Article Text

Abstract
Objective Self-refracting spectacles (SRSs) have different optical and mechanical designs, which may affect the refractive outcome, depending on the experience of the end user. This study compared the performance of two SRS among children in Ghana.
Methods and analysis A cross-sectional study of two Alvarez variable-focus SRS designs was conducted. A total of 167 children (mean age 13.6±1.6 years) identified as having refractive error were recruited from 2465 students who underwent screening. Subjects completed self-refraction using FocusSpecs, and Adlens, autorefraction and cycloplegic subjective refraction (CSR) (gold standard). Wilcoxon signed-rank test was used to compare visual outcomes and accuracy of refraction and graphically illustrated using Bland-Altman plots.
Results Eighty (47.9%) urban and 87 (52.1%) rural children were analysed and only about one-quarter 40 (24.0%) wore spectacles. The proportion who achieved visual acuity of ≥6/7.5 with FocusSpec, Adlens, autorefraction and CSR among urban schools were 92.6%, 92.4%, 60% and 92.6%, while those in rural schools were 81.6%, 86.2%, 54.0% and 95.4%, respectively. The mean±SD spherical equivalent errors for urban and rural schools using FocusSpec, Adlens and CSR were −1.05±0.61 D, –0.97±0.58 D and −0.78±0.53 D; and −0.47±0.51 D, –0.55±0.43 D and −0.27±0.11 D, respectively. The mean differences between the two self-refraction spectacles for urban and rural schools were not statistically different (p>0.00) but differed significantly when both were compared with the gold standard (CSR) (p<0.05).
Conclusion Background and refraction experience of school children did not significantly affect self-refraction.
- Child health (paediatrics)
- Optics and Refraction
- Public health
Data availability statement
Data are available on reasonable request. Data are available on reasonable request. The datasets used and analysed during the current study are available from the corresponding authors on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Previous studies have indicated that a range of good refractive results and visual acuity were achievable with self-refraction, although there are discrepancies in accuracy of results reported, possibly due to several factors including the background and refraction experience of the subjects used.
WHAT THIS STUDY ADDS
By employing two commercially available Alvarez variable-focus self-refraction spectacles, the study shows that self-refraction among children from a less resourced environment, in rural and urban sittings, did not differ significantly from each other despite variable refraction experience among the children, but only shows a difference when self-refraction was compared with clinical standard.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The results indicate that self-refraction devices are capable of achieving acceptable refractive accuracy and visual acuity outcomes in children from low-resourced environments, but an easier mechanism of self-adjusting the spectacles must be taken into account to match clinical standards and increase wear compliance.
Introduction
Access to primary eye care services is essential to prevent avoidable visual impairment (VI) and blindness in children. Global estimates in 2010 indicated that 19 million children below the age of 15 years have VI, out of which 12 million are due to refractive error and more than two-thirds of them are found in low-income and middle-income countries.1 Compared with the other major causes of VI, refractive error sets in at a younger age, and constitutes the most prevalent cause of disabling visual disorder in children.1 Therefore, if not corrected, refractive error causes more blind-years than other causes in school-going children, particularly those from low-income and middle-income countries, who represent the greater portion of the vulnerable group with significant problems of undetected or uncorrected refractive error,2–5 leading to considerable impact on their participation and learning in class.3 According to the WHO, in low-income and middle-income countries, children with vision loss are 2–5 times less likely to be in formal education, but refractive error correction by spectacles can reduce the odds of failing a class by 44%.6
However, in many low-income and middle-income countries, various barriers prevent many children with refractive errors from accessing eye health services and achieving the classroom success. These barriers include the cost of spectacles,7 concerns about cosmetic appearance8 and inadequate understanding of the benefits of refractive correction among children, parents and teachers.9 10 In addition, although refractive error may be safely and effectively corrected with spectacles, there is a lack of well-trained optometrists and ophthalmologists in settings of limited resources.11 12 To help solve the problems associated with the traditional way of correcting refractive error, self-refracting spectacles (SRSs) or adjustable spectacles were developed to provide a simple, effective and affordable means of vision correction whereby it is possible for the wearer to adjust the refractive power of each lens independently to optimise his or her vision. This approach makes vision correction accessible to those in areas of the world where there is either a lack of professionally trained optometrists or where the cost of traditional spectacle lenses and professional consultation is expensive. Specifically, SRSs have been recommended for school children in rural communities who have no or little access to refractive services.13 14 Examples of such commercially available SRS are eye adjusters (Eyejusters 2015, Oxford, UK), Adspecs, (Centre for Vision in the Developing World, Oxford, UK), Superfocus device (Superfocus, Van Nuys, California, USA), Adlens (Eyejusters 2015, Oxford, UK) and FocusSpecs (Focus-on-Vision, Eindhoven, Netherlands).
Notwithstanding the intended use of SRS, to be able to use the SRS effectively, the child must understand and perform the self-adjustment according to a manufacturer instruction. However, commercially available SRSs have different optical designs (usually Alvarez and fluid-filled) and mechanisms of administering the self-refraction, which may affect the refractive and visual outcome. Though few studies15–18 have compared the accuracy of some SRS to the traditional way of refraction, to the best of our knowledge, no study has investigated the influence of refraction experience among school children of different settings on the refractive and visual accuracy of SRSs.
As known, the burden of VI caused by refractive error is not evenly distributed across and within countries, as over 70% of VI due to refractive error are borne by low-resourced countries and rural settings.19 20 A recent study found that myopia affects about 1 in 20 African school children and in Ghana, the reported myopia prevalence ranged from 1.7% to 22.6%.21 Another study found that more than 72% of VI in school children was caused by inadequately corrected refractive error.20 Urban and rural school children can be said to have different experiences in terms of access to refractive services, compliance and acceptance of recommended optical wear.18 In effect, urban school children may be more likely to be efficient in the use of the SRS compared with their rural counterparts. Given these differences, it is essential that the relative self-refraction experiences of urban and rural children are measured. This study, therefore, compared the accuracy and refractive outcome of two self-refraction spectacles among rural and urban school children to results obtained from three traditional refraction modalities: cycloplegic subjective refraction (CSR), non-cycloplegic refraction and autorefraction. The finding will be relevant in tailoring specific SRS instructions, design and mechanism of refraction to suit the population of interest and promote the use of adjustable spectacles to meet the visual needs of school-going children in low-income and middle-income countries who may have limited access to comprehensive refractive services.
Materials and methods
Study design
Study area and setting
The study was a descriptive cross-sectional one conducted among junior high school children between the ages of 12 and 17 years identified with refractive error from selected basic schools in the rural and urban areas in the Central Region of Ghana. The Region is divided into 20 administrative areas. These are made up of 1 metropolitan, 6 Municipal and 13 Districts. With a population density of about 162 inhabitants per square kilometres, the Central Region is the second most densely populated region in Ghana. About 63% of the region is rural and is classified among the four poorest in the country; with the unemployment rate at 8.0%, 2.4% lower than the national average of 10.4%.22 In terms of eye care, the region has a total of 17 public eye care facilities (12 belonging to the government and 5 belonging to quasi-government), 2 ophthalmologists, 36 optometrists and 47 ophthalmic Nurses. Most facilities and personnel are located in urban areas, leaving the rural areas mostly underserved.22 Basic refraction and optical services are also available in a small number of expensive private optical shops. Periodically, some non-governmental organisations and personnel from public and private health facilities embark on outreaches to provide eye screening services to some schools and communities either singly or in partnership interventions. However, considering the multitude of people requiring refractive services, there is limited access to appropriate eye care services within the region.
Inclusion and exclusion criteria
The following criteria were considered for inclusion into the study: age range 12–17 years with uncorrected visual acuity (VA) less than or equal to 6/12 (0.3 logarithm of the minimum angle of resolution, logMAR) in at least one eye, for myopes and less than or equal to 6/9.5 (0.2 logMAR) in at least one eye for hyperopes; best-corrected VA (BCVA) greater than or equal to 6/7.5 in each eye after subjective refraction; myopia greater than or equal to −1.00 D but less than −5.00 D in one or both eyes (due to the limit of correction in FocusSpecs self-refraction (FSSR) spectacles) and limit of +0.50 to +3.00 D for hyperopes and astigmatism less than or equal to −2.00 D in one or both eyes, and no ocular pathologies, strabismus or amblyopia. Children whose parents/guardians consented to the study completed all examination protocols. Prior to this, personal assent was obtained from all the school children after the purpose and the protocols were explained to them and allowing ample time for questioning.
Sample size calculation and sampling technique
To select school children from urban and rural schools who have refractive errors, an eye screening exercise was conducted. For sampling, a multistage random cluster sampling design was followed based on mapping a geographical corridor of the Central Region. The sampling frame of this study was based on the register of urban and rural schools provided by the Central Regional Education office. First, junior high schools in the Central Region were divided into four district clusters based on the roster provided. Then, 16 schools were randomly selected from the clusters, comprising 8 rural and 8 urban schools from each cluster taking into consideration the various geographical subregions and the socioeconomic characteristics of the districts. The last stage involved a simple random sampling of all students enumerated in the selected schools for the eye screening exercise.
Since the purpose of this survey was to measure the refractive error among school children, the minimum sample size was calculated based on the prevalence of refractive error in the Central Region. Using the formula N= (Z)2 pq(1−p)/(d)2, where N is the minimum sample size, Z is the value of Z statistics at a 95% CI of 1.96, p is the estimated prevalence of 5.0%,19 q is 1−p and d is the absolute precision level (margin of error=0.05), a calculated minimum sample size of 2465 students was required, after adjusting for an anticipated 10% non-participation rate and a design effect of 1.5 due to cluster sampling.
Self-refracting spectacles
Two Alvarez SRS, with significant differences in instructional protocol and optical designs, were used. They both give variable spherical power and are fabricated for relatively low-cost markets. The first of these, the FocusSpec (Focus-on Vision, www.focus-on-vision.org/) is an antireflection coated, polycarbonate lenses (refractive index 1.59) and is available with a power range of −1.00 to −5.00 D for myopes and +0.50 to +4.50 D for hyperopes (see figure 1). The second design, the Adlens Adjustables (Adlens, https://adlens.com/uk/) also uses polycarbonate lenses and has a power range −6.00 to +3.00 D. Both designs have nominally zero astigmatic power at all spherical power settings. The assumption is that the wearer will, by observing a task at the appropriate distance, be able to adjust the spherical power of the lenses to obtain optimal correcting power and vision. Both designs have individual adjustments for the right and left eye lenses, so that the needs of anisometropes are catered for, although at the expense of an increased time requirement for optimising the powers. Both self-refraction spectacles are commercially available and remain stable on the same dioptre after setting. Figure 1 shows a picture of the two SRS, FocusSpec (A) and Adlens (B)
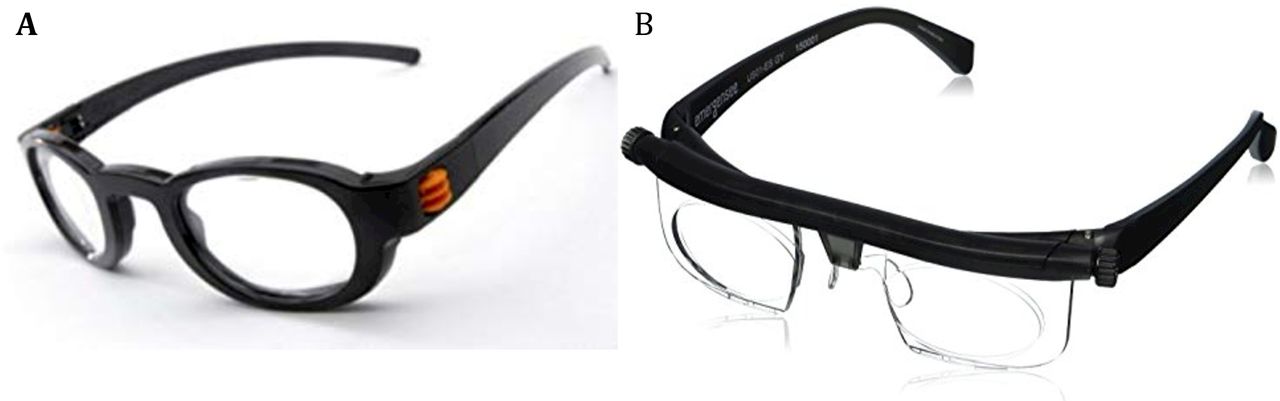
Picture depicting the two SRS, FocusSpec (A) and Adlens (B). SRS, self-refracting spectacles.
Data collection process
Screening
All the pupils in the selected schools underwent a refractive screening programme to determine those who had refractive error according to the inclusion criteria. Refractive screening was conducted using VA and autorefraction. Distance VA was measured using a retro illuminated logMAR chart with tumbling-E optotypes (Precision Vision, La Salle, Illinois USA) under natural illumination. School pupils who had VAs worse or equal to 6/12 (0.3 logMAR) in at least one eye, for myopes and worse or equal to 6/9.5 (0.2 logMAR) in at least one eye for hyperopes were selected for comprehensive refractive assessment. The type and magnitude of error was determined by the aurefraction.
Ocular examination
External and internal examinations were done for all the students who were identified with refractive error to help identify and rule out any pathological cases. This was done with the aid of a portable slit lamp and an ophthalmoscope.
Refraction (self-refraction, autorefraction and CSR)
The main data collection of the SRS was conducted after a pilot study. Eligible children were taken through self-refraction with FocusSpecs and Adlens adjustable spectacles separately based on instructions/protocols that have previously been reported.15–17 Under the supervision of research assistants, the children were instructed to adjust the powers of the SRS accurately as possible until the best VA is obtained in the tested eye, each time occluding the fellow eye. Self-refraction was repeated three times in each eye, and the measurement that gave the best VA was used as the final result. Once the best VA was obtained, the refractive powers of the SRS were measured with a lensometer, and the results documented. Instructions for self-refraction were the same for both urban and rural children.
Next, automatic refraction with an auto refractor was performed by an examiner masked to the results of self-refraction and the results documented. Finally, CSR was performed by another experienced optometrist, who was oblivious of all previous refraction results. Distance retinoscopy (streak retinoscope; Welch Allyn, Skaneateles, New York, USA) was then performed as well as standard subjective refraction, under cycloplegia induced with three drops of 1% cyclopentolate; two drops were administered 5 min apart and the third drop was administered after 20 min. Best sphere and binocular balancing (prism dissociation) were used to refine the spherical component and the results documented. Self-refraction, automatic refraction and CSR were all performed on different days.
Data analysis
VA was measured for uncorrected vision and with correction by FSSR, Adlens self-refraction (ASR), autorefraction and CSR. The data were first screened and assessed for normality based on non-parametric Kolmogorov-Smirnov D tests, (p<0.05).
Wilcoxon signed-rank test was used to assess differences in the proportion of participants achieving BCVA of greater than or equal to 6/7.5 in the right eye across methods. Multiple logistic regression was used to analyse the association of age, sex, non-spectacle wearer, type of school, spherical error and failure to achieve a BCVA of greater than or equal to 6/7.5 among the children with uncorrected VA less than or equal to 6/12 for myopes and 6/9.5 for hyperopes. Measures of refraction across methods were analysed by using spherical equivalent (SE) refractive error and one sample t-test used to determine differences in means across the methods of refraction. Accuracy of self-refraction was assessed by determining the mean difference, SD and 95% confidence limit of agreement between CSR and self-refraction measures and by graphical illustration of Bland-Altman plots. In calculating the 95% CI, adjustments for the effect of cluster sampling were considered. Analyses were performed with SPSS program for Windows (V.22.0; SPSS). Level of statistical significance was set at a p value of less than or equal to 0.05.
Results
Sociodemographic characteristics of study population
Out of a total of 2465 children who underwent ophthalmic screening, 208 (8.4%) identified as having refractive error (presented VA ≤6/12 for myopes and ≤6/9.5 for hyperopes in one eye or in both eyes) were recruited for the study. Of the 208 eligible subjects, 7 were excluded because they could not achieve a BCVA of 6/7.5 owing to macular toxoplasma scar (4 subjects), optic disc atrophy (2 subjects) detected on fundus examination, and 1 due to the presence of ptosis; 11 did not complete all of the examination protocol owing to being absent/scheduling constraints, 4 subjects were excluded for lack of cooperation, and 10 had high astigmatic error that did not fit into our inclusion criteria and 9 did not consent to cycloplegia. The 167 remaining eligible participants formed the basis of analysis of the results.
The mean±SD age of the 167 children was 13.6±1.6 years (range 12–17 years), and the majority were females (74.3%; 124/167). Only about one-quarter 40 (24.0%) of the children wore spectacles at the time of examination. A number of participants from schools in urban and rural settings were 80 (47.9%) and 87 (52.1%), respectively. The distribution of demographic characteristics and refractive status among the type of school the children attended are shown in table 1. Hyperopia was found to be more among children in rural schools (58.0%) whereas urban school pupils were more myopes (54.4%). Spectacle wearers were more among urban school children (72.5%) than rural school pupils.
Distribution of demographics and refractive status among the type of school participants attend
Distribution of VA obtained without correction and with the different methods of refraction correction
The median and mean uncorrected VA in the better-seeing eye for urban schools were 0.3 (6/12) and 0.27 (roughly equivalent to 6/12) while that for rural schools were 0.2 (6/9.5) and 0.26 (roughly equivalent to 6/12), respectively. For the worse-seeing eye, the median and mean uncorrected VA for the urban schools were 0.6 (6/24) and 0.57 (roughly equivalent to 6/24), while that for rural schools were 0.5 (6/19) and 0.53 (roughly equivalent to 6/19), respectively. The median and mean VA which accounted for similar VA in both eyes among urban schools were 0.45 (between 6/19 and 6/15) and 0.514 (roughly equivalent to 6/19) while those among rural schools were 0.3 (6/12) and 0.35 (between 6/15 and 6/12), respectively. Inspection of the distribution of VA between the right eyes and left eyes showed a similar distribution, so analysis of the results was done using the right eye only. Details of visual acuities obtained for rural and urban children without correction and with the different methods of refraction are presented in figure 2. Figure 2 also shows the proportion of children who achieved VA of ≥6/7.5 with self-refractions using FocusSpecs, Adlens, autorefraction and with CSR (as the standard) among those in urban schools were 92.6%, 92.4%, 60% and 92.6%, respectively, while those in rural schools were 81.6%, 86.2%, 54.0% and 95.4%. The median VA for those with similar VA across all methods of refraction in both eyes was 6/6 (0.0). A Wilcoxon signed-rank test conducted to determine if there was a statistically significant difference in the visual acuities obtained between those in urban and rural schools against the different methods of refraction showed that VA distributions differed from each other among rural and urban children (p<0.001) and among the different methods in rural children (p<0.001). Improvement over uncorrected VA in the right eye was greater in urban children than rural children for both self-refraction methods.

Distribution of visual acuity (logMAR) in the right eye without correction and achieved with the different methods of refraction (top panel) and proportion who achieved visual acuity of ≥6/7.5 with the different methods of refraction (bottom panel) among the rural and urban children. logMAR, logarithm of the minimum angle of resolution.
Comparison of self-refraction to clinical standard
The mean SE refractive powers found in all the subjects for FocusSpec, Adlens, autorefraction and CSR were −0.75±0.57 D, −0.74±0.54 D, −0.49±0.01 D and −0.51±0.33 D, respectively.
The mean difference between the SE refractive error for FSSR and ASR was not significant (Wilcoxon signed-rank test; Z=−1.078, p=0.281), with a mean difference of −0.02±0.61 D, and a 95% limit of agreement between −0.10 and +0.10. The mean difference in SE refractive error between FSSR and autorefraction was significant (Z=−5.999, p<0.0001), with a mean difference of −0.26±0.044 D, and a 95% limit of agreement between −0.38 and −0.14. Similarly, the mean difference between ASR and autorefraction was also significant (Z=−4.785, p<0.001), with a mean difference of –0.24±0.04 D, and 95% limit of agreement between −0.35 and −0.14. The mean difference between FSSR and CSR was significant (Z=−5.071, p<0.001), with a mean difference of – 0.24±0.05 D, and 95% limit of agreement between −0.39 and −0.10. The mean difference between ASR and CSR was also significant (Z=−4.212, p<0.0001), with a mean difference of – 0.22±0.049 D, 95% limit of agreement between −0.35 and −0.10.
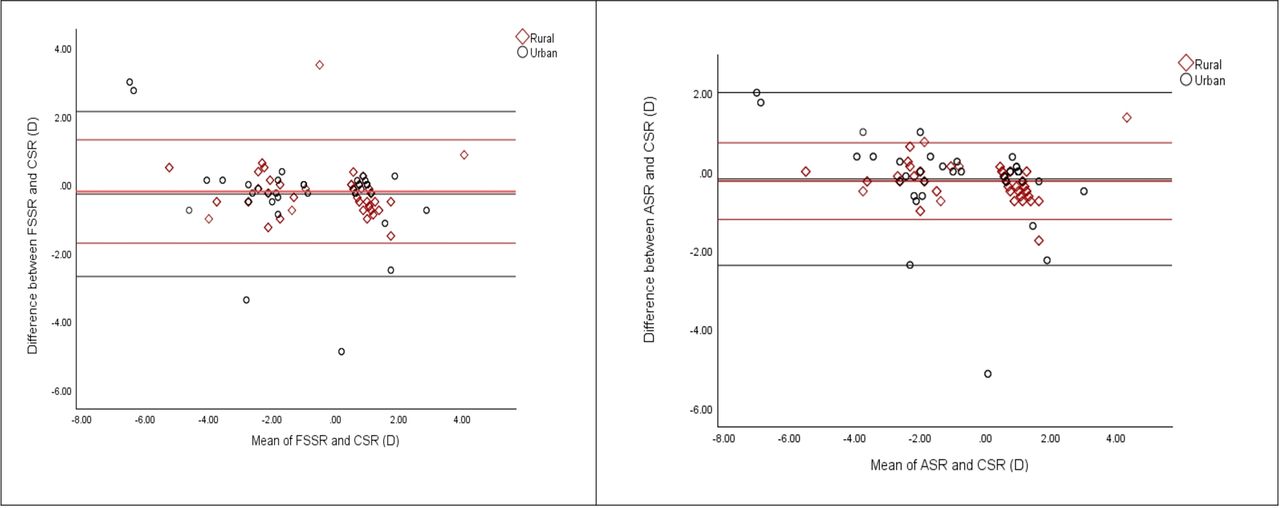
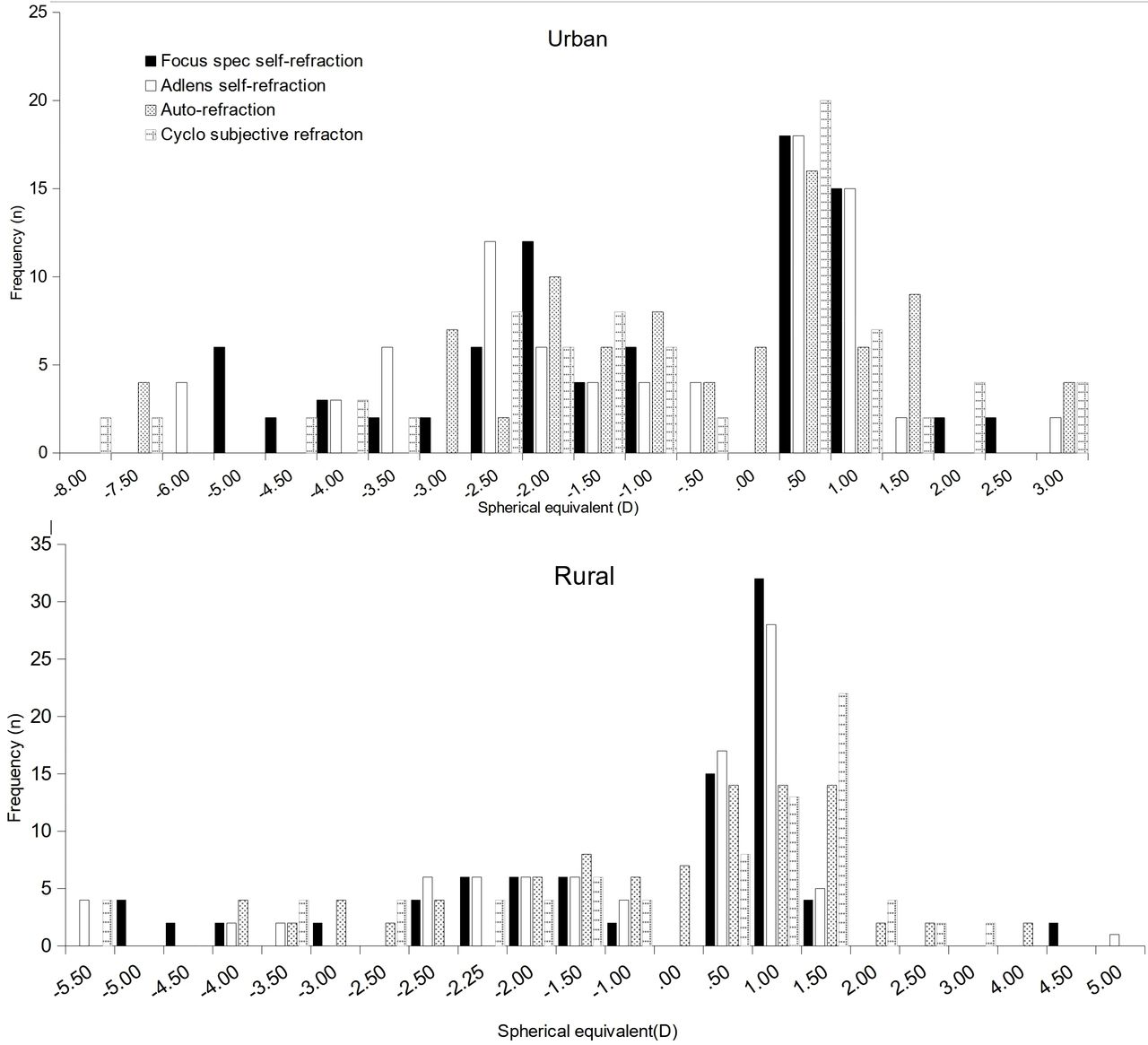
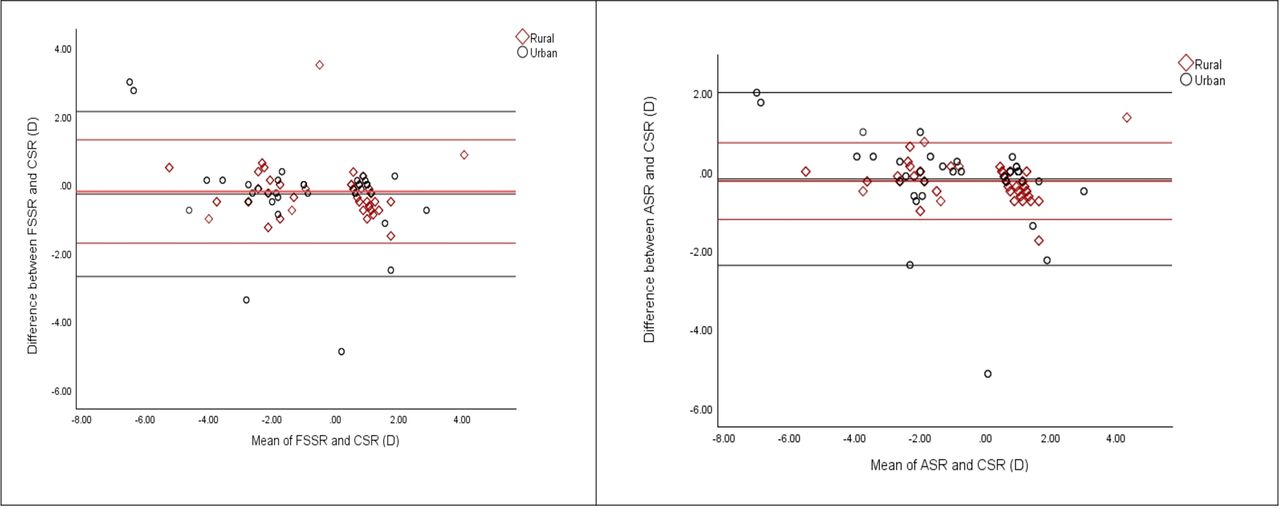
Figure 3 shows the distribution of SE refractive power indicating the range of myopia and hyperopia measured and figure 4 shows Bland-Altman plots comparing the SE refractive error of both self-refractions against CSR (as the gold standard) in right eye for children in urban and rural schools. Negative values indicate myopia and positive values, hyperopia. Overall, the mean±SD SE errors in urban schools for FSSR, ASR and CSR were −1.05±0.61 D, –0.97±0.58 D and −0.78±0.53 D while those in rural schools were −0.47±0.51 D, –0.55±0.43 D and −0.27±0.11 D, respectively. The difference between FSSR and ASR in urban schools was not statistically significant (one sample t-test, t=0.850, p=0.3966 and a 95% limit of agreement between −0.1059 and 0.2659), with a mean difference of −0.08±0.094 D. The difference between FSSR and ASR in rural schools was also not statistically significant (t=−1.119, p=0.265 and a 95% limit of agreement between −0.2212 and 0.0612), with a mean difference of −0.08±0.07 D. The difference between FSSR and CSR in urban schools was statistically significant (t=2.988; p=0.0033; 95% limit of agreement between −0.0916 and 0.4484), with a mean difference of −0.27±0.09 D while the difference between FSSR and CSR in rural schools was also statistically significant (t=3.596; p=0.0004; 95% limit of agreement between 0.0902 and 0.3098), with a mean difference of −0.20±0.06 D. The difference between ASR and CSR in urban schools was statistically significant (t=2.163; p=0.0320; 95% limit of agreement between 0.0165 and 0.3635), with a mean difference of −0.19±0.09 D while the difference between ASR and CSR in rural schools was also statistically significant (t=5.918; p<0.0001; 95% limit of agreement between 0.1866 and 0.3734), with a mean difference of −0.26±0.047 D.
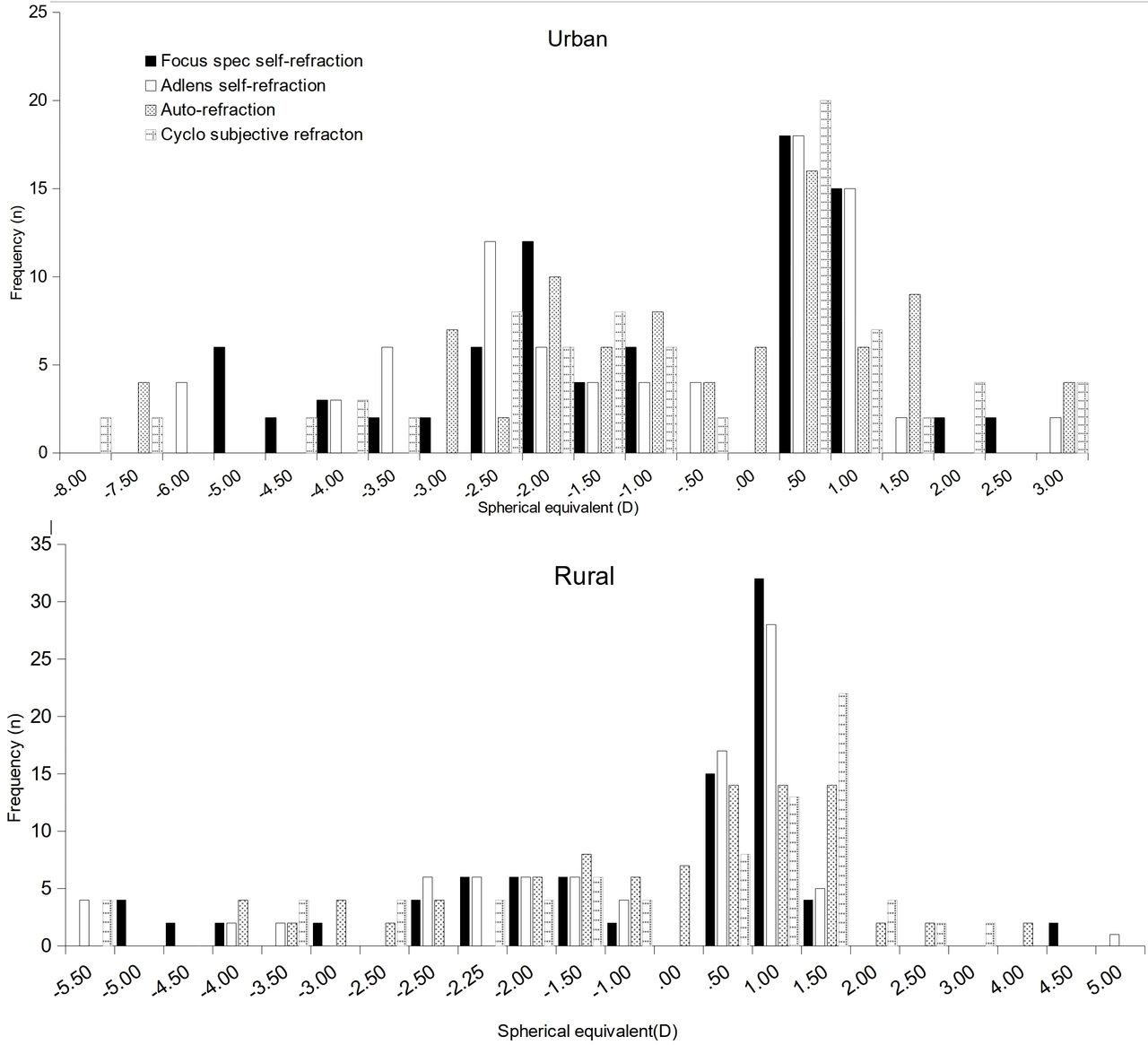
Distribution of spherical equivalent refractive among urban (top panel) and rural (bottom panel) children measured by FocusSpecs self-refraction, Adlens self-refraction, autorefraction and cycloplegic subjective refraction.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Shows Bland-Altman plots comparing the spherical equivalent refractive error of both self-refractions methods against cycloplegic subjective refractive spherical equivalent refractive error among urban (left panels) and rural (right panels) school children. Difference between the measurements is plotted on the vertical axis, and their mean is plotted on the horizontal axis. The middle horizontal line represents the mean difference and the two horizontal lines, one above and the other below, are the 95% limits of agreement between measurements. ASR, Adlens self-refraction; CSR, cycloplegic subjective refraction.
Self-refraction among myopes and hyperopes
With regard to their refractive error, the mean±SD SE refractive errors for myopes measured by FSSR, ASR and CSR among those in urban schools were −2.76±0.54 D, −2.60±0.70 D and −2.49±0.24 D, respectively. The mean difference between FSSR and ASR was not statistically significant with a mean difference of −0.16±0.07 D (t=1.609, p=0.109; 95% limit of agreement between −0.0365 and 0.3565), difference between FSSR and CSR was statistically significant with mean difference of −0.27±066 D (t=4.061, p<0.0001; 95% limit of agreement between 0.1387 and 0.4613) and the difference between ASR and CSR was not significant, with a mean difference of −0.11±0.083 D (t=1.321, p=0.188; 95% limit of agreement between −0.0545 and 0.2745). The mean±SD SE refractive errors measured by FSSR, ASR and CSR for hyperopes were +0.93±0.52, +0.93±0.51 and +1.21±0.78 D, respectively. The mean difference between FSSR and ASR was not statistically significant, 0.00±056 D (p=1.000), FSSR and CSR were statistically significant with a mean difference of 0.28±1.00 D (t=2.802, p=0.0057 and a 95% limit of agreement between −0.0828 and 0.4772) and ASR and CSR were also significant with a mean difference of 0.28±0.09 D (t=2.818, p=0.0054 and a 95% limit of agreement between 0.0839 and 0.4761).
The mean±SD SE refractive errors for myopes measured by FSSR, ASR and CSR among those in rural schools were −2.46±0.98, –2.57±0.81 and −2.47±0.32 D, respectively. The mean difference between FSSR and ASR was −0.110±0.14 D which was statistically not significant (t=−0.769, p=0.4431 and a 95% limit of agreement between −0.3926 and 0.1726), difference between FSSR and CSR was not significant, −0.010±0.12 D (t=−0.086, p=0.9314 and a 95% limit of agreement between −0.2391 and 0.2191) and ASR and CSR were not significant −0.10±0.09 D (t=1.021, p=0.3090 and a 95% limit of agreement between −0.0936 and 0.2936). While the mean±SD SE refractive errors for hyperopes among the rural children were +0.93±0.77, +0.86±0.50 and +1.29±0.68 D. The mean difference between FSSR and ASR was statistically not significant, −0.070±0.09 D (t=−0.715, p=0.4754 and a 95% limit of agreement between −0.2632 and 0.1232), FSSR and CSR were significant, −0.36±0.11 D (t=3.287, p=0.0012 and a 95% limit of agreement between −0.1439 and 0.5761) and ASR and CSR were also significant, −0.430±0.09 D (t=4.779, p=0.0001 and a 95% limit of agreement between 0.2524 and 0.6076).
Discussion
A number of studies13 17 23 have indicated that a range of good refractive results and VA were achievable with self-refraction in children although variations in the results reported. The discrepancies in the accuracy of self-refraction reported in their results may be attributed to several factors including the background and refraction experience of the subjects. The current investigation was, therefore, carried out to assess the accuracy of two commonly available self-refraction spectacles in urban and rural school children in the Central Region of Ghana.
The distribution of refractive error among the study population showed that myopia was more common in urban children (54.4%), while hyperopia was more common in rural children (58.0%). The differences in the prevalence of refractive error could be attributed to modern lifestyle activities, especially near work with technological devices (eg, computers, laptops, phones and video games) which may cause myopia. On the other hand, less access to activities with demanding near visual activity and nutritional changes in rural children may predispose them to hyperopia.24 25
The results from this study indicate that while the differences in refractive power achieved with the two Alvarez spectacles were not different from each other they were appreciable when compared with the traditional clinical gold standard of refraction in children (ie, CSR). The refractive results from both self-refractions also differed from refraction obtained with autorefraction. The refractive results from both self-refractions also differed from refraction obtained with autorefraction. The results are consistent to a previous study conducted on Chinese children16, which found differences in the methods and reported that SE differed by 1.0 D in either direction from CSR, which was more frequent for self-refraction (11.2%) than non-cycloplegic autorefraction (6.0%). In a study conducted in Ghana among myopes,17 it found that the mean SE refractive error measured by CSR and self-refraction were significantly different by −0.44 D. The study found that more children undercorrected or overcorrected their myopia greater than 0.50 D (15.3%) and greater than or equal to −1.00 D (8.4%) with self-refraction using FocusSpec.
The finding in this study is also consistent with previous studies which indicated that there was a higher propensity for some of the children to either undercorrect or overcorrect their refractive errors by self-refraction, as indicated by relatively high SD. For instance, about 4% and 3% (translating to about six individuals) of the children undercorrected and overcorrected their myopia with FocusSpec, respectively, while about 7% of the children undercorrected or overcorrected the refractive errors over the clinical subjective values using Adlens. Correspondingly, the visual outcomes determined by CSR were better than those by self-refraction, as the former gold standard method included correction for existing astigmatism.17
The results also showed that generally, there were no statistically significant differences in mean SE refractive value correction between the two self-refraction devices in urban and rural children, with negligible mean differences. However, when compared with the clinical standard, the mean differences between FSSR and CSR in urban (−0.27±0.09 D) and rural (−0.20±0.06 D) children were significant. Similarly, there were statistically significant differences in mean SE refractive values between ASR and CSR in urban (−0.19±0.09 D) and in rural (−0.26±0.047D) children. These results revealed that difference in refractive error correction using the two Alvarez self-refraction methods was not different in both urban and rural children. However, when compared with cycloplegia subjective refraction, the refraction differed for all methods in urban and rural children. This finding is similar to previous studies that also reported differences in refractive outcomes between self-refracting methods and clinical standard of CSR due to mechanical and optical limitations of adjustable glasses.18 23 25–27 The results, however, are contrary to suggestions that children from less socioeconomic background are less likely to accurately perform self-refraction compared with their counterparts from more privileged backgrounds.17 It is suggested that children from less resourced environments, who are likely not to habitually wear spectacles were at greater risk for less accurate results with adjustable glasses possibly because such children are more tolerant of imperfectly corrected VA and were thus less inclined to carefully adjust the SRSs until optimal VA had been achieved.17 18
In addition, in this study, the findings revealed that refractive correction using the two self-refraction spectacles were similar and produced similar SE refractive values within acceptable margins of optical error for Alvarez designs,28–30 irrespective of the background of the end user. This was despite the fact that the study found low spectacle wear among the children, with only about a quarter of the study population reporting wearing spectacle, and nearly two-thirds (72.5%) of those wearing spectacles were from urban areas compared with slightly over one-third (27.5%) of rural children. The finding does not support our presumption that refraction and spectacle wear experience could influence self-refraction regarding appreciation of power changes.
On the other hand, the finding observed could be associated with the relative ease of manipulating the two adjustable devices, even though the styles of manipulating the adjustable are different. In performing self-refraction, the instruction for FocusSpec requires scrolling the wheel to adjust the lens power, with about 2.5 turns of the adjustment screw producing a 4D power change. That translates to a setting accuracy of 0.25 D which corresponds to screw scrolling of about 60°. On the other hand, Adlens design requires dialling or twisting the wheel on the sides to adjust the lens power, with about five complete rotations producing a 9.0 D power change. That translates to a setting accuracy of 0.25 D corresponding to screw rotations of about 50°.29 These angular rotations are quite large so that, from the purely mechanical point of view, no great skill is required when adjusting the lens powers. This perhaps explains why there was no significant difference in results among the children in adjusting for the lenses, by dialling or twisting the wheel on the sides to the Adlens adjustable or scrolling the wheel on the sides of the FocusSpec adjustable to recognise changes in refractive power. The results also revealed that refraction among myopes from both urban and rural schools across all refraction methods were statistically not significant, but there were statistically significant differences in mean SE refractive value obtained in hyperopes from both urban (FocusSpec and CSR, −0.28 D; Adlens and CSR, −0.28 D) and rural schools (FocusSpec and CSR, −0.35 D; Adlens and CSR, −0.38 D). This finding perhaps indicated that the children easily appreciated differences in minus correction than spherical blur plus corrections. Indeed, inspection of that data showed that myopes from urban schools tended to over minus with self-refraction compared with rural children, with the over minus more with FocusSpec (more myopic) than with Adlens.
Although a comparison of the distribution of refractive error values obtained is an easier, simple and objective way to compare the refractive modalities, the range of visual acuities achieved is in many ways of greater clinical significance. Inspection of the VA outcomes after refraction showed that the proportion of urban children who achieved VA of ≥6/7.5 for all refraction methods were more than rural children, except CSR. In percentage terms, 11%, 6.2% and 6.0% more urban children obtained better VA with FocusSpec, Adlens and autorefraction, respectively, than in rural children. For urban children, when the self-refraction methods were compared against each other and to the clinical gold standard, there was no difference in the proportions who achieved the expected VA of ≥6/7.5 in urban schools. In contrast, for rural schools, the proportion of children failing to achieve VA of ≥6/7.5 with both self-refractions differed significantly from each other (<5%), and from the proportion failing to achieve the same VA with CSR for FocusSpecs (13.8%) and Adlens (9.2%). Self-refraction outcome was, however, better when autorefraction results are compared with results of CSR in urban (32.6%) and rural children (41.4%) or to FocusSpec (32.6%; 27.6%) and Adlens (32.4%; 32.2%) self-refractions in urban and rural children, respectively. The results further showed that more urban school children achieved VA of ≥6/7.5 with both types of self-refraction devices compared with rural children. Improvement in worse VA was better in urban school children across all methods. Indeed, this study is the first to report on the refractive and visual outcome among rural and urban children in the same study, other studies have reported in urban15 and rural16–18 30 31 children separately.
While greater proportions of children that achieved desired visual acuities have been reported elsewhere,15–17 the proportion that achieved VA of ≥6/7.5 in this study is consistent with findings in urban15 and rural children.16 In reported studies in China using Adspecs self-refraction spectacles (fluid-filled lenses of refractive index 1.579) found the proportion of urban children with VA of 6/7.5 in the better eye with habitual correction, self-refraction, non-cycloplegic autorefraction and CSR were 34.8%, 92.4%, 99.5% and 99.8%, respectively, while another study among rural children found the proportion with similar VA to be 5.2% for uncorrected vision, 30.2% for currently worn spectacles, 96.9% for self-refraction, 98.4% for automated refraction and 99.1% for subjective refraction.15 16 In Ghana, a previous study in Ghana in myopic school children indicated that the proportion of children correctable to greater than or equal to 6/7.5 in the better eye by CSR was 99.0%, followed by cycloplegic retinoscopy (94.1%) and self-refraction was 85.2%.18 It must be noted that while the proportion of rural and urban school pupils in China who achieved the desired VA with self-refraction and clinical standards were similar, the study in Ghana found substantial difference in VA outcomes between the refractive methods, perhaps due to refraction experience of the subjects used. While the findings on the value of SE is consistent with other studies, and relatively similar for both self-refraction devices used, the difference in the visual outcome between rural and urban may be due to differences in refraction experience. In China, both rural and urban children may have relatively better access to refractive services, and therefore, have comparable refraction experience.
The results and the implications of this study must be understood within the context of its limitations. As indicated, self-refraction spectacles are incapable of correcting high astigmatism, which resulted in the exclusion of children with high astigmatic error from the study. Again, the limits of spherical correction for FocusSpecs are +0.50 to +4.50 and −1.00 to −5.00 D, and+3.00 to −6.00D for Adlens meant that the devices could not be used to correct very high amount of refractive errors. This may have resulted in failure to achieve ≥6/7.5 as seen in some cases. A larger sample size could have resulted in greater percentages of agreements with more predictive power. In addition, a reliability study using intraobserver measurement (test, retest) and interobserver measurement was not performed due to the time and scheduling constraint as the study was performed during school hours. Despite the study’s limitations, the results here are able to provide previously unavailable comparative data on the potential use of different self-refraction spectacles to improve vision in young people in urban and rural schools who carry a considerably large burden of inadequately corrected refractive error. The findings also show that self-refraction produces better refractive and visual outcome than that of autorefraction, which seems to indicate that their results may be less prone to accommodative inaccuracy than non-cycloplegic autorefraction,15 another modality advocated for use in areas where access to eye care providers is limited.
Conclusion
The study revealed that the background and refraction experience of school children did not significantly affect self-refraction, however, the results differed when compared with the clinical standard in urban and rural schools. For the visual outcome, the results revealed that, there was no difference in the proportion of children who obtained the desired VA with both self-refraction and the clinical standard in urban children, but the proportion that obtained the desired VA significantly differed among rural schools. The results indicate that both self-refraction devices are capable of achieving acceptable refractive accuracy and VA outcomes in children from low-resourced environment, but an easier mechanism of self-adjusting the spectacles must be taken into account to match clinical standards and ensure high wearing compliance.
Data availability statement
Data are available on reasonable request. Data are available on reasonable request. The datasets used and analysed during the current study are available from the corresponding authors on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted according to the Tenets of the Declaration of Helsinki and ethical approval obtained from the Institutional Review Board of the University of Cape Coast (UCCIRB/CHAS/18/62). Permission to conduct the study was also approved by the Central Regional Education Directorate for use of the schools involved in the study.
References
Footnotes
Twitter @ocansity
Contributors SO conceived the study. SO, CHA, RA and EKA designed this study. SO and RA screened and did the data collection. RA and CHA did literature search. SO, RA, CHA and EKA did the data analysis and interpretation. SO drafted the manuscript, and CHA and EKA did proofread of the manuscript. SO is the corresponding author and is responsible for the overall content as guarantor. All authors approved this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.