Article Text

Abstract
Introduction In ophthalmology, clinical trials (CTs) guide the treatment of diseases such as diabetic retinopathy, myopia, age-related macular degeneration, glaucoma and keratoconus with distinct presentations, pathological characteristics and responses to treatment in minority populations.
Reporting gender and race and ethnicity in healthcare studies is currently recommended by National Institutes of Health (NIH) and Food and Drug Administration (FDA) guidelines to ensure representativeness and generalisability; however, CT results that include this information have been limited in the past 30 years.
The objective of this review is to analyse the sociodemographic disparities in ophthalmological phases III and IV CT based on publicly available data.
Methods This study included phases III and IV complete ophthalmological CT available from clinicaltrials.org, and describes the country distribution, race and ethnicity description and gender, and funding characteristics.
Results After a screening process, we included 654 CTs, with findings that corroborate the previous CT reviews’ findings that most ophthalmological participants are white and from high-income countries. A description of race and ethnicity is reported in 37.1% of studies but less frequently included within the most studied ophthalmological specialty area (cornea, retina, glaucoma and cataracts). The incidence of race and ethnicity reporting has improved during the past 7 years.
Discussion Although NIH and FDA promote guidelines to improve generalisability in healthcare studies, the inclusion of race and ethnicity in publications and diverse participants in ophthalmological CT is still limited. Actions from the research community and related stakeholders are necessary to increase representativeness and guarantee generalisability in ophthalmological research results to optimise care and reduce related healthcare disparities.
- Public health
- Epidemiology
- Clinical Trial
Data availability statement
Data are available upon reasonable request. All the data used in this article is available at www.clinicaltrials.org. All the article data are available under request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Fairness and generalisability are limited in medical clinical trials (CTs), with National Institutes of Health and Food and Drug Administration efforts to address this limitation.
WHAT THIS STUDY ADDS
This study is the first to analyse the sociodemographic disparities in ophthalmological CTs, with the findings that most ophthalmological participants are white and from high-income countries.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study confirms the limited fairness and generalisability in ophthalmological CTs, with more efforts needed to address this problem.
Introduction
Generalisability in medical research is contingent on patient cohorts being representative of the populations in which the findings will ultimately be clinically applied.1 To promote generalisability, the National Institutes of Health (NIH) 1993 guidelines recommend that research publications include gender and race and ethnicity to determine whether there is adequate diversity in the study participants.2 Since 2012, the Food and Drug Administration (FDA) has also implemented recommendations to improve the representation of such subgroups.3
Clinical trials (CTs) require adherence to strict regulations and represent a benchmark for ethical research in medicine.4 While pre-CTs (phases I and II) promote safety for human subjects, phase III trials apply treatments to larger populations and trials in phase IV evaluate the results after FDA approval, identifying adverse reactions and cost-effectiveness.4
An appreciation of the global socioeconomic burden of preventable and treatable causes of vision loss has driven an increasing number of ophthalmological trials in recent years.5 Currently, CTs guide treatments in areas such as diabetic retinopathy, glaucoma and corneal infection, but few address the possible sociodemographic bias (and subsequent limitations to generalisability) embedded in these studies due to suboptimal representation of certain populations that are in facts the ones most often affected.
Common ophthalmological diseases such as diabetic retinopathy,6 myopia,7 age-related macular degeneration, glaucoma8 and keratoconus9 can have distinct presentations, pathological characteristics and responses to treatment across different populations. Coupled with the under-representation of minority subgroups in ophthalmological CTs and the consequent limited generalisability of results, the impact of socioeconomic inequality becomes even more pronounced.10
The objective of this review is to analyse the sociodemographic disparities in ophthalmological phases III and IV CTs based on publicly available data.
Material and methods
This review included data from CTs in ocular diseases publicly available on clinicaltrials.org.11
We extracted data including (1) national clinical trial (NCT) number, (2) number of participants, (3) gender, (4) ophthalmological specialty area addressed, (5) funding, (6) race, (7) country of the study participants and (8) completion date, as of 5 July 2022.
Inclusion and exclusion criteria
We included CTs with (1) ophthalmology theme, (2) any language and (3) without date restriction, and excluded (1) non-ophthalmological studies, (2) ongoing trials, (3) with non-available results and (4) studies in phases I and II.
The searched terms and phrases included ‘ophthalmological disorder’, ‘ophthalmological’ and ‘ocular disorder’; these the synonyms ‘eye disease’, ‘ophthalmopathy’, ‘eye disorder’, ‘disease of the eye’, ‘ophthalmic disorder’, ‘oculopathy’, ‘disease’, ‘condition’, ‘diagnoses’, ‘eye’, ‘vision’, ‘ophthalmic’, ‘optic’, ‘visual function’, ‘sees’, ‘sight’, ‘visual perception’, ‘oculus’, ‘seeing’, ‘ophthalmology’ and ‘optometry’.
This review considered the NIH racial categories.12 Although many CTs include Hispanic or Latino as a race classification, according to the NIH, it is an ethnic category and was not considered in this review.
Regarding ophthalmological specialties, the CTs were classified as cataract, cornea, glaucoma, retina, oculoplastic, neuro-ophthalmology, strabismus, refractive error, uveitis, oncology and paediatrics.
For funding source, the CTs were classified as supported by industry, the NIH or other.
When the extracted data were unavailable in the clinicaltrials.org online database, information from the publications indexed with the same ClinicalTrials.gov Identifier (NCT number) was included.
The World Bank’s income level was considered in the country’s classification according to the gross national income (GNI) per capita (low income—GNI per capita of US$1085 or less, lower-middle income—GNI per capita of US$1086 to US$4255, an upper-middle income—GNI per capita of US$4256 to US$13 205 and high income—GNI per capita of US$13 205 or more).13
Results
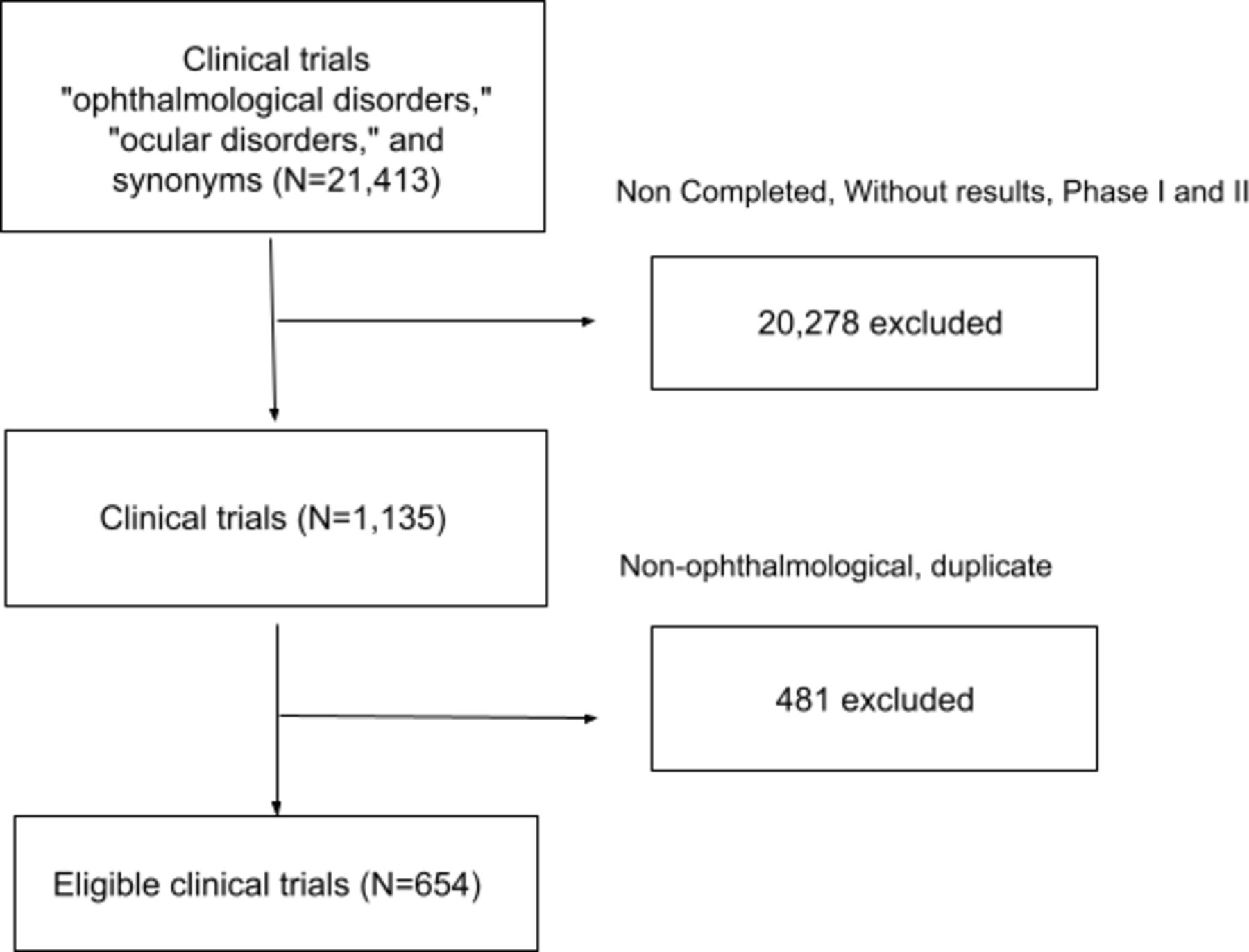
A total of 21 413 trials were identified by the search terms ‘ophthalmological disorders’, ‘ophthalmological’, ‘ocular disorder’ and their synonyms. A total of 20 239 trials were excluded for not falling within our phase III or IV trial criterion, leaving 1174 eligible trials. After analysis, 520 non-ophthalmological and duplicated articles were excluded, with 654 CTs included in the final review from 1990 to 2022 (figure 1).

Flow diagram of inclusion and exclusion.
General characteristics of studies and participants
Within the CTs, 93 421 patients were male (47.0%); in 3, gender was not identified.
In the analysis of the countries involved, a total of 69 countries were represented, with the most common being the USA (455), Germany (75), Canada (68), the UK (65) and France (62), with the top 11 of the 69 classified as high-income countries.
In 84% of the CTs, the study population came from high-income countries, with 10.7% from upper-middle-income, 4.2% from lower-middle-income and 0.2% from low-income countries.
Ophthalmological classification
Among the 654 CTs studied, the most frequent specialty areas involved the cornea (194), retina (171), glaucoma (141) and cataracts (68). A description of race was less frequent in these four ophthalmological specialties (cornea, retina, glaucoma and cataracts) and more frequent in the remaining seven (uveitis, refractive error, oculoplastic, neuro-ophthalmology, paediatrics, oncology and strabismus) (figure 2).
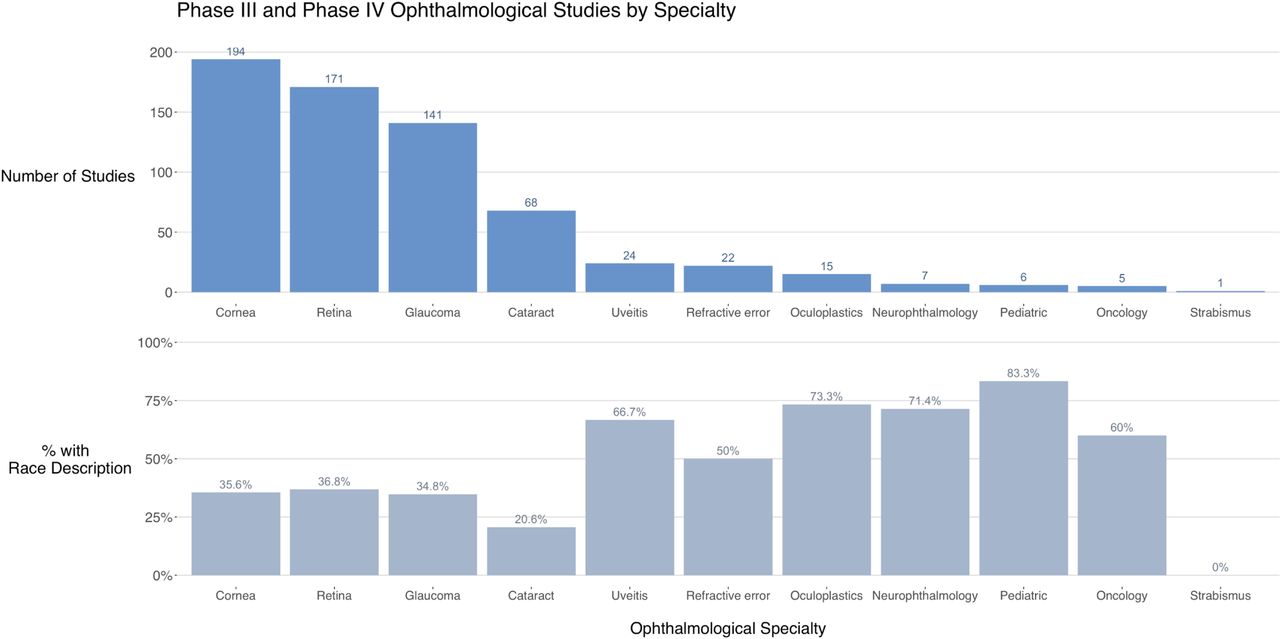
Ophthalmologic specialty distribution and percentage with race description.
Race characteristics
In 37% of the CTs, race was described. The number of studies that did not describe race of the participant was higher in 2012 and decreased through the years, with 76% of the completed CTs in 2021 through July 2022 including race descriptions (figure 3).

Percentage of ophthalmologic clinical trials with race description by year and the number of studies (n).
Among studies with at least 1 US location, race was described in 52.57% of studies, and in studies outside the USA, race was described in 19.77%.
The most frequent race was white (77.7%), followed by black (10.9%), Asian (7.9%), other (1.7%), unknown/not reported (1.4%) and American Indian (0.4%).
Regarding race distribution, retina trials had the most numerous white, asian and unknown/not reported races. Glaucoma trials had the most numerous black patients, and cornea trials had the largest frequency of other race.
Funding characteristics
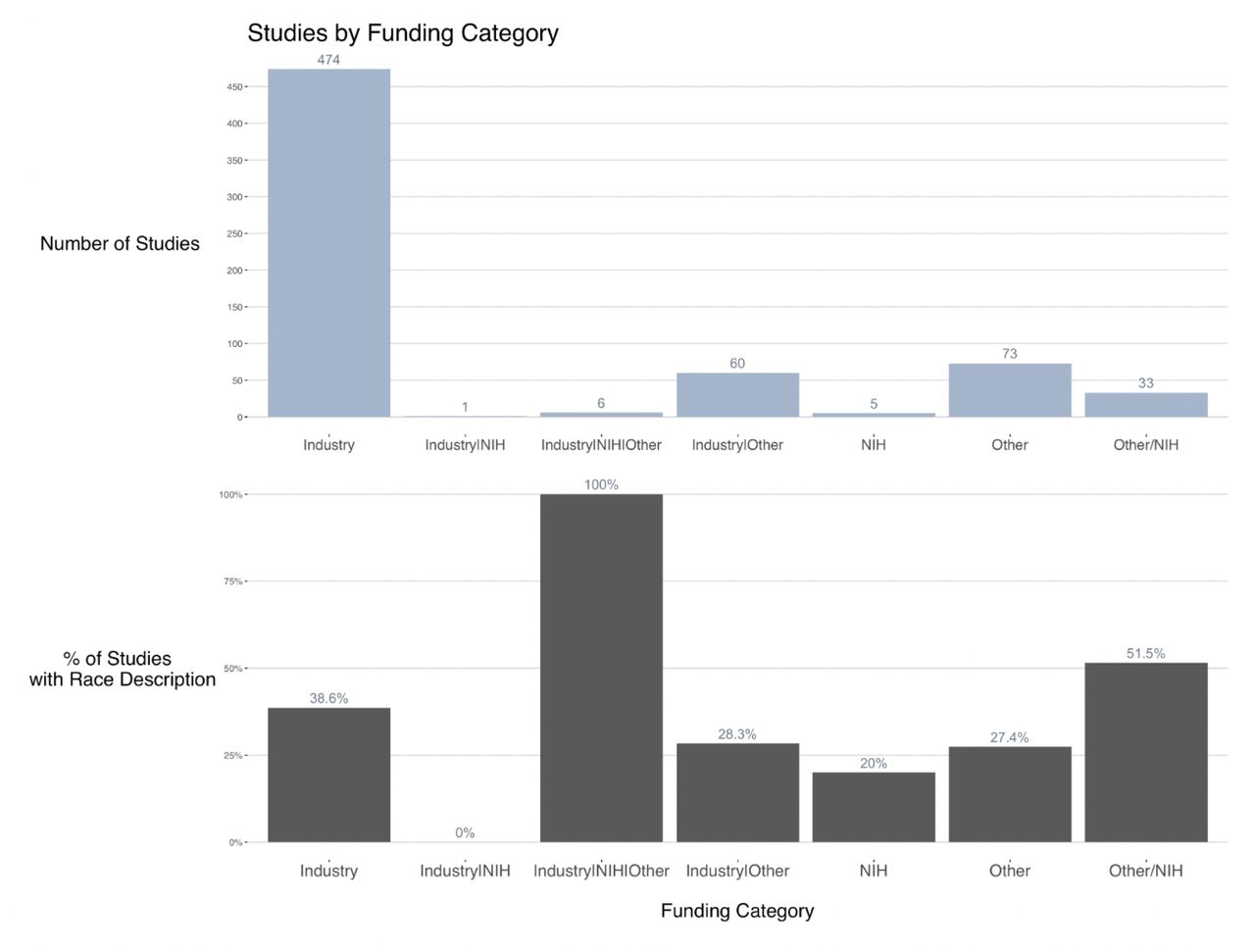
Industry-funded studies were most prevalent, representing 81.9% of the CTs; 7.1% had NIH funding. Race was described in 38.6% of the industry-exclusive funded, 27.4% of other, 51.5% in other and NIH and 20% of NIH-funded studies (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Clinical Trials funding characteristics and percentage with race description. NIH, National Institutes of Health.
The white group was more common in all types of financing, and the American Indian or Alaskan Native was the less represented.
Discussion
Our findings corroborate those of other ophthalmological CT reviews, which have shown the majority of patients to be white and from high-income countries, with under-representation of racial and ethnic minorities.14–16 To address this longstanding problem, new FDA and NIH initiatives, for example, Bridge2AI and AIM AHEAD, are driving more diverse and representative datasets in medical research.17 18
In ophthalmology, it is not usual to validate and reproduce CTs in distinct countries and populations. However, there are numerous examples of treatments in other medical areas that have been found to be beneficial in studies conducted in one country, but without benefit or even harmful in another country. For example, the Surviving Sepsis Guidelines for paediatric intensive care include rapid and early fluid resuscitation based on US-based studies; nevertheless, in a CT with a sub-Saharan African population, this gold standard treatment increased the risk of death, raising concern about implementing guidelines without local validation.19
More diverse cohorts and studies are needed to determine the exact relationship between diseases and treatment, especially in minority groups, where the gap in medical care access is greater.5 Inclusion of sex description is one of the NIH recommendations in clinical research, and it is reported in 99.5% of the participants in NIH-funded ophthalmologic CTs, with an acceptable gender distribution among enrolled patients.
The NIH requires the reporting of the breakdown of the race–ethnicity of trial participants, but it is reported in half of the ophthalmologic CTs in the US and in 20% of non-US CTs, although with improvement in recent years. The lack of standards in the reporting of race–ethnicity is also an issue. While the NIH has recommended racial categories, various studies used different racial classifications. For example, some trials had distinct classifications for Hispanic participants, and some had distinct categories for Asian participants.
A review from Allison et al reported a disproportionately low representation of minority participations in glaucoma CTs,20 a similar finding to what we identified across all ophthalmologic specialties. Our study shows that in ophthalmological CTs, white patients are predominant, with lower representativeness of blacks, Asians and other groups. This raises a concern in the applicability of the findings to patients who are not white and from low-and-middle-income countries (LMIC).
In ophthalmological CTs, only 69 countries out of 195 total countries in the world are represented. Most of the ophthalmological CTs are from populations of high-income and upper-middle-income countries, with only 0.25% from low-income countries where the burden of disease is actually highest. Several barriers to better representation of marginalised communities in ophthalmological CTs have been outlined previously. With substantially lower rates of medical insurance and access to care, patients from racial/ethnic minorities are less likely to present to health systems and consequently less likely to be recruited to trials.21 Even when access to insurance and healthcare is available, trial participation requires extraneous costs such as additional transport and additional/prolonged clinical visits, which curb participation.22 English proficiency is usually required for trial participation. Mistrust in physicians and research institutions further compound difficulties in recruiting underserved populations.22
Although the reasons for (and consequences of) poor recruitment and representation have been well documented, to the authors’ knowledge little has been done by ophthalmological research bodies to prioritise more representative inclusion. A recent global review published in the Lancet highlights this, demonstrating that of 66 recent diabetic retinopathy RCTs, none were performed in LMICs.23 A review of trials analysing how to improve access to cataract services showed only two RCTs were from LMICs.24 And despite the disproportionate prevalence of glaucoma in black populations, major trials examining the effect of medications on glaucoma have not included non-white racial groups altogether.25 Overall, almost three-quarters of published ophthalmological studies were undertaken in HICs—several regions in Southeast Asia, sub-Saharan Africa and Latin America had especially low representation.26
Strategies to improve representation in ophthalmological trials have been outlined elsewhere. They stress the importance of educating researchers in HICs on recruiting those from marginalised populations into trials.15 16 Collaboration with racial and ethnic minority clinicians and clinics that primarily serve minority communities, and establishing research facilities in LMICs, means research can be performed by those caring for those populations.15 16 Engaging members of marginalised communities as stakeholders in trials is crucial in fostering trust in the medical research community.15 27
The collection of demographic information in CTs is improving, with almost all studies including gender description and an increasing number with race and ethnicity descriptions. However, updated classifications to better represent groups are necessary, such as more detailed information among Hispanic and Asian groups.
Race and ethnicity distribution varies among countries, and reporting in CTs is fundamental to verify the generalisability and ensure external validity of findings.
There is little incentive to perform CTs, and research in general, in resource-limited countries, perpetuating the global knowledge gap, which in turn fuels the divide between rich and poor countries. Advocacy from within the research community, governments and non-government players such as the WHO, is necessary to increase representativeness and improve applicability of medical research to those who are most burdened by disease.
Limitations
Our study has several limitations. First, it was restricted to clinicaltrials.org and PubMed articles indexed with the same NCT Number. Second, it only included completed phases III and IV CTs. Third, it is possible, although unlikely, that trials without race–ethnicity information may have better demographic representation.
Conclusion
Overcoming the burden of eye disease on marginalised populations is contingent on their inclusion in clinical ophthalmological trials. Given how trials inform future research and funding (and ultimately treatment availability), the systematic under-representation of already marginalised communities has only served to widen the eye health chasm, one which is currently largely attributed to poor access to care.15 In fact, the knowledge gap that results from healthcare delivery that is designed to optimise outcomes only in the majorised population is also an important driver of this chasm.
Data availability statement
Data are available upon reasonable request. All the data used in this article is available at www.clinicaltrials.org. All the article data are available under request.
Ethics statements
Patient consent for publication
Ethics approval
The research undertaken is exempt from institutional review board approval and informed consent as only publicly available aggregate data from 1990 to 2022 were analysed.
Footnotes
Twitter @WPhanphruk
Contributors LFN: Guarantor, conceptualisation, data curation, investigation, methodology, writing—original draft, writing—review & editing. WGM: Data curation, writing—original draft, writing—review & editing. SS: Writing—original draft, writing—review & editing, visualisation. APDS: Data curation, writing—review & editing. WP: Data curation, writing—review & editing. KK: Data curation, writing—review & editing. LAC: Conceptualisation, supervision, data curation, writing—review & editing. CVSR: Data curation, writing—review & editing, supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.