Article Text

Abstract
Objective To study the visual, refractive and surgical outcomes of intraocular lens (IOL) implantation versus aphakia in children with microspherophakia.
Design Retrospective, comparative, non-randomised interventional study.
Methods All consecutive children with microspherophakia who satisfied the inclusion criteria were included. The eyes that underwent in-the-bag IOL implantation and those that were left aphakic were included in groups A and B, respectively. The postoperative visual outcomes, IOL stability and complications during the follow-up period were studied.
Results 22 eyes (13 patients, male 76%), of which 12 eyes were in group A and 10 eyes in group B. The mean±SE of age at surgery was 9.4±1.4 and 7.3±0.9 years in group A and group B, respectively (p value 0.18). The mean follow-up of group A was 0.9±0.4 years (median 0.5 years; Q1 0.04, Q3 2.16) and group B was 1.3±0.9 years (median 0.147 years; Q1 0.08, Q3 0.39) (p value 0.76). All the baseline biometric variables including best-corrected visual acuity (BCVA) were comparable in each group. The final BCVA in logMAR adjusted for follow-up was comparable in both group A (0.29±0.06) and group B (0.52±0.09) (p value 0.06). Mean predictive error of IOL power in microspherophakia was 0.17±0.43.
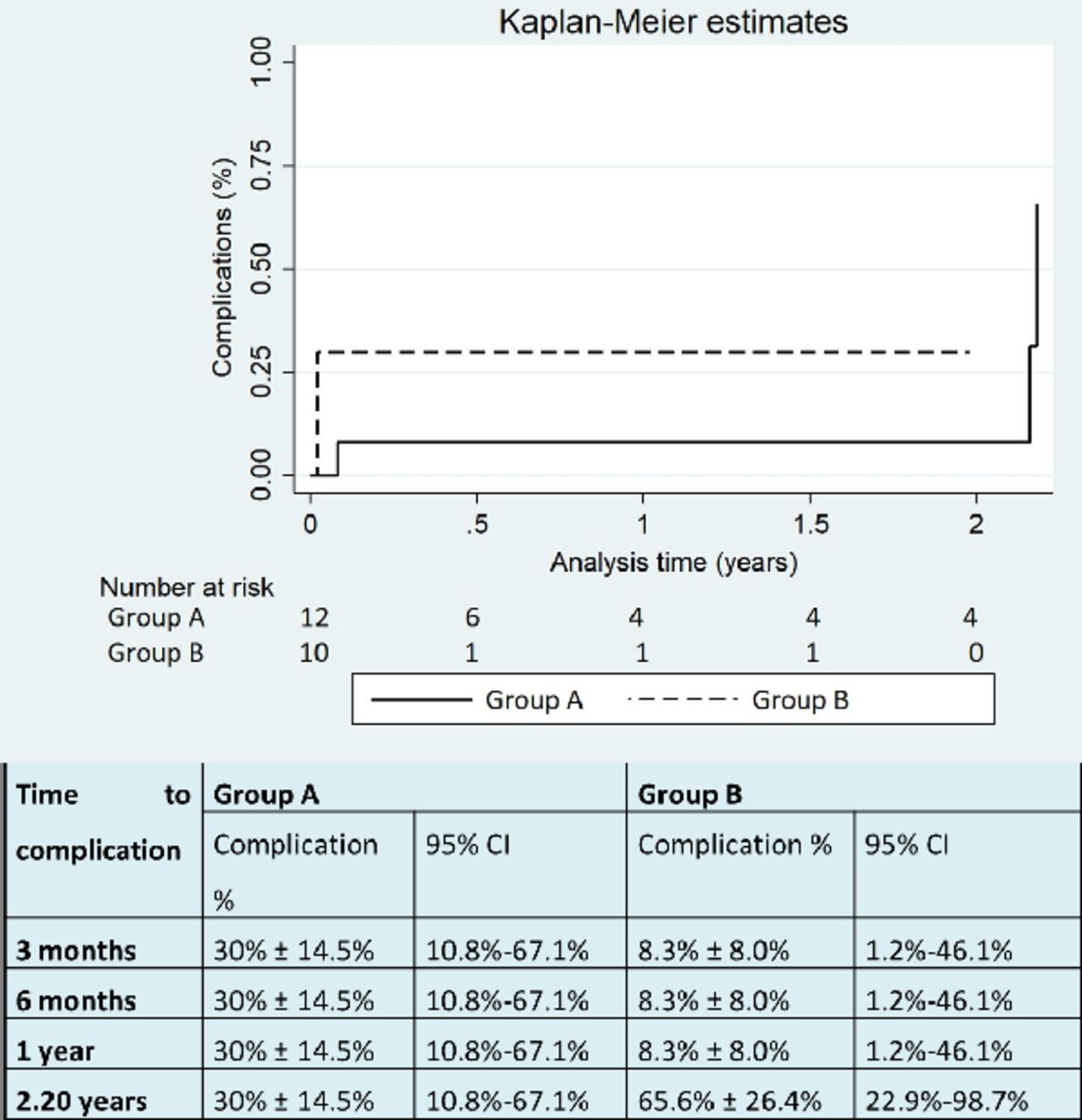
The most common complication in group A was visual axis opacification of two eyes (16.7%, 95% CI 2.9% to 49.1%), of which one eye (8.3%, 95% CI 0.4% to 40.2%) needed membranectomy. Vitreous in anterior chamber was the most common complication in group B, seen in two eyes (20%, 95% CI 3.5% to 55.8%), of which one eye (10%, 95% CI 0.5% to 45.9%) underwent YAG laser vitreolysis. The survival analysis (p value 0.18) was comparable in each group.
Conclusion In-the-bag IOL is an option, which can be considered in selected cases of microspherophakia in developing nations where regular follow-up and economic constraints are a major concern.
- lens and zonules
- child health (paediatrics)
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Microspherophakic eyes undergoing surgery can be rehabilitated using angle-supported, iris-fixated, scleral-fixated intraocular lens (IOL), although there are inherent complications to the above-said procedures.
Only sporadic case reports with variable follow-up and outcomes are reported on in-the-bag IOL implantation in microspherophakic eyes.
WHAT THIS STUDY ADDS
This study has a larger number with reasonable follow-up in patients undergoing in-the-bag IOL implantation in microspherophakic eyes.
In-the-bag IOL implantation in microspherophakic eyes is safe with comparable outcomes to ones left aphakic.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
In-the-bag IOL is a potential option in eyes with microspherophakia with strict preoperative parameters in developing nations where regular follow-up and economic constraints are a major concern, although long-term risks of IOL stability and safety outcomes are yet to be studied.
Introduction
Microspherophakia is a bilateral condition in which crystalline lens is small and spherically shaped with increased anteroposterior and reduced equatorial diameters and is associated with high lenticular myopia and defective accommodation. It can be isolated or can have systemic associations such as Weill-Marchesani syndrome, Marfan syndrome and Homocystinuria.1 2 The lens zonules become weak and stretched and can lead to intermittent angle closure causing secondary glaucoma and subluxation or dislocation.3 4 In non-subluxated/dislocated microspherophakic lenses, the risk of ametropic amblyopia due to high lenticular myopia and permanent visual loss secondary to glaucoma is as high as 51%.3 Developing nations, where regular follow-up is a major limiting factor, call for the need for early intervention in these children.
The peculiar nature of the lens makes surgery challenging and small capsular bag precludes the implantation of intraocular lens (IOL) into the capsular bag. Multiple studies have shown variable outcomes of rehabilitation with angle-supported, iris-fixated or scleral-fixated IOLs.5 6 The complications of IOL dislocation, retinal detachment, pigment dispersion glaucoma, corectopia, synechiae (associated with iris-fixated IOL), suture exposure (in scleral-fixated IOL) and increased corneal endothelial loss initiated the idea of in-the-bag implantation of IOL in microspherophakic eyes without subluxation.5 7
There are sporadic case reports on IOL implantation in the bag with variable outcomes. Use of capsular tension ring and segments to stabilise the bag for in-the-bag implantation of IOL has been described with favourable outcomes in limited follow-up period.8 Use of intraoperative iris hooks to stabilise the small bag and implantation of three-piece IOL has been described by Khokhar et al.9 Three-piece IOL placed in sulcus was found to be more stable than in-the-bag IOL in the report by Al-Haddad and Khatib.10 The improvement in higher and lower order aberrations after a sulcus implantation of three-piece IOL is reported.11 Implantation of single-piece in-the-bag IOL correcting simultaneously angle closure and lenticular myopia with limited follow-up has been reported in adult patients.12 13 In this study, we have retrospectively looked into visual outcomes and safety profile of IOL implantation in the capsular bag in children with microspherophakia.
Methods
We retrospectively reviewed the electronic medical records of children diagnosed with microspherophakia without subluxation and underwent surgery at our institute, during the period from May 2017 to March 2021 with a minimum follow-up of 6 weeks post surgery. Only children with clinically diagnosed microspherophakia with clear lens and no subluxation and normal intraocular pressure (IOP) with no sign of glaucoma were included in the study. Children with subluxated lens, cataract, raised IOP and optic disc showing glaucomatous changes were excluded from the study. Only children whose parents who agreed for IOL implantation in-the-bag were included as cases (group A) and rest of the children who were left aphakic in the control group (group B).
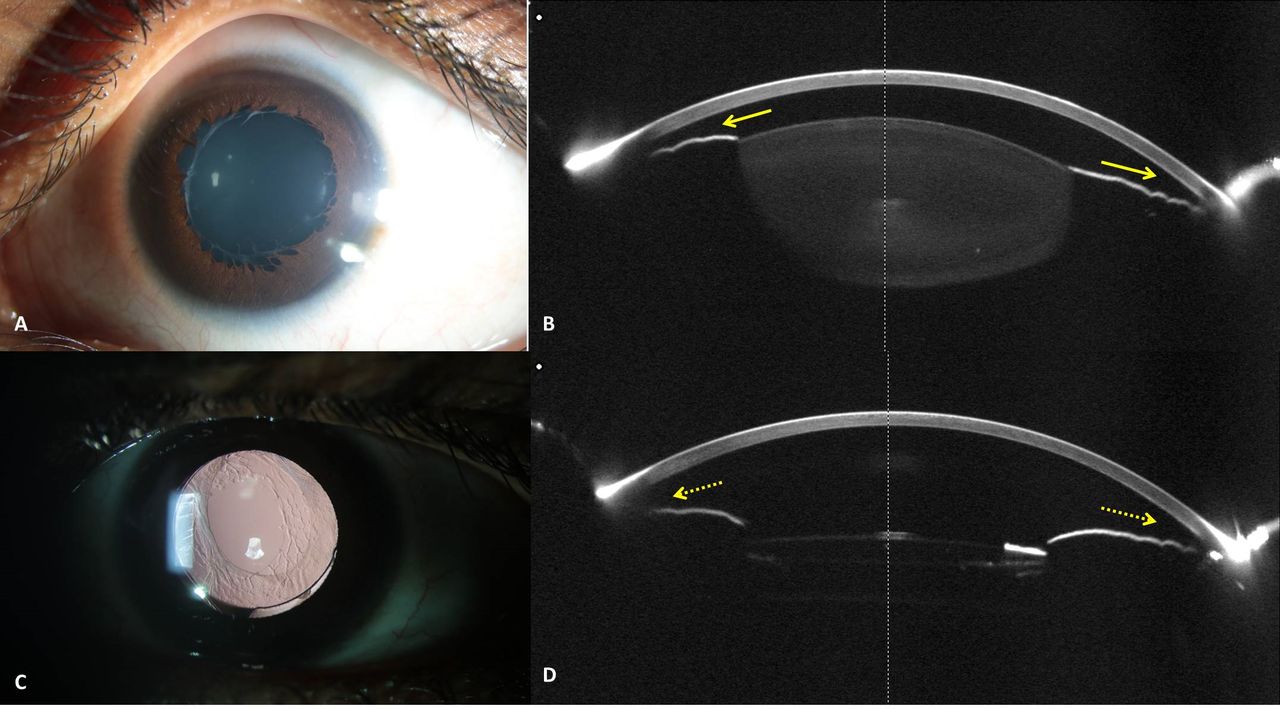
All children with confirmed microspherophakia were subjected to a comprehensive ocular examination after taking a detailed history of the presenting complaints, family history and associated systemic complaints. Details of age at presentation, age at surgery, gender, presenting complaint, best-corrected visual acuity (BCVA) and refractive error were documented. Slit lamp examination was performed to evaluate anterior chamber depth (ACD) in the centre and periphery, presence of small spherical crystalline lens and presence of subluxation. Gonioscopy (4-mirror indirect goniolens, VOLK Optical, USA) and applanation tonometry were documented. Following details were documented: clinical photographs, biometry (IOL Master 700, Carl Zeiss Meditec AG, Dublin, California, USA) for axial length, ACD, lens thickness and white-to-white horizontal corneal diameter. Oculyzer with Scheimpflug imaging (WaveLight OB820, Alcon Laboratories, Fort Worth, Texas, USA) was obtained for keratometry and to identify any mild subluxation. Optic disc photographs were documented whenever possible (figure 1). All children were evaluated for serum homocysteine levels and 2D echocardiography and were referred to paediatrician to rule out any systemic association. Pedigree was charted in all patients and genetic testing was advised to all our patients. Patients or the public were involved in the design, or conduct, or reporting, or dissemination plans of our research.
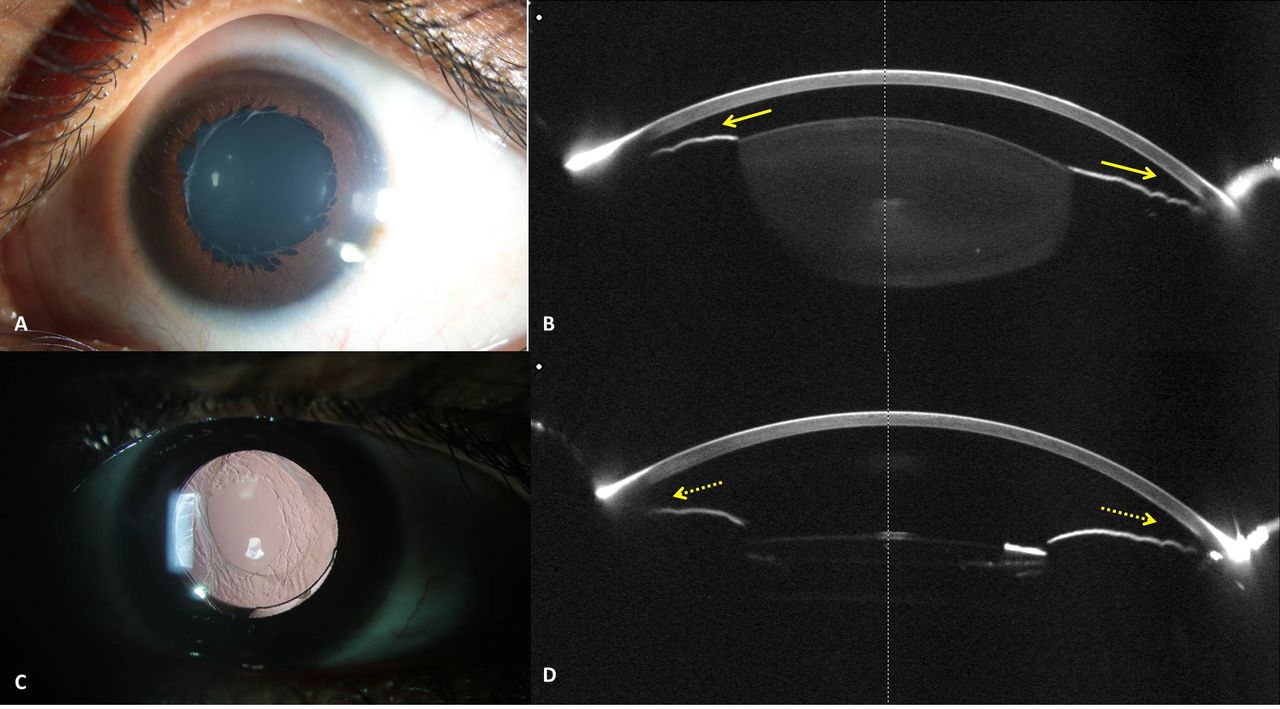
(A,B) Preoperative clinical and Scheimpflug imaging with crowding of angles (yellow arrow). (C,D) Postoperative clinical and Scheimpflug imaging with deepening of angles (dotted yellow arrow).
All surgeries were performed by a single surgeon (RK). Surgical steps are demonstrated in the online supplemental video. All the eyes in the group A underwent clear corneal main incision at 12 0'clock for IOL implantation and two limbal side ports at 3 and 9 o’clock hour and for group B only two limbal side ports were made at 3 and 9 o’clock hour for lensectomy.
Supplementary video
Hydrophobic single-piece acrylic IOL (Acrysof SA60AT, Alcon laboratories, Fort Worth, Texas, USA) was implanted in the capsular bag in pseudophakia group. IOL power was calculated using Sanders-Retzlaff-Kraff II/T formula with no under-correction as this was a pilot study and there was an unpredictability of the effective lens position after surgery. Postoperatively, topical tobramycin 0.3% or moxifloxacin 0.5% 4 times a day for 1 week, homatropine 0.5% eye drops 3 times a day for 1 week and a tapering dose of prednisolone acetate 1% 6–10 times daily with a gradual tapering over 6 weeks was prescribed to all patients. The children were examined on the first postoperative day in the clinic and 1 week later, during which sutures were removed and glasses were prescribed. The children were followed up at 1, 3, 6 and 12 months post surgery. Visual acuity, IOP and optic disc were assessed in every visit. Anterior chamber depth measured preoperatively from corneal endothelium to anterior surface of crystalline lens to postoperatively from corneal endothelium to anterior surface of IOL was compared. In addition, visual axis opacification (VAO), signs of inflammation, position of the IOL and posterior segment complication if any were noted in every visit.
Statistical analysis was done using STATA V.14.2 (StataCorp, College Station, Texas, USA). A linear mixed effects model using maximum likelihood estimation with random intercepts at the patient level was used in the data analysis to account for the correlation between fellow eyes of the same patient. The relationships between postoperative visits or groups were evaluated by mixed effects regression analysis using marginal linear predictions. A p value of <0.05 was considered statistically significant.
Results
In total, 22 eyes belonging to 13 patients satisfied the inclusion criteria during the study period and were included in the study. Ten were males (76.9%). None of the eyes had evidence of angle closure, subluxation, cataract or glaucomatous disc changes preoperatively. Of the 22 eyes, 12 eyes underwent lens aspiration with primary in-the-bag IOL implantation (group A) and 10 eyes underwent lensectomy through limbal approach and were left aphakic (group B).
Mean age at presentation was 8.9±4.0 years and 7.3±2.5 years in groups A and B, respectively (p=0.38). Mean age at surgery was 9.4±1.4 years and 7.3±0.9 years in groups A and B, respectively (p=0.18). The most common presenting complaint was the diminution of vision (8/11, 73%) followed by child taking objects close to face for viewing (3/11, 27%). Mean follow-up duration in group A was 1.1±0.3 years (median 0.5 years; Q1 0.04, Q3 2.16) and group B was 1.5±0.9 years (median 0.147 years; Q1 0.08, Q3 0.39) (p=0.65). The characteristic findings of small, spherical crystalline lens with increased anteroposterior diameter and reduced equatorial diameter were seen in all eyes in the study. Baseline axial length, average keratometry, pachymetry, ACD, white-to-white diameter and lens thickness are shown in table 1. All the biometric variables were comparable between both groups.
Preoperative biometry details of groups A and B
Familial microspherophakia was noted in two siblings (four out of six patients, first sibling group of two brothers, 5 years and 6 years, second sibling group of brother, 12 years and sister, 14 years) in the group A and one out of seven patients (daughter and mother, daughter included in the study) in group B. The remaining two patients in group A were identified as idiopathic microspherophakia. Among the remaining six patients in group B had two each of Marfan syndrome, homocystinuria and idiopathic nature.
The visual and refractive outcomes in both groups are as shown in table 2. The baseline BCVA in both groups was comparable. The final BCVA was also comparable.
The visual and refractive outcomes in group A and group B at final follow-up
As we did not plan under-correction in any eye in group A, the mean residual IOL power preoperatively was −0.04±0.10 D and the mean spherical equivalent at final visit was −0.21±0.45 D. Mean predictive error of IOL power in microspherophakia was 0.17±0.43 D. The ACD in group A deepened significantly postoperatively (p=0.000004231) as depicted in figure 1.
Intraoperatively, two eyes in group A (16.6%) had developed pupillary block and iris prolapse through the side port after IOL implantation in the bag, which settled after a peripheral surgical iridectomy. Another eye (8.3%) had developed haptic capture intraoperatively, which required redialling. None of the eyes in group B had developed intraoperative complication. In group A, VAO was noted in the first patient who was implanted IOL and the eye underwent membranectomy through the pars plana approach. Owing to the risk of VAO and difficulty of membranectomy due to pseudophakodonesis in these eyes, subsequent four patients underwent primary posterior capsulotomy and anterior vitrectomy also during the IOL implantation surgery.
The postoperative complications through the follow-up period are as shown in online supplemental table 1. None of the eyes in either group developed glaucoma through the follow-up. All the eyes in group A had pseudophakodonesis noted postoperatively with one eye developing mild IOL subluxation. The survival analysis plot for groups A and B is as shown in figure 2 (p=0.18, log-rank test).
Supplemental material
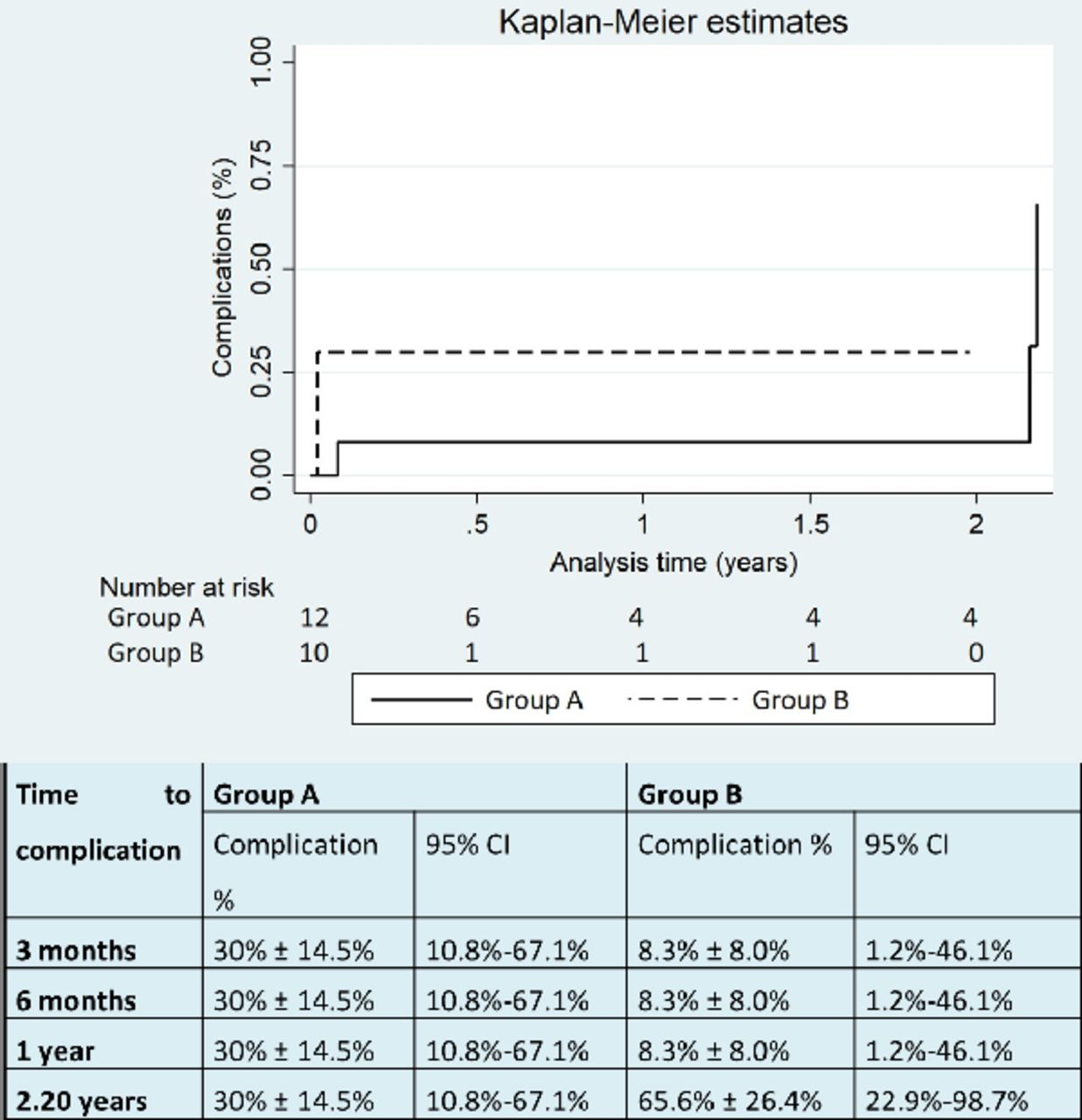
Kaplan-Meier survival analysis plot for group A and group B (log-rank test of p=0.18).
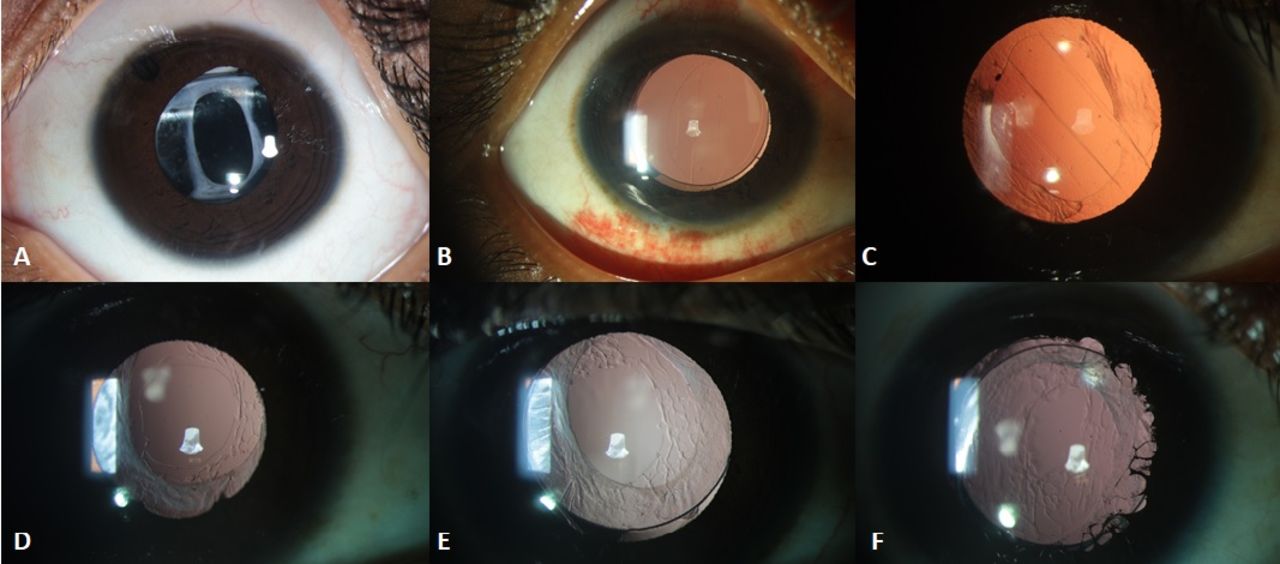
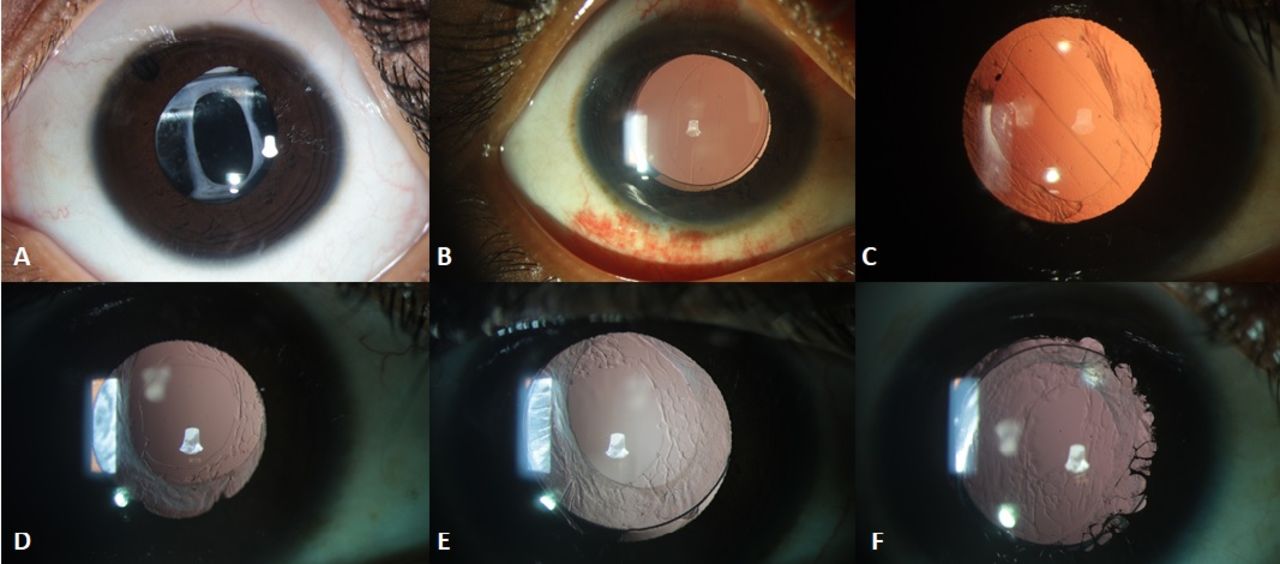
The most common complication in group A was VAO two eyes (16.7%, 95% CI 2.9% to 49.1%). The VAO noted were in the eyes that did not undergo primary posterior capsulotomy primarily. Of which one had mild grade without affecting the visual acuity and one eye (8.3%, 95% CI 0.4% to 40.2%) needed membranectomy. Mild subluxation without affecting visual acuity in undilated state was noted in one patient. Vitreous in anterior chamber was the most common complication in group B, seen in two eyes (20%, 95% CI 3.5% to 55.8%), of which one (10%, 95% CI 0.5% to 45.9%) of them needed YAG laser vitreolysis. The follow-up visit clinical picture of one eye of each patient in group A is as shown in figure 3.
{kind=link}
{kind=link}
{kind=link}
Postoperative follow-up clinical photograph of one eye of each patient of group A.
Discussion
Rehabilitation with primary IOL in eyes with microspherophakia undergoing surgery can be done using angle-supported, iris-fixated, scleral-fixated IOL.5 6 Owing to the small size and peculiar nature of capsular bag in microspherophakia, in-the-bag implantation of IOL is controversial. There are sporadic case reports on in-the-bag IOL implantation with variable outcomes in adults.12 13 The standard of care still remains leaving the eyes aphakic. To the best of our knowledge, this is the only study with larger number of patients with reasonable follow-up in patients undergoing in-the-bag IOL implantation in microspherophakic eyes. Most of the reported literatures are single case reports (online supplemental table 2).8–11 13 14
Supplemental material
In this retrospective study, strict inclusion criteria for in-the-bag IOL implantation was undertaken due to scarcity of literature on the long-term outcomes and safety profile. Patients were not randomised as it is a pilot study to understand the behaviour of in-the-bag IOL in microspherophakic eyes. The eyes that were included in the IOL group were strictly based on parents of the patients’ decision. Thus, we had two groups, group A with IOL implantation and group B that were left aphakic. This gave us an opportunity to study and compare the visual outcomes between eyes that underwent IOL implantation and those left aphakic.
The mean age at surgery was comparable in both groups in our study. Reported literature on the age of patient with primary posterior chamber IOL implantation in paediatric group, range from 4 to 14 years (online supplemental table 2).8–11 13 14 There was a male preponderance in our study, similar to the case reports cumulatively. The presenting complaints of diminution of vision and keeping objects closer to eyes in our cohort point towards uncorrected lenticular high myopia in eyes with microspherophakia. There was no statistical difference between the two groups on presenting BCVA. The individual case reports on the follow-up of eyes undergoing in-the-bag implantation of IOL range from 1 to 24 months (online supplemental table 2).8–11 13 14 Our study considering the larger number of patients has a reasonable follow-up in either group to compare the visual outcomes. Online supplemental table 2 depicts literature review of studies with their outcomes on primary IOL implantation in eyes with microspherophakia along with present study.8–11 13 14 The published literature on IOL implantation in the bag are sporadic case reports with variable outcomes. Khokhar et al described the use of capsular tension ring and segments to stabilise the bag for in-the-bag implantation of IOL and have shown favourable outcomes in limited follow-up period.8 Use of intraoperative iris hooks to stabilise the small bag and implantation of three-piece IOL has been described by Khokhar et al.9 Our study differs by using neither the capsular tension ring nor the iris hooks to stabilise the lens bag. Al-Haddad and Khatib reported three-piece IOL placed in sulcus was more stable than in-the-bag IOL.10 Implantation of single-piece in-the-bag IOL correcting simultaneously angle closure and lenticular myopia with limited follow-up has been reported in adult patients.12 13 In this study, we have retrospectively looked into visual outcomes and safety profile of IOL implantation in the capsular bag in children with microspherophakia with a reasonable follow-up.
The axial length, keratometry, pachymetry and corneal diameter were comparable in both groups giving us an opportunity to eliminate the confounding ocular characteristics that may affect the visual outcomes. The final BCVA in logMAR adjusted for follow-up was comparable in group A compared with group B. As none of the eyes in group A were not under corrected, due to unpredictability of the effective lens position in these eyes, the predictive value of refractive correction was noted to be closer to emmetropia.
The intraoperative complications of pupillary block in two eyes are explained by the positive vitreous pressure and IOL in the small spherical lenticular bag. The pupillary block was relieved by the surgical peripheral iridectomy and reducing the end-tidal carbon dioxide to less than 35 mm Hg. Due to IOL implantation in the small bag, there was haptic capture noted in one patient who required IOL redialling. The postoperative IOL position is as depicted in figure 3. Owing to the crowding of IOL in the small spherical lenticular bag, calls for further innovation on the IOL design suitable for microspherophakic eyes.
The most common complication in group A was VAO seen in two eyes, of which only one needed membranectomy. The membranectomy was done through pars plana route to avoid instability of the IOL through limbal approach. Due to difficulty of membranectomy due to pseudophakodonesis in this eye, subsequent four eyes included in the study underwent primary posterior capsulotomy. None of the case reports report this complication. As VAO developed was noted in eyes, which did not undergo primary posterior capsulotomy and anterior vitrectomy primarily, we recommend doing primary posterior capsulotomy and anterior vitrectomy in all cases to avoid this late complication and need for second surgery. IOL subluxation was seen in one eye in group A, which was mild and did not need resurgery. Two eyes in group B had vitreous in anterior camber, of which one needed Neodymium:yttrium:aluminum:garnet (Nd:YAG) laser vitreolysis. This could be due to absence of IOL barrier in aphakic eyes, and hence can be avoided with IOL implantation.
In-the-bag IOL may be considered in eyes with microspherophakia with strict preoperative parameters in developing nations where regular follow-up and economic constraints are a major concern.
The study is limited by a smaller sample size, retrospective non-randomised cohort, lack of data on preoperative lens diameter and short-term outcomes. Future prospective study with randomisation, preoperative assessment of the lens bag diameter and calculation of effective lens position postoperatively and a long-term safety profile and stability of lens-bag complex is called for. This study also gives an opportunity for innovative IOL design for eyes with microspherophakia.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Institutional Ethics Committee (Ethics Ref No LEC-BHR-R-05-21-657) and adhered to the tenets of the Declaration of Helsinki. A written informed consent was obtained from the parents of children undergoing surgery, explaining the details of evaluation, surgery performed, intraoperative challenges, possible complications associated with surgery and general anaesthesia, requirement of multiple follow-up visits and resurgery in the language comprehended by the parents.
Acknowledgments
The authors thank Mr Vishnu Murthy Gollapally for assisting in editing the surgical video.
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors GC: conduct, reporting, conception and design, acquisition of data or analysis and interpretation of data. VM: conduct, reporting, conception and design, acquisition of data or analysis and interpretation of data. AM: analysis and interpretation of data. RK: planning, conduct, reporting, conception and design, acquisition of data or analysis and interpretation of data, gurantor etc.
Funding This study was supported by Hyderabad Eye Research Foundation.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.