Article Text

Abstract
Introduction As the rates of age-related macular denegation exponentially increase, new innovation is required to address the challenges faced by our ageing population. The aim of the Palmerston North Interventional Rapid Avastin Treat and Extend (PIRATE) study is to establish the safety and efficacy of rapid treatment extension of bevacizumab (Avastin) in patients with low-risk neovascular age-related macular degeneration (nAMD).
Methods and analysis The PIRATE study is a monocentric, non-blinded, open-label randomised control trial. Participants over the age of 50 years with low-risk nAMD characteristics will be recruited in a prospective manner and randomised into treatment and control groups. Rapid treatment extension by 4 weeks will be applied in the treatment group, with the standard 2-week treatment extension occurring among controls. Participants will enter the trial after initial treatment induction consisting of three bevacizumab injections, 1 month apart. The primary outcome of best-corrected visual acuity will be assessed along with predetermined secondary outcomes at a study duration of 12 months (initial) and 24 months (total).
Trial registration number ACTRN12622001246774p.
- Vision
- Retina
- Macula
- Clinical Trial
Data availability statement
No data are available. No data is currently available at time of publication.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Support for the Palmerston North Interventional Rapid Avastin Treat and Extend (PIRATE) study protocol has been established by previous large interventional trials including the ALTAIR and ARIES studies, with safe and efficacious results of rapid treatment extension in patients with low-risk neovascular age-related macular degeneration (nAMD).
WHAT THIS STUDY ADDS
What is unique about the PIRATE study is that bevacizumab (Avastin) is being used, which is the approved first-line antivascular endothelial growth factor agent in Australasia, in comparison to aflibercept (used in both the ALTAIR and ARIES studies).
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The PIRATE study presents an innovative solution to increase medical retina service capacity in the face of resource limitation to address the disease burden of our ageing population. If determined to be safe and efficacious, patients with low-risk nAMD may receive fewer injections, fewer clinic appointments and fewer injection-related side effects while still maintaining their visual outcomes.
Introduction
Age-related macular degeneration is the primary cause of blindness in individuals over the age of 50 years in high-income countries.1 Intravitreal antivascular endothelial growth factor (VEGF) therapy has become the standard treatment for individuals with neovascular (exudative) age-related macular degeneration.1 Once commenced on anti-VEGF therapy, individuals with neovascular age-related macular degeneration (nAMD) require frequent monitoring and sequential treatment to prevent debilitating central visual loss. As the prevalence of AMD is projected to increase over the next 10 years, national healthcare delivery and individual ophthalmology services face a significant disease burden.2 The Palmerston North Interventional Rapid Avastin Treat and Extend (PIRATE) study presents an innovative method of addressing challenges posed by our ageing population. If deemed safe and efficacious, the rapid extension of treatment intervals may reduce patients’ treatment burden and increase service capacity within current health infrastructure while still maintaining visual outcomes.
Methods and analysis
The PIRATE study protocol has been established according to the Standard Protocol Items: Recommendations for Intervention Trials (SPIRIT) checklist.
Study objectives
The purpose of the PIRATE study is to establish the safety and efficacy of bevacizumab rapid treatment extension in treatment-naïve patients with low-risk nAMD. Direct comparison of rapid treatment extension (4 weeks) to the standard protocol (2 weeks) will be made with respect to measured visual outcomes. Secondary objectives will be assessed around the impact on local medical retinal service capacity with the proposed changes to practice.
Study design
The PIRATE study is designed as a monocentric, interventional randomised control trial. It will be open-label and non-blinded. Participants will be recruited prospectively based on predetermined inclusion criteria. All participants will be provided with 0.05 mL bevacizumab 3.75 mg/0.15 mL. This will be administered into the vitreous cavity by either nurse injectors or ophthalmology registrars/ophthalmologists observing sterile aseptic technique. Injection frequency and follow-up intervals will be criteria-led and study group-specific.
Eligibility criteria
The diagnosis and risk-stratification of nAMD will be based on clinical and optical coherence tomography (OCT) parameters. Ocular angiography will not be implemented for subclassifcation purposes due to practice resource limitation. Participants with low-risk nAMD will be recruited based on predetermined inclusion criteria. The following criteria must be met for study inclusion:
Age: adult patient of ≥50 years.
Low-risk nAMD characteristics (see further for risk stratification).
Best-corrected refracted visual acuity between 6/9 and 6/120 at first specialist assessment. Note that if both eyes are affected, then the poorer eye will be included as the study eye.
Deemed appropriate for bevacizumab by investigator(s).
Willing and able to provide independent informed consent for study inclusion.
Participants who fulfil any of the criteria listed as follows will be excluded from the study:
Prior treatment in the study eye (including intravitreal anti-VEGF/corticosteroid, verteporfin photodynamic therapy, focal retinal laser and ocular surgery within last 3 months).
Active or suspected intraocular/periocular infection.
Peripapillary choroidal neovascular membrane.
Raised intraocular pressures of ≥28 mm Hg in the treatment eye.
Alternative primary or secondary ocular condition that can confound study results (under the discretion of the study investigators).
Contrainidication to bevacizumab intravitreal injection (eg, allergy, recent cerebrovascular accident (CVA) or myocardial infarction (MI) in the last 3 months).
Any other participant deemed ineligible by the study investigator(s).
Participants will be stratified based on the nAMD characteristics. High-risk participants will be deemed anyone who meets one or more of the following criteria:
Monocularity (ie, only have single-sighted eye).
Macular haemorrhage ≥1 disc diameter (DD).
Subretinal fluid of ≥200 µm.
A low-risk participant is deemed anyone who meets the inclusion criteria without having any of the high-risk characteristics stated previously. High-risk participants will be excluded from recruitment into the PIRATE study.
Methodology
Low-risk participants who meet the inclusion criteria and consent to participation will be randomly allocated to either the treatment group or the control group. Randomisation will be conducted using block randomisation with a block size 0f 4. Group randomisation will occur after completion of the treatment induction. The treatment group will undergo treatment extension at 4-week increments. The control group will undergo treatment extension of 2-week increments, as per the current standard protocol.3 The relative treatment protocols will commence following induction treatment consisting of three bevacizumab injections at a 4-week interval (figure 1).

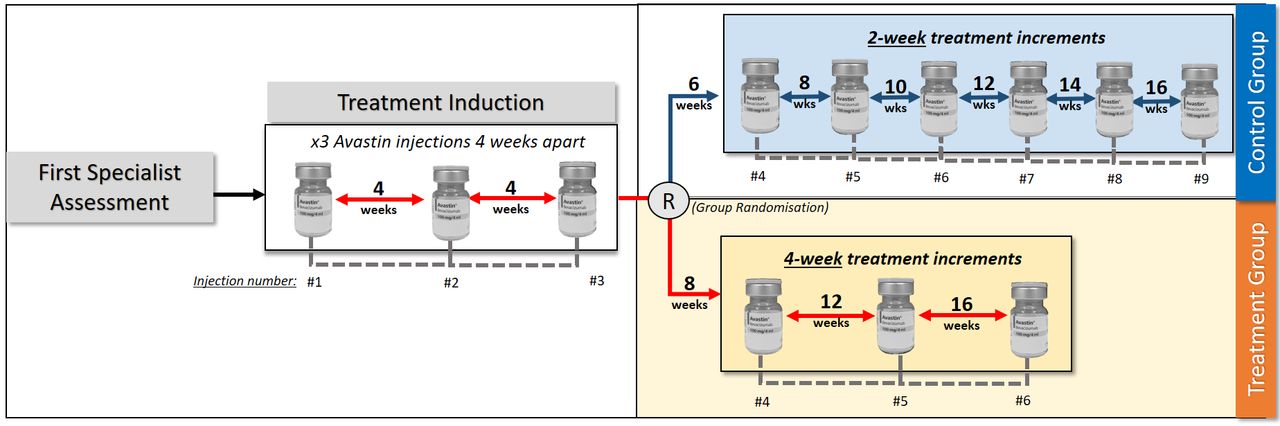{kind=link}
Proposed treatment regimen of study groups.
Close monitoring through regular clinical assessment by ophthalmologists and/or ophthalmology registrars will be supplemented by OCT for each treatment extension. Each adjustment to a participant’s treatment interval will be criteria-led with predetermined extension, shortening and maintenance criteria (table 1). If any one of the shortening criteria is met for a participant, the interval will be reduced by 4 weeks (to a minimum of 4-week treatment interval), and all subsequent interval extensions will be at 2-week increments as per the standard protocol. The standard protocol will be in accordance with the Royal Australia and New Zealand College of Ophthalmologists best practice guidelines for nAMD management.3 A maximum treatment interval of 16 weeks will be maintained, ensuring fluid-free macula status and no shortening criteria is met. An intention-to-treat analysis will be implemented for anyone who is lost to follow-up or exits the study for any reason.
Criteria-led approach for interval shortening, extension treatment maintenance
Study outcomes
The primary outcome measure will be best-corrected refracted visual acuity at end of study periods. Best-corrected refracted vision will be collected at all consultation visits. Secondary outcome measures will include central macular thickness, number of adverse injection-related events, whether treatment interval had to be shortened, number of large macular haemorrhages (≥1 DD), total number of injections and total number of age-related macular degeneration-related appointments. No human tissue will be collected as part of the PIRATE study.
Study size and data collection periods
Prospective trial recruitment will occur over an initial 12-month period with total study duration being 24 months. Database auditing and analysis will be conducted to assess treatment safety, efficacy and impact on visual outcomes after 12 months. At the time of writing, no study participants have yet been recruited. Internal auditing has demonstrated an incidence of 80 nAMD cases annually within the regional ophthalmology service with a 20%–30% incidence increase each year from 2019. Our power calculation for sample recruitment size assumes a predefined type I error rate (α) of 0.05. The type II error rate (β) was set at 0.80. A standard difference of 0.60 was calculated from internal auditing data from our institution. Using Altman’s nomogram, a sample size of 90 participants was calculated to achieve statistically significant results. 4 Primary and secondary outcome measures will be summarised descriptively with the use of frequency tables and categorical numerical values.
Support for the PIRATE study protocol
New methods to reduce injection frequency in patients with nAMD have been researched extensively. The ALTAIR and AIRES studies are two recent, large-scale, randomised controlled trials supporting rapid treatment extension with safe and efficacious results.5 6 Both trials used aflibercept (Eylea) as their therapeutic anti-VEGF agent in treatment-naïve patients with nAMD. They had similar randomised open-label methodology and best-corrected visual acuity endpoints. The ALTAIR study was based solely in Japan, while the ARIES study was a multicentric study spanning eight countries (Australia, Canada, France, Germany, Hungary, Italy, Spain and the UK).5 6 Comparisons between treatment extension of 2 weeks and 4 weeks were provided by both, following initial three, one-monthly, induction treatment. Both trials demonstrated similar functional and anatomical outcomes between study groups with consistent safety profile.5 6 In New Zealand, bevacizumab is the first-line, publically funded, anti-VEGF treatment choice for nAMD, while Eylea is reserved mostly for bevacizumab non-responders. The PIRATE study methodology mirrors that of the ALTAIR and AIRES studies5 6 but is tailored to a New Zealand centric population and treatment selection.
Importance and clinical impact
The introduction of anti-VEGF therapy has revolutionised the safety and efficacy of nAMD treatment superseding previous historic treatments such as retinal photocoagulation and verteporfin photodynamic therapies. This, however, has come at a huge economic cost. Once anti-VEGF treatment is commenced, regular follow-up and subsequent intravitreal injections are required to prevent irreversible central visual loss. Anecdotally, in Palmerston North, we found patients with low-risk nAMD to have maintained visual outcomes while inadvertent treatment delays occurred during the COVID-19 lockdowns of 2020. As supported by the ALTAIR and ARIES trials,5 6 it appears this select nAMD subgroup demonstrate disease factors suitable to rapid treatment extension.
According to the Ministry of Health’s National Health Committee 2015 report, the number of bevacizumab injections has increased threefold to fivefold in the last 5 years at an almost $8 million (NZD) public health cost.2 It is further estimated that 50%–75% of all bevacizumab injections received nationally are for nAMD.1 In the PIRATE study, treatment group participants are expected to require 3 fewer injections to reach a maximum 16-week treatment interval, reaching this target 6.5 months sooner, assuming expected treatment response. This would result in cost saving of $279.22 (NZD) per patient in pharmaceutical consumables alone.7 Further savings would result from injection-related overhead, administration and labour costs. In addition, this initiative would ensure patients with high-risk nAMD are not needlessly delayed due to the increasingly resource-constrained environment. There would also be an indirect beneficial effect on increased service capacity for other primary ocular diseases dependent on anti-VEGF therapy such as diabetic eye disease and retinal vein occlusions in which indigenous Māori groups are commonly over-represented.
A new Food and Drug Administration-approved agent, faricimab-svoa (Vabysmo, Genentech), further presents a promising advancement in nAMD treatment.8 Although not yet approved for use in New Zealand, large multinational phase III trials have demonstrated efficacious results in the treatment of both nAMD and diabetic macular oedema. In the TENAYA and LUCERNE studies, patients with nAMD maintained visual outcomes with treatment extensions up to 4 months.9 The current cost of faricimab is US$2190 ($3469.73 NZD) per unit dose (Roche).7 ⇓Even with the promising early results, bevacizumab is likely to remain the first-line therapy in New Zealand for the foreseeable future due to its efficacy, safety and low unit cost until faricimab approval is obtained. Furthermore, this approval process is typically long and protracted.
One limitation anticipated is the impact of the monocentric nature of the PIRATE study with respect to patient recruitment numbers. An extended study duration of 24 months has been employed to reach the intended participant recruitment required for statistical power. The generalisability of a regional patient demographic may not be entirely representative of New Zealand’s complete ethnic diversity. The data and results, however, would aid and promote further research in this area.
The results of the PIRATE study will provide invaluable data on resource allocation, service planning and standard care in treatment extension of nAMD. This protocol outlines the intended study aims, methodology and outcomes and provides the reader with an anticipation for the study results and conclusions to follow.
Data availability statement
No data are available. No data is currently available at time of publication.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval has been granted by the Northern B Health and Disability Ethics Committee, New Zealand through the FULL pathway. Ethical approval was granted on 3 October 2022. The Palmerston North Interventional Rapid Avastin Treat and Extend (PIRATE) study has been thoroughly examined for robust methods and the highest ethical standards. An in-depth data management plan has been established in accordance with the National Ethics Standards of the National Ethics Advisory Committee (NEAC). Data will be collected in accordance with the Health Information Privacy Code 2020. Informed consent will be obtained before study inclusion and data recording of participants. All health data collected will be protected with confidentiality, except in exceptional circumstances as outlined by the NEAC standard guidelines. No data linking, internally or externally, to the study is intended to be conducted. Data collected during the PIRATE study may be used for future analyses at the discretion of the principal investigators and project management group. Health governance accessibility within the PIRATE study will comply with the indigenous people of New Zealand and Māori data sovereignty principles (Te Mana Raraunga). Māori will have the opportunity to exercise control of their own data and self-determination. The Kaupapa Māori principles, as first described by Graham Higangaroa Smith in 1990, will be acknowledged. Individuals will have the option to withdraw from the study at any time without treatment or financial repercussions.
Acknowledgments
The authors recognise with gratitude the contributions of the ophthalmology department
of Palmerston North, including its nursing, medical, administrational and IT staff.
Footnotes
Contributors Primary authorship for the Palmerston North Interventional Rapid Avastin Treat and Extend (PIRATE) study is credited to Dr. Louis Antoine Bonnet. Dr. Vidit Singh and Dr. John Ah-Chan are recognised as contributory authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.