Article Text

Abstract
To facilitate the integration of eye care into universal health coverage, the WHO is developing a Package of Eye Care Interventions (PECI). Development of the PECI involves the identification of evidence-based interventions from relevant clinical practice guidelines (CPGs) for uveitis.
A systematic review of CPGs published on uveitis between 2010 and March 2020 was conducted. CPGs passing title and abstract and full-text screening were evaluated using the Appraisal of Guidelines for Research and Evaluation II (AGREE II) tool and data on recommended interventions extracted using a standard data extraction sheet.
Of 56 CPGs identified as potentially relevant from the systematic literature search, 3 CPGs underwent data extraction following the screening stages and appraisal with the AGREE II tool. These CPGs covered screening for, monitoring and treating juvenile idiopathic arthritis (JIA)-associated uveitis, the use of adalimumab and dexamethasone in treating non-infectious uveitis, and a top-level summary of assessment, differential diagnosis and referral recommendations for uveitis, aimed at primary care practitioners. Many of the recommendations were based on expert opinion, though some incorporated clinical study and randomised controlled trial data.
There is currently sparse coverage of the spectrum of disease caused by uveitis within CPGs. This may partially be due to the large number of conditions with diverse causes and clinical presentations covered by the umbrella term uveitis, which makes numerous sets of guidelines necessary. The limited pool of CPGs to select from has implications for clinicians seeking guidance on clinical care strategies for uveitis.
- Inflammation
- Public health
- Retina
- Treatment other
- Treatment Medical
- Epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
A key recommendation of the WHO’s 2019 World report on vision1 was to embed eye care within universal health coverage (UHC) in order to address inequities in access to eye care services and contribute to Sustainable Development Goals.2 To enable countries to plan, budget and integrate eye care into UHC, WHO is developing a priority package of eye care interventions (PECI), in collaboration with Cochrane Eyes and Vision (CEV).3 A crucial step in the development of the PECI is the systematic identification of evidence-based eye care interventions for selected priority eye conditions using high-quality clinical practice guidelines (CPGs) and, where needed, systematic reviews. Uveitis has been identified as 1 of 15 priority eye conditions for inclusion in the PECI.
Uveitis is a common, sight-threatening group of disorders, all of which are characterised by inflammation of the uveal tract of the eye (iris, ciliary body and choroid). Population-based studies have suggested an overall incidence of 17–52 people in 100 000 each year, and that uveitis causes 9%–15% of blindness in the Western World.4 Classifying this heterogeneous disease spectrum, which spans numerous infectious and autoimmune diseases, has been a unique challenge for ophthalmic clinicians. The standardisation of uveitis nomenclature (SUN) group sought to standardise the descriptions of the diseases and syndromes,5 mapping at least 28 uveitis diseases in 2005. This variability in disease features, both across and within distinct disease groups, has impacted clinical trials in uveitis.
Nevertheless, interventions for uveitis are continually emerging. These have included medications applied to the eye such as topical steroid6 and non-steroidal eye-drops, local injection treatments to the eye and intraocular steroid implants,7 systemic immunosuppressants8 and immunomodulatory therapies which include newer biologic treatments.9 The purpose of this paper is to present the results, including the quality and current state of evidence, of a systematic review of CPGs for uveitis.
Methods
This systematic review of CPGs was conducted in compliance with the methodology presented in the introductory PECI paper.3 Exclusion criteria for each stage of screening below are provided in table 1. The stages in the review are as follows:
Exclusion criteria for screening of clinical practice guidelines (CPGs)
Systematic literature search
A single, systematic literature search of selected academic (MEDLINE, Embase, CINAHL, Global Health, Global Index Medicus) and guideline databases (online supplemental Appendix 1) was carried out by a CEV information specialist in March 2020. MeSH terms were used where applicable. In addition, the websites of professional ophthalmology and optometry associations’ were searched for relevant guidelines (online supplemental Appendix 1). All searches were limited to the last 10 years, to ensure evidence was current, and to English language, to ensure timely completion of the PECI. The search strategy for academic databases can be found in online supplemental Appendix 2.
Supplemental material
Title and abstract screening
Two members of the technical working group independently screened the titles and abstracts of articles identified from the systematic literature searches. Title and abstracts were presented, and responses tracked, using Abstrackr, a semiautomated online citation screening programme.10 Citations were excluded if they were not in the English language, not a CPG or were not relevant to a priority eye condition. A secondary title and abstract screening was then conducted to identify CPGs potentially relevant to uveitis. All disagreements were resolved by discussion between a CEV representative and the WHO.
Full-text screening
Following title and abstract screening, independent full-text screening of the CPGs relevant to uveitis was conducted by two authors (NG and IRR). CPGs without author affiliations listed, or with undisclosed or unmanaged conflicts of interest, were excluded. Discrepancies were resolved through discussion between the two authors or, in the event a consensus couldn’t be reached, by discussion with a third author.
Quality appraisal
The same two authors who conducted full-text screening went on to independently evaluate the quality of CPGs using the ‘Appraisal of Guidelines for Research and Evaluation’ (AGREE II) tool.11 Nine items (4, 7, 8, 10, 12, 13, 15, 22 and 23) were specifically used for the appraisal of CPGs (online supplemental Appendix 3). These items were selected based on a consensus finding process among three researchers12 and in consultation with WHO Guideline Review Committee Secretariat. If the rating of an item differed by more than two points between the two researchers, the results were discussed between the two authors, and a representative of WHO or CEV, if necessary, to reach consensus.
Following evaluation with the AGREE II tool, guidelines were excluded if (1) the average score of the two researchers for items 4, 7, 8, 12 or 22 was below 3 or (2) the sum of the average score of the two researchers for all nine items is less than 45.
Data extraction
Data on recommendations were extracted from selected CPGs by one author using a standardised form that captured information on the recommendation (type of recommendation, dosage, target group, etc), the strength of recommendation and the quality of the evidence used to inform the recommendation. The data extraction was then independently checked by a second author. In the event of disagreement, a third author was involved and agreement reached by discussion. The process was repeated for all the CPGs until agreement on the recommended eye care interventions was reached.
With respect to the published protocol, no changes were made. The quality check and the methodological support for this study have been provided by the WHO and CEV.
Results
Title and abstract screening
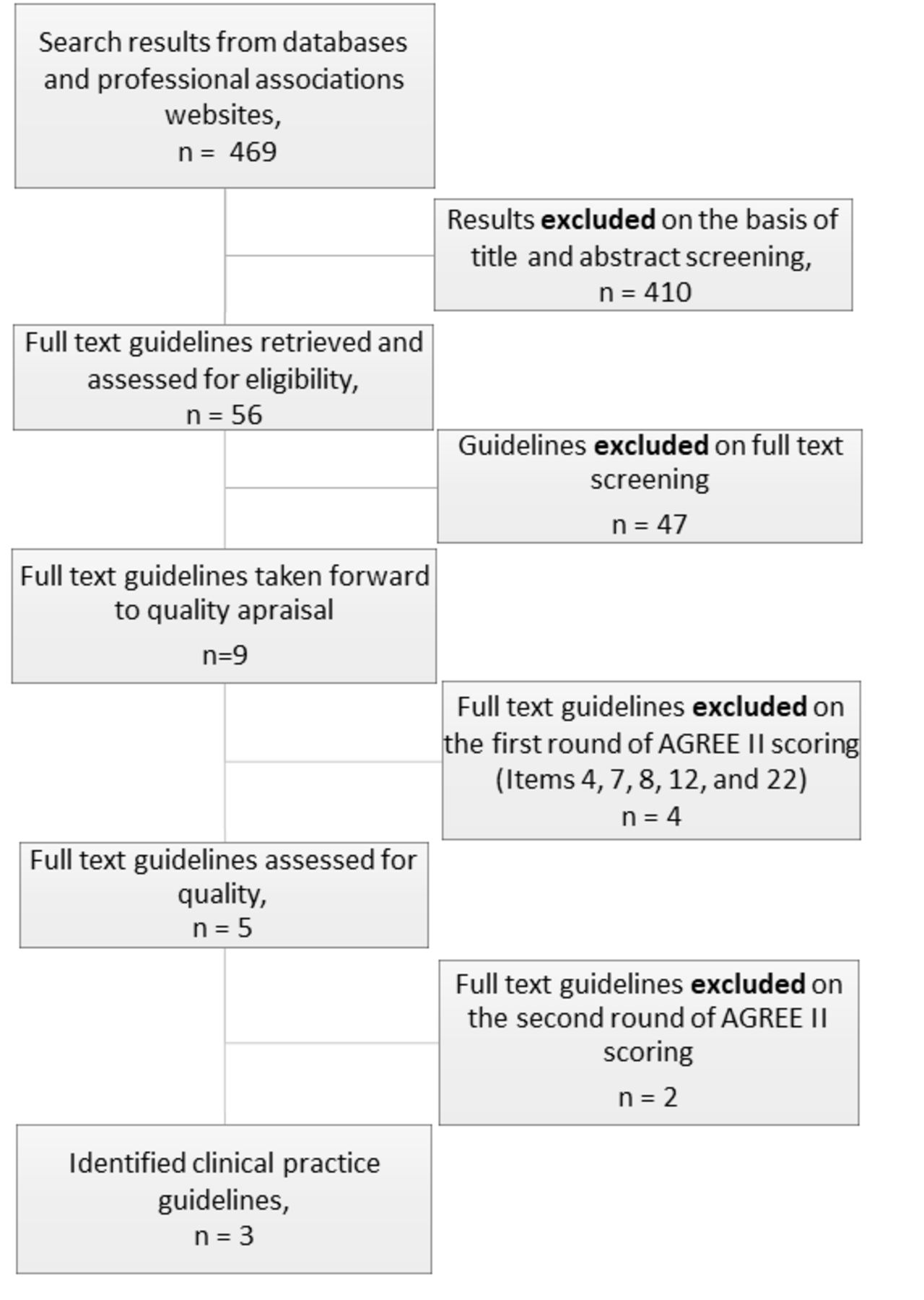
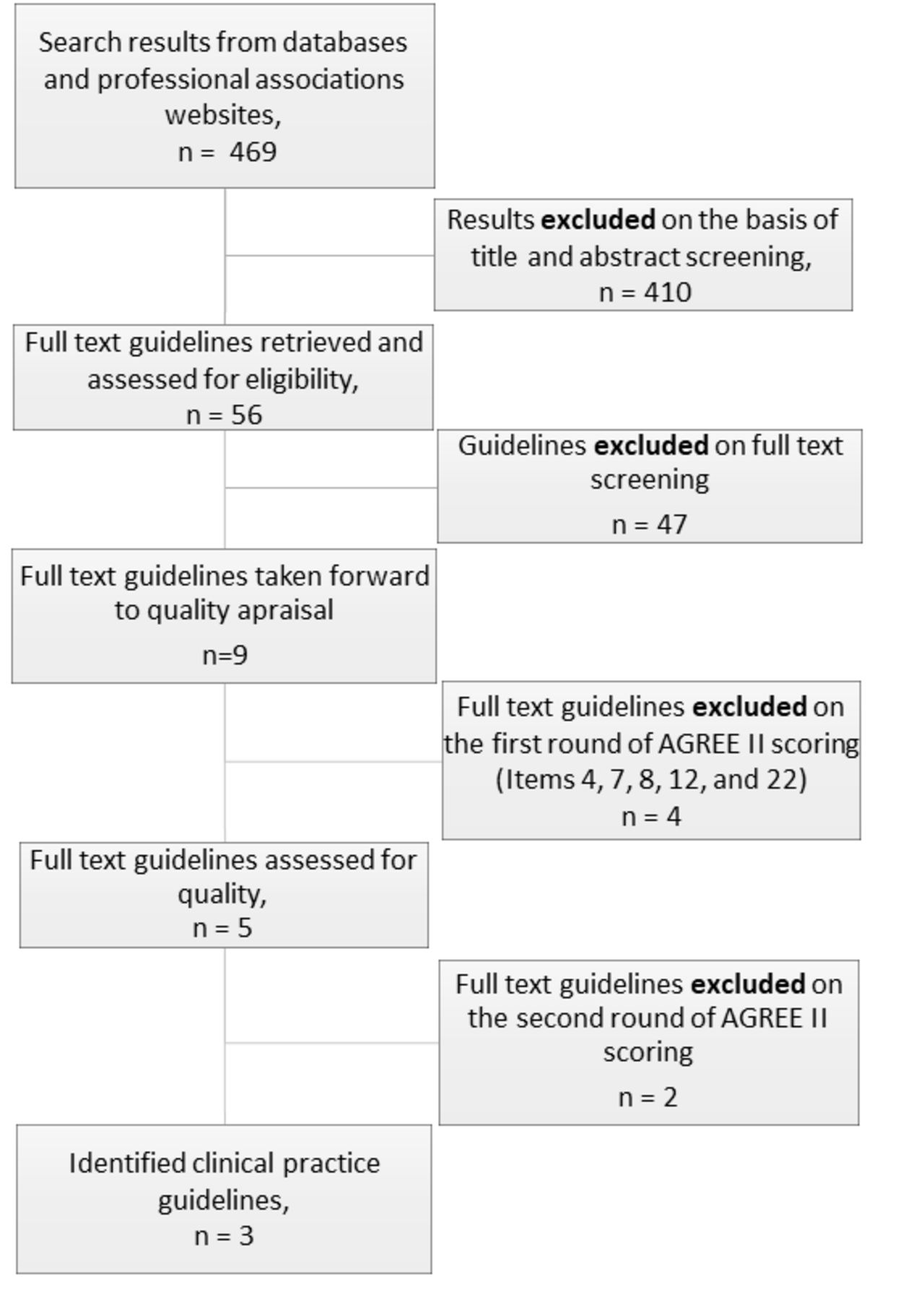
The results of the selection process are summarised in figure 1. After combining all searches from academic and guideline databases and professional association webpages, 469 CPGs were identified and underwent independent title and abstract screening. Fifty-six of these were judged to be potentially relevant to uveitis after title and abstract screening, and went on to full-text screening.
{kind=link}
Results of the screening process (diagram).AGREE II, Appraisal of Guidelines for Research and Evaluation II.
Full-text screening and quality appraisal
Of the 56 potentially CPGs with potential relevance to uveitis, 47 CPGs were excluded. Forty were judged not relevant to uveitis. In a further two cases, exclusion was based on industry funding of the guideline, or because the presence or absence of possible conflicts of interest were not stated, as well as the author affiliations not being stated.13 14 A further four were excluded based on the potential conflict of interest criteria alone,15–18 and a final one because the author affiliations were not listed.19 A total of nine CPGs were considered potentially relevant and passed to the quality appraisal phase. Of these nine, there were no concerns over conflicts of interest, and author affiliations were unambiguous. Following quality appraisal with the AGREE II tool, six guidelines were excluded for the following reasons (figure 1): four because the average score of the two researchers for items 4, 7, 8, 12 or 22 was less than 3,20–23 and two because the sum of the average score of the two researchers for all nine items was less than 4524 25 (table 2).
Guidelines found and selected, and their score in respect of the criteria used to reach the final choice
The CPGs identified for data extraction were as follows26–28:
Adalimumab and dexamethasone for treating non-infectious uveitis, National Institute for Health and Care Excellence (NICE) (UK) Technology appraisal guidance, July 2017.
2019 American College of Rheumatology/Arthritis Foundation Guideline for the Screening, Monitoring and Treatment of Juvenile Idiopathic Arthritis-Associated Uveitis.21
Uveitis Clinical Knowledge Summary, NICE (UK), November 2019.
The AGREE II ratings for the three selected CPGs are presented in table 2.
Data extraction
An overall view of the strength of recommendation and quality of evidence given in each selected guideline is reported in table 3. Specific recommendations extracted from each CPG are given in online supplemental table, along with the strength of the recommendation as assessed by the guideline writers, and the type of evidence used to make the recommendation.
Supplemental material
Strength of recommendation and quality of the evidence of the retrieved CPGs
The three selected guidelines covered various areas of clinical practice and types of uveitis. The 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Screening, Monitoring and Treatment of JIA-Associated Uveitis27 covered a specific type of uveitis which is associated with JIA. The document included recommendations for screening, monitoring and treatment of the condition as well as patient education, which were drawn up by an expert panel using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology. General recommendations of note in this guideline centre on tight monitoring of children with uveitis; the authors suggest every 3 months for stable, treated uveitis and monthly for patients tapering treatment. Specific treatment recommendations include using prednisolone acetate 1% over alternative topical preparations, and using topical corticosteroids for short-term control of inflammation. Should systemic therapy be required, then subcutaneous methotrexate is recommended over oral methotrexate in the first instance. The large majority of the recommendations within this guideline are based on either the expert opinion of the panel or on clinical studies. The only randomised controlled trial data available to support a recommendation is on the use of antitumour necrosis factor (TNF) biological therapies, where the use of a monoclonal antibody biologic is advised over etanercept, which works by acting as a decoy receptor.
Adalimumab and Dexamethasone for Treating Non-Infectious Uveitis26 is a guideline produced by the UK NICE, which is most concerned with providing guidance for medical practitioners working within the UK National Health Service. It specifically deals with the use of the biological treatment adalimumab, and with dexamethasone intravitreal implants, in cases of posterior uveitis. Within this narrow scope, its recommendations are clear and concise and were decided on by an appraisal committee, which heard evidence from clinical experts and received evidence from pharmaceutical companies. Included in this were results from randomised controlled trials.29–31 The guidance advised the use of adalimumab in cases of non-infectious posterior uveitis unresponsive to corticosteroid therapy, and dexamethasone intravitreal implant as an option if there is active posterior uveitis causing worsening vision with a risk of blindness. Expert opinion also advised that adalimumab therapy be halted if new choroidal or retinal inflammatory lesions developed, or if there was an increase in intraocular inflammation or a decrease in visual acuity by 3 or more lines or 15 letters while on treatment.
The Clinical Knowledge Summary on Uveitis28 produced by the NICE provides general recommendations on uveitis covering clinical assessment, differential diagnosis and referral. It is explicitly meant to support practitioners in primary care, and recommendations were largely drawn from review articles and medical textbooks.
Discussion
The CPGs available to help inform the WHO PECI for uveitis formed a relatively small pool. Of 496 CPGs identified by literature search, and 56 passing title and abstract screening, the large majority were not relevant to uveitis on full-text screening. Of those identified to be of relevance to uveitis, only three guidelines were of sufficient quality (based on key AGREE II item scores) to merit inclusion. This highlights an important and concerning deficiency in high-quality CPGs in the field of uveitis and may reflect the heterogeneity of the uveitis disease spectrum and the fact that most individual uveitides are relatively uncommon. Some guidelines15–18 were excluded at the screening stage owing to possible conflicts of interest as they were funded by industry partners. Industry funding of research is a common and necessary practice, but, given the intended large reach of the PECI particularly among developing nations, it was crucial to avoid any actual or potential commercial bias towards particular interventions. At the point of AGREE II scoring, the most common item for a guideline to fall short on was item 8—‘The criteria for selecting the evidence are clearly described’. Four guidelines had an average score of less than three on this point, which excluded them from inclusion (table 2). This highlights the importance of clarity on how clinical guidelines select the evidence which informs their guidance.
The diverse spectrum of disease under the umbrella of uveitis means that a single, or even a handful, of guidelines cannot comprehensively cover all disease subtypes. Although the most recent SUN working group continue to systematise the approach to disease diagnosis, classification and outcomes,26 there remain significant gaps in terms of guidelines for investigation and treatment of uveitis, particularly in adult patients. Paediatric uveitis is commonly associated with JIA and this spectrum of disease is well covered by one guideline.27 Cases of paediatric uveitis occurring without a background of JIA are, however, not covered.
Owing to the relative paucity of guidelines for uveitis, there can be little cross-checking between guidelines from different sources to assess concordance in recommendations. However, one consistent theme of two of the three included guidelines is that treatment with biologic anti- TNF agents (eg, adalimumab) is appropriate in cases with a high risk of ‘blindness’26 or ‘sight-threatening complications’.27 This guidance is largely based on expert opinion, though there are randomised controlled trials comparing Adalimumab to placebo in adult patients (VISUAL I and VISUAL II trials),30 31 which showed beneficial results. These trials did not, however, compare adalimumab to any conventional immunosuppressive therapy. The SYCAMORE trial32 did provide this comparison for paediatric uveitis associated with JIA, demonstrating a significantly lower treatment failure rate in the methotrexate plus adalimumab group compared with the methotrexate plus placebo group. This is reflected in the JIA-associated uveitis guideline chosen for inclusion here, which recommends starting methotrexate and a monoclonal antibody TNF inhibitor immediately over methotrexate as monotherapy for severe active uveitis with sight threatening complications.27
Owing to the relative rarity of many forms of uveitis, a key challenge for the development of high-quality guidelines on the treatment of these conditions is to generate the primary research on which guidelines are built. This requires high-quality randomised controlled trials, which often need to be conducted across several countries in order to meet recruitment targets. Preceding any trials of therapeutics, consensus must be reached on the definition of the condition being treated. The recent SUN criteria are a vital development in this area.33 Well-defined endpoints for trials are also needed, and standardisation of these would make cross-comparisons of new therapeutics being tested more straightforward. There is clear scope for improvement in the availability of clinical guidelines on uveitis diagnosis and management and well as the number of uveitides which are covered by guidelines. It is also apparent that separate guidelines may be appropriate for different care settings. Many patients may present first to a primary care setting, where the practitioner may have very limited training in recognising and treating eye disease. It is necessary therefore to be aware of the target audience for guidelines.
Some weaknesses remain in the design of this systematic review; the initial literature search was restricted to English language guidelines and this does create an anglocentric bias to the selected guidelines. However, this search method does keep this review in line with others completed to inform the PECI. A further limitation is that he initial search was focused on specific eye-related guidelines, which may have missed some guidelines on uveitis related to systemic inflammatory diseases (eg, the spondyloarthropathies) or infectious diseases (eg, tuberculosis and syphilis), though the search strategy did catch guidelines for uveitis associated with JIA.
Conclusion
Uveitis is an important clinical problem, with high prevalence worldwide,34 and with high visual morbidity.35 It is an umbrella term for a range of clinical entities, and the range of different aetiologies for uveitis, including infectious, autoimmune and autoinflammatory, traumatic and ischaemic causes, means that single overarching guidelines are difficult to produce. Guidance exists on the use of newer treatments such as the monoclonal antibody anti-TNF treatment adalimumab and slow release dexamethasone intravitreal implants in non-infectious posterior uveitis,26 but this covers only a small proportion of cases of uveitis, and anti-TNF treatment is only recommended for cases refractory to first line (corticosteroid) and second line (conventional immunosuppressive) therapies. However, no guidance exists on when to initiate these first- and second-line treatments. There is also a marked lack of guidance on the more common presentation of anterior uveitis; and on infectious uveitis, which can be devastating to vision.36
Designing specific guidelines for each subtype of uveitis is likely impractical, as is a single CPG to cover all uveitis. However, an achievable way of increasing coverage of uveitis by CPGs, to the benefit of patients worldwide, may be to aim for guidance on uveitides based on aetiology and/or anatomical location. Broad guidelines could cover diagnosis, treatment strategies and monitoring of several uveitis subtypes under this arrangement.
Regrettably, evidence derived from CPGs for uveitis to support the development of the WHO PECI form a small pool, and cover only a minority of the clinical presentations of uveitis in sufficient detail to help clinical decision making. Thus, there will be a greater reliance on Cochrane Systematic Reviews and expert opinion in deciding on interventions to include in the PECI. There is an urgent requirement for high-quality, evidence-based guidance on a wider range of uveitides. The COVID-19 pandemic has precipitated a necessary collaboration between clinicians around the world, including uveitis specialists, due to the need for shared experience during a period of uncertainty. This era of collaboration may accelerate larger and higher-quality studies and reviews, which would support measures such as the PECI in the future.
Ethics statements
Patient consent for publication
Acknowledgments
This publication was funded by a small educational grant from Alimera Sciences
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
NG and IRR are joint first authors.
Twitter @DrStrangetwit
NG and IRR contributed equally.
Correction notice This article has been corrected since it first published. First authorship and equally contributed statements have been added to the article.
Contributors NG and IRR are joint coauthors of this work. SK and JRE were involved in the conception and design of the study. All authors critically reviewed the manuscript and approved its submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.