Article Text

Abstract
Background The current study aimed to analyse epidemiological data on eye burns in Wuxi, China, for the years 2015–2021, and to provide insight into the development of appropriate prevention strategies.
Methods A retrospective study was conducted on 151 hospitalised patients with eye burns. Data collected included gender, age, the monthly distribution of incidence, cause of eye burn, the site of eye burn, the type of surgery, visual outcome, the length of hospital stay and the cost of hospital admission. Statistical analysis was performed using SPSS V.19.0 and Graph Pad Prism V.9.0.
Results In a total of 151 eye burn patients, 130 were males (86.09%) and 21 were females (13.91%). The proportion of patients classified as grade III was the greatest (46.36%). The average age of our hospitalised patients with eye burns was 43.72 years and the average length of hospital stay was 17 days. The number of injuries was highest in September (14.6%). Among eye burn patients, workers and farmers became the most common occupations (62.91%, 12.58%). The most frequent cause of burns was alkali burns (19.21%), followed by acid burns (16.56%). When admitted to the hospital, patients’ average vision was 0.06, and 49% of them had a poor vision (<0.3, ≥0.05).
Conclusion With an investigation of 7-year hospitalisation data, the current study provided a fundamental reference for epidemiological features and management of eye burns in Wuxi, China, which could contribute to the development of treatment and prevention strategies.
- epidemiology
- eye (tissue) banking
- public health
- wound healing
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Eye burns could constitute an ophthalmic emergency, and most research has focused on chemical eye burns.
WHAT THIS STUDY ADDS
Our data are for the last few years, so it is time-sensitive. And the results are relatively comprehensive in Eastern China.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The findings of the study provided a fundamental reference for the epidemiology of eye burns in Wuxi, China, which could contribute to the development of management and prevention strategies.
Introduction
The eye processes massive information that is received by humans from the environment.1 Eye burns could cause significant harm to the ocular surface and the anterior part of the eye, leading to long-term monocular or binocular vision impairment. The patient’s quality of life and psychological problems might be significantly impacted by such a long-term handicap.2 The most frequent causes of eye burns are industrial injuries.3 4 Chemical and thermal burns account for around 15% of eye injuries5 and need immediate medical attention since the tissue and function of the eye can be seriously damaged if not treated promptly.6 Epidemiological studies of eye burns could provide important data and reference for the development of strategies for prevention and emergency care of eye burns. However, by for epidemiological data on eye burns in China remains limited, and the clinical characteristics and management of eye burns need to be evaluated. In the current study, a total of 151 in-patients with eye burns admitted to the Affiliated Hospital of Jiangnan University in Wuxi were enrolled to investigate the latest epidemiological features and management of eye burns in Eastern China.
Materials and methods
Data collection
Data from 8474 burn patients admitted to Wuxi City from 2015 to 2021 were reviewed retrospectively, including 151 patients were diagnosed with eye burns. Patients’ information was collected including gender, age, the monthly distribution of incidence, cause of eye burn, the site of eye burn, the type of surgery, visual outcome, the length of hospital stay and the cost of hospital admission. Inclusion criteria for patients with eye burns were as follows: (1) Eye burns diagnosed by an ophthalmologist; and (2) Patients without a history of systemic, local, or infectious disorders of the eyelid, cornea, conjunctiva or uvea based on medical history and slit lamp microscopy; (3) No history of diabetes or other ocular surface disorders except eye burns: no ocular trauma lacrimal duct irrigation, or intraocular surgery and (4) No history of wearing corneal contact lenses.
Classification of eye burns
The clinical manifestations of eye burns are graded according to Dua et al’s report.7 Grade I: Eye burns with only corneal epithelial damages and no limbal or conjunctival involvement. Grade II: The limbus was involved for less than 3 hours and the adjacent conjunctiva was involved for less than 30% of the time. Grade Ⅲ: Damage occurs when the limbus is engaged between 3 and 6 hours and the conjunctiva is implicated between 30% and 50%. Grade Ⅳ: When the limbus is implicated at 6–9 hours and the conjunctiva is 50%–75% involved, for which reconstruction of the ocular surface has the potential to provide favourable outcomes. Grade Ⅵ: When the limbus was involved for more than 9 hours but less than 12 hours, the grade was Ⅴ if the full limbus was not involved, and grade Ⅵ otherwise.
Corneal fluorescein staining
The whole corneal epithelium might block the passage of the chromosomal when the corneal fluorescence is labelled. By colouring the corneal fluorescence, this indicator may, therefore, assess the degree of the corneal epithelial defect. Following the TBUT test, the degree of corneal epithelial defect may be assessed under the crack lamp.8
Low vision examination
A low vision checklist based on the national vision gauge standard is used for low vision examination (GB-11 533-2011). It is computed at 0.1 d/5 when the patient’s eyesight is less than (0.1 d is the distance from the inspector to see the timing of the timeline distance). If the patient cannot recognise at 5 cm, the index is modified to manual (HM)/distance.9
In vivo confocal microscopy
Corneal topography was conducted using the Heidelberg Retina Scanner III’s corneal module (Heidelberg Engineering, Heidelberg, Germany). Each subject was given 0.5% procaine eye drops as a topical anaesthetic prior to the examination. Disposable sterile plastic caps were used to lubricate and improve optical connections (Tomo-Cap, Heidelberg Engineering, Heidelberg, Heidelberg, Texas, USA).10
Statistical analysis
Age and length of hospital stay were represented as mean values±SD, while qualitative data were presented as numbers and percentages. The Mann-Whitney U test or the Kruskal-Wallis test was used to compare the medians of two or more categorical variables. Microsoft Excel 2007 was used to enter and process the majority of the data. A p<0.05 was regarded as significant when analysing the data using Graph Pad Prism V.9.0 and SPSS V.19.0.
Results
Patient demographics
From 2015 to 2021, the database contained 8474 hospitalised burn patients with an average age of 26.80 years, including 5565 male (65.67%) and 2909 female (34.44%). There were 151 (1.78%) patients with eye burns, including 130 men (86.09%) and 21 females (13.91%). They were all hospitalised patients who got therapy. The average age was 43.72 years old, with the age range being 3–73 years old (table 1). Thirty-one (20.53%) hospitalised patients were between the ages of 30 and 39, 51 patients (33.77%) were between the ages of 40 and 49, and 41 patients (27.15%) were between the ages of 50 and 59 (figure 1). Workers, farmers, preschoolers, managers (professional technicians), pensioners, etc were among the patients' vocations. Workers made up the majority of patients (62.91%), while farmers (12.58%) made up the second-most common category (table 1).
Distribution of selected variables among eye burn patients (N=151)

Number of eye burns patients represented according to the grade of eye burn by age.
Causes of eye burns
According to table 2, among the 151 patients with eye burns that were examined, acid (mostly hydrochloric acid, nitric acid and hydrofluoric acid), alkali, aluminium liquid, copper liquid, zinc liquid, molten steel, thermal burn and electric shock are the leading causes of burns (table 2). Alkali/acid (29, 19.21%; 25, 16.56%) and thermal scald (20, 13.25%) were the main causes of burns, followed by explosions and aluminium liquid which accounted for 12.58% of all burns. The incidences of burns caused by fires, touch, electricity, chemicals or explosives rises rapidly when people enter working age (18–59 years old). Additionally, eye burns caused by fire, lightning, chemicals or explosions are more frequent in summer. The great majority of burns are unintentional, with contact, electrical, chemical or explosion burns brought on by disregard for safety protocols and individual carelessness at work. Home burns are the most frequent kind of burns among elderly persons (>60 years).
Nature of injury (N=151)
Clinical features of eye burns
Eye burns in the 151 patients were graded according to Dua et al’s classification. The figure shows that the proportion of patients classified as grade III has the most frequent (46.36%), followed by grade IV and grade II (27.15%, 19.21%) (figure 1). There was a significant difference in the length of hospital stay of patients of different classes. Furthermore, an examination of the hospitalisation costs for 61 of these patients revealed that overall hospitalisation costs rose with burn severity (table 3). Online supplemental table S1 shows that 151 patients had an average vision of 0.06 at the time of their initial diagnosis of admission, with an average vision of 0.07 for females. When being admitted, there is no statistically significant difference in vision between males and females (p>0.05). 59.6% of the patients had a low vision when they were admitted to the hospital. Additionally, the assessment examination prior to discharge revealed that their vision had improved significantly (p<0.001), however, poor vision was observed in 3.97% of the patients.
Supplemental material
Total expense paid by the patient and the proportion of each part (N=61)
Month distribution of eye burns
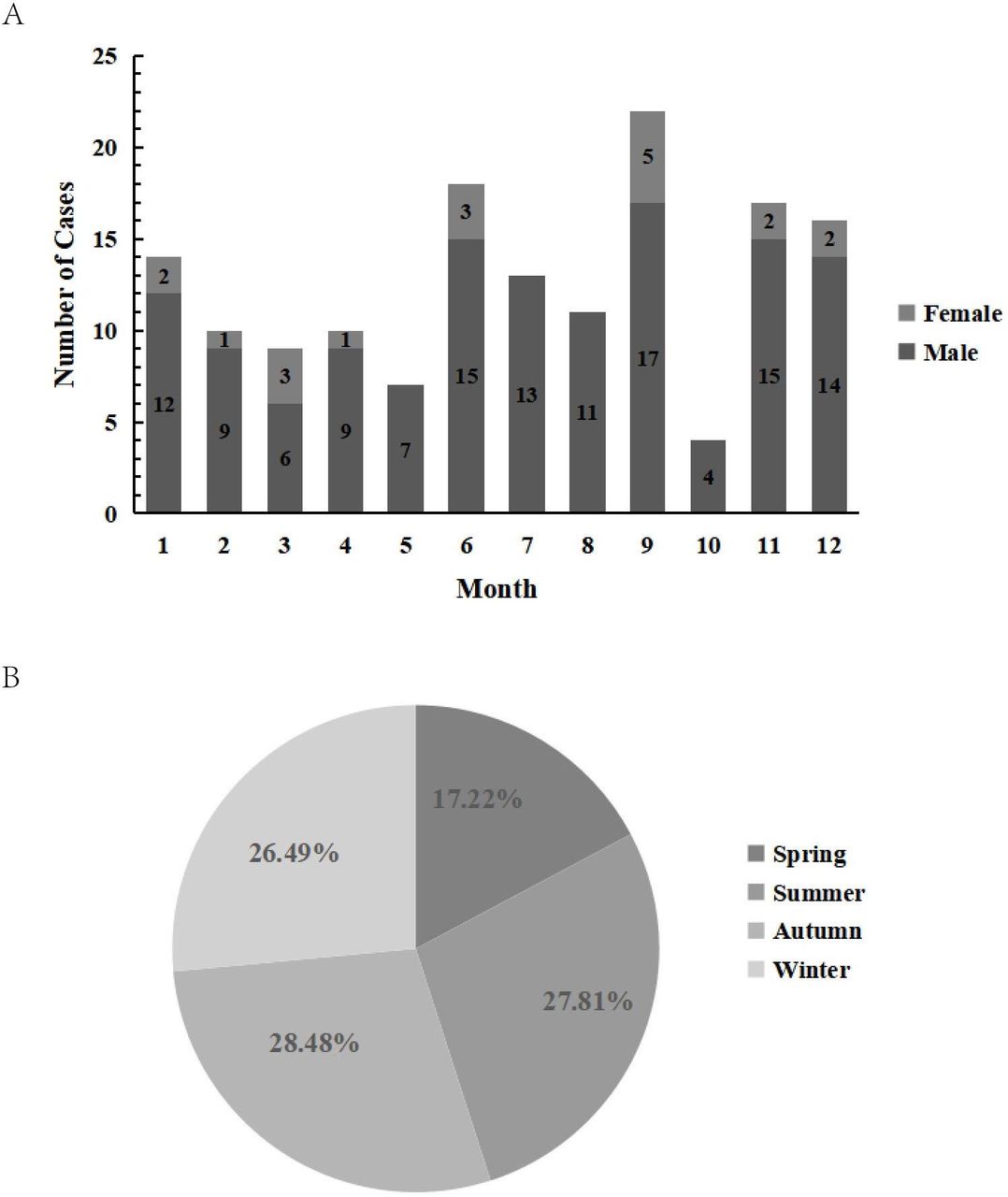
Eye burn incidences were more frequent in June, September, November and December according to the distribution of the months throughout the year. The most admissions occurred in September (22, 14.6%) and the least in October (4, 2.6%) (figure 2A). The season has an impact on the frequency of burns. With 43 (28.5%) patients, autumn (September, October and November) was shown to be the season when people were most vulnerable. The spring months of March, April and May had the fewest burn victims, with 26 hospitalised patients (17.20%) during this time (figure 2B).

{kind=link}
{kind=link}
Month and season distribution of ocular burn patients. (A) Number of patients being represented graphically according to month distribution in male and female groups. (B) The proportion of ocular burn patients in the four seasons.
The length of hospital stay
The average length of hospital stay for patients with eye burns was 17 (17.3±14.55) days, according to the report (table 1). The length of their hospitalisation was the longest between 0 and 9 days (53, 35.1%), accounting for 68.21% of all hospitalisation days (online supplemental figure S1). For males, the median length of their hospitalisation was 13.5 (2, 123) days, compared with 9 (3, 35) days for females. Neither the patients’ gender nor whether they took traditional Chinese medicine made a difference in the length of hospital stay (p=0.098). Additionally, there was no significant difference in the days spent in the hospital(p=0.276) (online supplemental table S2). Forty-two patients (27.81%) underwent surgery while they were hospitalised, with one patient requiring four surgeries (table 1).
Medical expenses
A total of 61 patient cases were eliminated for statistical expenditures, and the average amount spent on medical care was CNY3497.42 (table 3). Respectively, the average percentages of conventional western medicine, traditional Chinese medicine, examination costs and operating costs were 16.65%, 71.74%, 2.43% and 9.18%. Patients who had bilateral burns had considerably greater medical costs than those who only sustained single eye burn (p<0.001). The patient’s payment was substantially connected with the length of their hospitalisation, according to Kruskal-Wallis (p<0.001).
Discussion
Patient demographics
Eye burn incidents are on the rise in developed nations and it contributes to about 10%–18% of all eye injuries, according to some research.11 What is intriguing about this study is that when age-related data are examined, the age group most affected is neither the youngest nor the oldest, but the 30–49 age range. This is congruent with a data of East China by Le et al, but differs with Bizrah’sstudy that found the average age of eye chemical burns to be 23 years old.12 13 Instead of focusing on individuals who have just joined, people at this point need to conduct ongoing risk prevention training.14 This study’s patients are mostly labourers and farmers, with 81.45% being between the ages of 30 and 59. Corporate management and government regulatory bodies should prioritise reducing workplace harm by investing in more sophisticated protection gear and training programmes for employees on how to use personal protective equipment. Farmers suffer the second most frequent burn. The majority of the time, migrant employees lack proper professional training. They lack knowledge of the dangers of several acids and alkaline pesticides as well as the appropriate treatment options, particularly first aid procedures, when exposed to pesticides and other substances.
Causes of eye burns
Eye burns are frequent in China, particularly in several high-risk industries including manufacturing and construction work. The rapid development of industrialisation in Wuxi and the adjacent areas may be to blame for the fact that acid/alkaline compounds are the most prevalent cause of eye burns.15 16 In contrast to this study, Bizrah et al discovered that 70% of severe eye chemical burns were caused by an assault.12 Rinsing the eyes in large numbers is a critical emergency treatment strategy in the event that the important burns prevention strategy fails and eye burns develop. Tap water is the simplest and most convenient rinsing option. Except for locations using tap water, all employees should be provided with eye flushing equipment and instruction on how to use them.17 According to the findings of the Parmar’s study, 70% of patients experienced injuries at or near their homes, prompting us to pay closer attention to heat (flames, fireworks and hot liquids), electricity and microwave meals.18 According to the findings of this study, alkali is the most common chemical burn material, followed by acid.13 19 20 Reducing eye burn from pyrotechnics and firecrackers, as well as increasing laws and law enforcement, might be crucial during holidays. Eye burns from microwave-related things, such as eggs, microwave popcorn and overheated water, have increased in frequency over the past several years as their use has increased. The most important thing is to promote public awareness of microwave cooking techniques, including how to microwave eggs and to look after and guide children and the elderly while using these appliances.
Clinical features of eye burns
Ballen21 developed the first categorisation of ocular surface burns, which was later refined by Roper-Hall. The knowledge and understanding of ocular surface healing and surgical treatment of ocular surface burns have progressed substantially in the years since the Roper-Hall classification was introduced. According to Dua et al, ocular surface burns should be evaluated analogously rather than graded. The new classification methods depicted the extent of ocular surface damage and anticipate damage consequences more precisely. As a result, we used Dua et al’s classification of eye burns. The new classification of eye burns now includes a prognosis evaluation. Grade V and VI have a bad prognosis, although the other grades may improve with therapy. The greater the grade, the more serious the eye burn and the associated increase in hospital days and total expense of hospitalisation.
Month distribution of eye burns
As was previously stated, the ambient temperature was connected to various populations, burn sites, causes, etc. Compared with the rest of the year, eye burns occurred more often between June and September and October and December. This contradicts the findings of Jess’s investigation. According to the data they presented, the months with the highest incidence of chemical eye burns are June and July.14 The favourable temperature in the Wuxi region and the fact that fall and winter are ideal seasons for municipal industrial output and building may be to blame for the phenomena our study depicts. Since June, the weather becomes sweltering, and individuals are less likely to use safety gear like safety glasses, which might lead to an increase in cases of eye burn. Therefore, businesses should strengthen individuals’ awareness of protecting themselves during the high incidence season.
The length of hospital stay
The average length of hospital stay for eye burn patients in the current study was 17 days, which was longer than previously reported. One of the key causes was that the majority of patients who came in had been exposed to more dangerous chemicals or had burns in other parts, that patients with serious burns tended to dwell in a burn unit, and that the length of hospital stay often lasted until the patients’ wounds were nearly healed. As a result, the length of hospital stay could be longer than necessary for the treatment of eye burns. This finding implies that in order to reduce the typical length of hospital stays, additional strategies may be required. The usage of traditional Chinese medicine by patients and the length of hospital stay were both examined in this study. According to traditional Chinese medicine, heat toxicity is what causes burns and scalds, hence heat-clearing and detoxifying medications are frequently prescribed as treatments. Traditional Chinese medicines and their preparations for the treatment of burns and scalds are used in clinical settings because, according to some studies, they are non-toxic, have gentle medicinal properties, have a strong bacteriostatic effect and are less likely to cause drug resistance when used takes up a position in the process.22 Due to the limited sample size, there was no statistically significant relationship between the patients’ use of traditional Chinese medicine and the length of their hospitalisation in this study (p=0.276).
Medical expenses
The hospitalisation expenses include traditional Chinese medicine, western medicine, examination costs and surgery costs. Medical expenses increase with the degree of eye burns, among which the cost of western medicine and western medicine treatment accounts for the vast majority. Comparing hospitalisation costs for burns in monocular and binocular burns showed significant differences. The contact area and degree of penetration have a direct impact on how seriously an eye injury is caused. Most patients with mild burns do not need surgery, and minor burns seldom result in permanent sight impairment. The ocular surface tissue is typically completely destroyed as a result of moderate or severe burns, necessitating extensive medical care and repeated procedures.23 Longer hospital stays result from the lengthy process of visual recovery following many difficult procedures. As a result, patients with more serious burns have greater medical costs, and those costs are closely tied to how long a patient stays in the hospital.
Conclusions
In conclusion, eye burn cases exhibit the traits listed below in Wuxi: Patients are primarily farmers and workers, and most cases occur at work. Acid/alkali and thermal burns are the leading causes of eye burns, followed by explosions and aluminium water. Most frequently, these damages afflict people between the ages of 30 and 59. Employers should strengthen the sense of responsibility for their employees. Doctors and decision-makers may allocate resources for treatment and prevention more effectively by using the epidemiological trend that predicts eye burns. This study may contribute to creating an eye burn database and formulating preventative measures for severe eye burns.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This research was approved by the Ethics Committee of Human Research in Affiliated Hospital of Jiangnan University and was in accordance with the Declaration of Helsinki (Registration number: JNU20220310IRB46). Informed consent was obtained from all participants.
Acknowledgments
All authors gratefully acknowledge the ophthalmology team of Jiangnan University’s Affiliated Hospital for their collaboration and Jiangnan University’s support.
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
ZL and TC contributed equally.
Contributors Zi-jing Lu and Ting Chu planned and designed the study. Zhi-hui Yang, Zi-jing Lu, Yi-hui Shen and Xin Xia contributed to data collection, data analysis and data interpretation. Zi-jing Lu played a leading role in writing the manuscript. Jian-huan Chen and Ji-hong Wang revised the manuscript. All authors read and approved the final manuscript.
Funding The project was supported by the Research Project of Public Health Research Center of Jiangnan University (2018-2020, JUPH201809), Wuxi Municipal Health Commission (T201901), Maternal and Child Health Research Project of Wuxi Health Commission (FYKY201903), Wuxi Science and Technology Bureau (N20192030).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.