary treatments required over the 24-month period).
Supplemental material
Discussion
The current study adds to the existing literature by characterising the prevalence of SRF, as well as visual and anatomical outcomes of eyes with or without SRF following anti-VEGF for treatment based on real-world variable dosing. To our knowledge, this study is the first to demonstrate the effects of SRF in DME and RVO simultaneously from the same tertiary retina centre. The prevalence of baseline SRF reported in this study allows a direct comparison between two diagnostic cohorts. We also demonstrate significant differences in the change in VA and CST from baseline based on the presence of baseline SRF.
The baseline characteristics of patients with SRF were compared against the patients without SRF. A novel finding is the greater frequency of bilateral macular oedema in DME patients with SRF. Consistent with this is the significantly greater baseline CST in both the study and fellow eyes of patients with SRF compared with the respective eyes without SRF in our study. One explanation is that SRF formation is a systemic process and that the mechanisms associated with RPE dysfunction promote accumulation of fluid intraretinally in the fellow eye even in the absence of SRF.22 A previous study found associations of SRF with systemic diseases such as renal diseases, suggesting that a systemic source of VEGFs may contribute to RPE dysfunction.23
The prevalence of SRF was 23% and 43% for DME and RVO, respectively. These findings are comparable to previous reports for DME (18%–32%) and RVO (40%–57%), but no previous study has characterised SRF in both disease entities concurrently from patients attending the same retina centre.10–17 Furthermore, the resolution of SRF occurred very early in the follow-up period, as the prevalence of SRF was nearly halved in both DME and RVO at 1 month after just a single injection. The rapid resolution of SRF was also reported in previous studies and indicates that SRF responds well to initial therapy involving anti-VEGF.17 24
Eyes with SRF achieved a greater reduction in CST compared with those without SRF as early as 3 months for DME and at 1 month for RVO subcohort. Previously, Kim et al25 showed that the reduction in central foveal thickness was more evident in DME eyes with SRF at 1 month following treatment. Dogan et al14 demonstrated that BRVO eyes with SRF achieved greater reduction in central macular thickness at 1 month. Higher levels of intraocular VEGF are found in eyes with SRF compared with those without.26 It is not surprising that anti-VEGF agents would lead to significant anatomical improvements should VEGF mediate RPE dysfunction and subsequent leakage of fluid into the subretinal space.
Following the initiation of anti-VEGF therapy, DME patients with SRF demonstrated 24-month VA that was significantly greater than baseline VA. Furthermore, the improvement in logMAR VA was significantly greater compared with those without SRF at 12 and 24 months. This finding is consistent with the results of a previous study of DME patients in the RISE and RIDE trials, which demonstrated that baseline SRF predicts improvement from baseline best-corrected VA of 15 or more at 24 months.21 Even among patients receiving anti-VEGF for neovascular AMD, the presence of SRF compared with IRF was associated with excellent visual outcomes at 1 and 2 years in large scale clinical trials.27 28 The exact mechanism explaining this potentially protective role of SRF in various retinal conditions is unclear. A recent finding is that disruption in the photoreceptor integrity occurs more frequently in eyes with SRF compared with those without.13 Although not confirmed in our study, it is possible that the significant differences in vision improvement corresponded with the recovery of photoreceptor integrity in SRF eyes following long-term anti-VEGF treatment.29
Meanwhile, a larger improvement in VA may be attributed to a poorer baseline VA, which allows any improvement in vision to be more apparent. In both of our DME and RVO cohorts; however, there were no significant differences in the baseline logMAR VA between the patients with and without SRF. In addition, the differences in mean change in logMAR VA remained significant after adjusting for age, sex, lens status and baseline VA, making it less likely that the findings of our study were due to a difference in baseline VA between the groups.
In our study, no significant differences between the groups in mean VA change were observed in the earlier follow-up period prior to 12 months. This is in contrast to other studies that have observed significant differences in VA improvement in the earlier months following the initiation of DME treatment with anti-VEGF.19 20 Notably, a post hoc analysis of BRDME study participants demonstrated that baseline SRF predicted significant improvement in best-corrected VA letter score as early as 3 and 6 months.20 Although unlikely, this difference may be due to the difference in the inclusion criteria as we had strictly included patients that were anti-VEGF treatment naive who were at the earliest stages of their treatment regimen, and thus any functional improvement may have occurred later in our study period. With respect to our RVO subcohort, there were no significant differences in vision outcomes with respect to the presence of baseline SRF, consistent with the findings from a large post hoc analyses of patients from BRAVO and CRUISE studies.17 Overall, our study involving the real-world variable dosing and selection of anti-VEGF for DME and RVO patients confirm the findings of the post hoc analysis of the pivotal trials (RISE/RIDE and BRAVO/CRUISE), which were based on strict monthly injections of ranibizumab only.
It is important to note that this study was retrospective in nature and as such there was variability in follow-up intervals and the choice of anti-VEGF treatment regimen involving bevacizumab, ranibizumab or aflibercept for each patient. The variable dosing employed in our centre has the advantage of representing the practice pattern of ophthalmologists in a real-world clinical setting. The findings are also based a smaller sample size, despite being one of the largest centres with high volumes of patients presenting with retinal conditions. Future studies may help elucidate the photoreceptor integrity associated with the presence of SRF, the mechanisms underlying the development of bilateral macular oedema or bilateral SRF in patients as well as the clinical implications associated with the presence of bilateral disease at baseline. Identifying any other patient characteristics associated with faster resolution of macular oedema would be helpful for patient selection for treatment with anti-VEGF.
In conclusion, the current study evaluates the effects of baseline SRF on DME and RVO following variable treatment regimens in a real-world clinical setting. The visual improvement noted in DME eyes with SRF was greater than that of eyes without SRF, but no similar association was demonstrated in RVO patients. Significant VA improvement in the SRF compared with non-SRF patients was demonstrated only after 12 months of anti-VEGF injections and did not parallel the rapid resolution of SRF and reduction in CST. The presence of SRF at baseline may thus have significant clinical implications on patients undergoing therapy, and it may be used in clinical decision making for ophthalmologists treating DME and RVO.
Data availability statement
Data are available upon reasonable request. Parties interested in data access should contact JP (jeffjy.park@mail.utoronto.ca).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Unity Health Toronto Research Ethics Board (Unity Health Toronto Research Ethics Board REB # 20-067) and adhered to the tenets of the 1964 Declaration of Helsinki and its later amendments, alongside the Health Insurance Portability and Accountability Act.The study was approved by IRB following a rigorous evaluation. Patient consent was not deemed necessary given the appropriate measures taken to de-identify all data.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Study Design: JP, TF, DTW
Data Collection: JP, IZK
Data Analysis: JP, TF
First Draft of Manuscript: JP
Critical Revision of Manuscript: JP, TF, IZK, FA, DRC, DTW
Acts as Garantor of Work: DTW
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.