Article Text

Abstract
Background/aims Demonstrate that subretinal drusenoid deposits (SDDs) in age-related macular degeneration (AMD) are linked to coexistent high-risk vascular diseases (HRVDs).
Methods Cross-sectional study. Two hundred AMD subjects (aged 51–100 years; 121 women, 79 men) were recruited. Spectral domain optical coherence tomography, autofluorescence and near-infrared reflectance imaging, and lipid profiles were obtained. Subjects were assigned by health history questionnaires into those with or without HRVDs, defined as: cardiac valve defect (eg, aortic stenosis), myocardial defect (eg, myocardial infarction) and stroke/transient ischaemic attack. Masked readers assigned subjects into two groups: SDD (with or without drusen) and drusen (only). Univariate testing was performed by χ2 test. We built multivariate regression models to test relationships of coexistent HRVD to SDD status, lipid levels and other covariates.
Results The prevalence of HRVD was 41.2% (40/97) and 6.8% (7/103) in the SDD and non-SDD groups, respectively (correlation of SDD with HRVD, p=9×10−9, OR 9.62, 95% CI 4.04 to 22.91). Multivariate regressions: only SDDs and high-density lipoprotein (HDL) in the first two HDL quartiles remained significant for HRVD (p=9.8×10−5, 0.021, respectively). Multivariate regression model: SDDs and an HDL in Q1 or Q2 identified the presence of HRVD with the accuracy of 78.5%, 95% CI 72.2% to 84.0%.
Conclusions High-risk cardiovascular and neurovascular diseases were accurately identified in an AMD cohort from SDDs and HDL levels. The SDDs may be related to inadequate ocular perfusion resulting from the systemic vasculopathies. Further research with this paradigm is warranted and might reduce mortality and morbidity from vascular disease.
- Imaging
- Macula
- Retina
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Decades of studies on age-related macular degeneration (AMD), cardiovascular disease and stroke have not found consistent associations between AMD and systemic vascular disease.
WHAT THIS STUDY ADDS
This study suggests that there is in fact no general relationship, but instead a strong, specific association between only the subretinal drusenoid deposit (SDD) phenotype of AMD on retinal imaging and certain coexistent vascular diseases that are high risk for compromised cardiac output or internal carotid artery stenosis.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Future screening initiatives for these high-risk vascular diseases (HRVDs) with fast, inexpensive retinal imaging could make a significant contribution to public health and save lives. Likewise, screening patients with known HRVDs for unrecognised AMD of the SDD form could enable needed treatment and save vision.
Introduction
Cardiovascular disease (CVD) and stroke are the leading causes of death in the developed world.1 Age-related macular degeneration (AMD) is the leading cause of blindness.2 However, despite some common risk factors, large studies have not found consistent associations.3–5 In meta-analyses considering AMD and CVD (n=29 964 334) and AMD and stroke (n=1 420 978), no associations were found.6 7
We have found evidence of a novel association between a subset of high-risk vascular diseases (HRVDs, our term) and the intermediate AMD (iAMD) lesions of subretinal drusenoid deposits (SDDs). SDDs, aka reticular pseudodrusen,8 and soft drusen are the two main forms of iAMD on spectral domain optical coherence tomography (SD-OCT), above and below, respectively, the retinal pigmented epithelium (RPE) (figure 1).9 The colour photographic, autofluorescence (AF) and near-infrared reflectance (NIR) images of SDDs are characteristics (figure 1A–C). The blood supply of the RPE and outer retina, the tissues damaged in AMD, is the choroidal vasculature and choriocapillaris (CC)10 (figure 1D). SDD and drusen can occur in the same eye and can progress to either form of advanced AMD, neovascularisation and macular atrophy,11 12 for which SDDs confer twice the risk of drusen.13–15

Multimodal imaging and spectral domain optical coherence tomography (SD-OCT) imaging of subretinal drusenoid deposits (SDDs) and soft drusen in age-related macular degeneration. (A–D) Subject with SDDs in the right eye. Multimodal imaging is variably sensitivity for SDDs. (A) Colour fundus photography (CFP), relatively insensitive to SDDs, required contrast enhancement to visualise their characteristic reticular pale flecks (green border). (B) Autofluorescence detected a larger area than in CFP. SDDs are fairly homogeneous and moderately hypoautofluorescent (magenta border). (C) With near-infrared reflectance (NIR) imaging, the area detected is even larger than with autofluorescence. SDDs are fairly homogeneous and moderately hyporeflectant (blue border). (D) On SD-OCT, SDDs are hyper-reflectant material between the retinal pigment epithelium (RPE) and ellipsoid zone (EZ) in the outer retina proper (yellow arrows). The blood supply of the RPE and outer retina is the subjacent choroid. The choroidal–scleral interface follows the red dashed line. Choroidal thickness, measured from the base of the RPE to this interface is 83 μm, significantly thinner than for age-matched normals. (E–H) Subject with soft drusen in the left eye. (E) CFP shows yellowish confluent lesions close to the fovea. (F) On autofluorescence, the soft drusen have slightly hyperautofluorescent or neutral appearance. (G) NIR shows the hyper-reflectant appearance of soft drusen. (H) Soft drusen on SD-OCT are lumps of intermediate reflectivity on Bruch’s membrane elevating the RPE (blue arrows). The choroidal thickness is with the soft drusen phenotype than with SDDs, 205 μm versus 83 μm (D).
HRVDs are two cardiovascular categories: (1) myocardial (myocardial infarction (MI), coronary artery bypass grafting (CABG), congestive heart failure (CHF)) and valve defects and (2) neurovascular, stroke/transient ischaemic attack (TIA). They are all high risk for morbidity and mortality and also high risk for compromised ocular blood supply. We hypothesise that HRVDs are strongly associated with SDDs, with or without concurrent drusen, and suggest that the mechanism is compromised ocular blood supply. Herein, we support this hypothesis with retinal imaging and vascular data in SDD and drusen cohorts of AMD subjects. Thus, in the future, detection of SDDs on retinal imaging could become an easily deployed, cost-effective tool to help detect coexisting HRVDs in subjects at risk.
Methods
This was a cross-sectional study of two cohorts (SDDs and drusen only randomly selected AMD subjects for classification by retinal imaging). Slightly varying definitions of iAMD have been used; most commonly the defining lesions are soft drusen and/or SDD,16 17 which we have adopted. Known demographic, clinical and social risks for HRVD were obtained from a questionnaire, and serum risks for HRVD were drawn. Vascular histories classified subjects into HRVD and non-HRVD for statistical association with SDDs and other risks. It was a cross-sectional study conducted at two tertiary vitreoretinal referral centres in New York City, New York, USA: Vitreous Retina Macula Consultants of New York (VRM) (LAY and KBF), and Department of Ophthalmology, New York Eye and Ear Infirmary (NYEE) of Mount Sinai School of Medicine (MSSM) (RBR and RTS), from August 2019 to November 2021, with 14-month interruption from COVID-19. The institutional review board (IRB) of MSSM approved the study, IRB approval no 19-00437, which adhered to the tenets of the Declaration of Helsinki.
Inclusion criteria
Subjects were aged 51–100 years, diagnosed with iAMD in at least one eye. All subjects had the capacity to sign informed consent and complete a study-related questionnaire. However, selection bias against more infirm or less able to cooperate subjects was discouraged.
Exclusion criteria
Bilateral advanced AMD. Other retinal degenerations and retinal vascular diseases such as diabetic retinopathy, prior retinal surgery (except intravitreal injections) and/or inconclusive medical or macular diagnoses.
Demographic, clinical and social risk variables
A questionnaire covered age, gender, race/ethnicity (white/black/Hispanic/Asian), body mass index (calculated), smoking history >6 months, treated hypertension or diabetes, use of blood thinners or antilipid medications.
Vascular history for assignment to HRVD
Subjects who reported stroke/TIA, MI, CABG, angina, arrhythmia, positive stress test, positive cardiac catheterisation, stent, valve disease and CHF were the CVD and stroke group. Among them, HRVD status was assigned to two cardiovascular categories: myocardial defects (such as MI, CHF) and valve defects; and one neurovascular, stroke/TIA. These categories were determined by experts in the field (JN, MSD) as likely causes of decreased systemic or ocular perfusion. All other subjects were classified as non-HRVD. The HRVD cases were checked against medical records; valve disease was further reviewed for specific valve(s), stenosis and/or insufficiency; strokes/TIA were reviewed for laterality.
Ophthalmic history, examination and multimodal imaging
Historical variables were age of AMD onset, AMD in first-degree relatives and intravitreal injections either eye (Y/N).
All examinations and image classifications were performed uniformly by two authors (GL-G, OO-M), including slit-lamp examination for iris colour (dark/light) and lens status (phakic/pseudophakic).
Volume SD-OCT scans (27 lines, automated retinal tracking, 16 scans averaged per line, good quality at least (29–34) per the device specifications), and en face AF and NIR scans (both 30°) centred on the macula, were obtained on the Heidelberg Spectralis HRA+OCT (Heidelberg Engineering, Heidelberg, Delaware, USA). Subjects without good quality SD-OCT scans were removed. After enrolment, SD-OCT images were analysed for SDD following a published protocol.18 In the case of unilateral nAMD, all determinations were made on the fellow eye. AF and NIR images were used to confirm the presence of SDDs as depicted in figure 1.18 Soft drusen were identified by standard criteria (figure 1). Subjects were assigned to two groups: SDD (SDD either eye, ±drusen) and drusen (drusen only). Mean choroidal thickness was measured on central SD-OCT scans (figure 1).
Serum risks
Blood samples for risk biomarkers of ASD19 (high-density lipoprotein (HDL), low-density lipoprotein (LDL), triglycerides) and high-sensitivity C reactive protein (hsCRP) were rapidly centrifuged at 1800g for 10 min and refrigerated. Fasting is no longer considered necessary for lipid levels,20 which were measured (Quest Diagnostics, Teterboro, New Jersey, USA) by spectrophotometry, and plasma levels of hsCRP by Immunoturbidimetric Assay (Orion Diagnostica, Finland).
Power calculation, statistics and study outcomes
Reported ORs for SDD versus drusen for any coronary artery disease (CAD) were 2:1,11 and for any AMD versus no AMD were also 2:1 for severe versus mild CAD.21 Hence, we estimated an OR of 4:1 for SDD versus drusen for severe versus mild CAD. Comparing 100 SDDs to 100 drusen, subjects yields power of 80% to detect an OR of at least 2.0 at alpha=0.05.
Univariate statistics for continuous variables with >30 samples were two-tailed t-tests and quartiles otherwise, and χ2 for categorical variables. Significant continuous variables were converted to quartile categories for multivariate testing, which then corrected the significance of each covariate for all others. Primary outcomes were thus 23 univariate and 1 standard multivariate correlation of SDD status (Y/N) and all 22 listed demographic, ocular, clinical and systemic risks with HRVD. Secondary outcomes were 23 univariate and 1 multivariate correlations of HRVD status and all 22 other risk variables with SDD status. Data scientists (AB and AG) used ‘IBM SPSS Statistics V.27’, ‘Waikato Environment for Knowledge Analysis (WEKA) V.3.8.5’, a data modelling tool and Microsoft Excel 365. Significance was set at p<0.05. Subjects with discordant iris colour (none) or lens status (17) were removed from univariate statistics for these variables. Variables that retained multivariate significance p<0.05 were then entered into a standard linear regression model for HRVD risk, with coefficients that maximised the adjusted R-squared statistic. Final study outcomes were accuracy, specificity and sensitivity of the final model for HRVD risk with 95% CIs.
Results
Patient selection, demographics and clinical characteristics
A total of 239 AMD subjects were randomly selected from the two centres and examined for eligibility, of whom 25 were excluded for not having iAMD in at least one eye and 7 for inadequate OCT scan quality. Seven declined to participate, leaving 200 study participants (87 at VRM, 113 at NYEE; 79 men and 121 women) who completed all study procedures with no missing data. Ninety-seven had SDDs present and 103 only drusen, mean ages matched at 80.3 and 78.3 years. The associations of demographic, social, ocular and clinical characteristics of SDD versus drusen subjects or HRVD versus non-HRVD subjects were not significantly different, except anticoagulant use (53%, 36%, p=0.021), and thinner choroids were significantly associated with SDDs (range, all eyes, 41–422 μm; mean OU SDD 156±59, drusen 204±76, p<0.001). Anticoagulant and antilipid medication use were significantly associated with HRVD versus non-HRVD (p=0.006, p=0.034, respectively).
Systemic risks
All groups had size 47 or greater. Mean lipid and hsCRP values for SDD and drusen subjects were not significantly different, except mean HDL was lower in SDD subjects (59±16, 66±21, p=0.01, t-test), as previously reported.22 For HRVD versus non-HRVD, only mean HDL was significant (HRVD 58.46±13.9, non-HRVD 64.5±20.0, p=0.01, t-test).
Quartile ranges for HDL in 47 HRVD and 153 non-HRVD were (38, 48.5, 56, 67, 95) and (27, 50, 63, 74, 108), respectively, medians 56 and 63. Quartile ranges for all HDL were (27, 49, 61, 72, 108), defining two categorical variables: HDL4 with four classes (Q1, Q2, Q3, Q4); and binary HDL2 with two classes (Q1 and Q2 combined) and (Q3 and Q4 combined). (Q1 and Q2) in HDL2 was significant for HRVD versus non-HRVD (p=0.012).
Vascular conditions
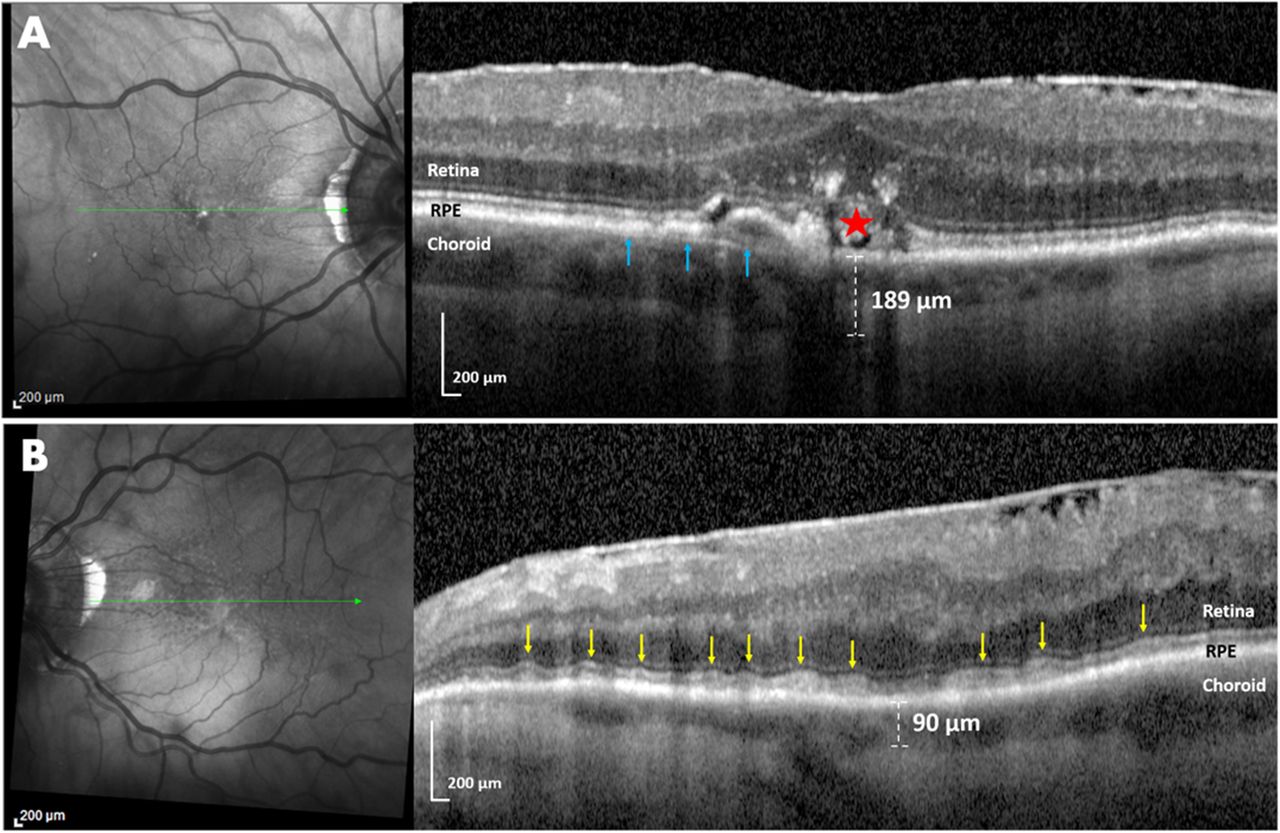
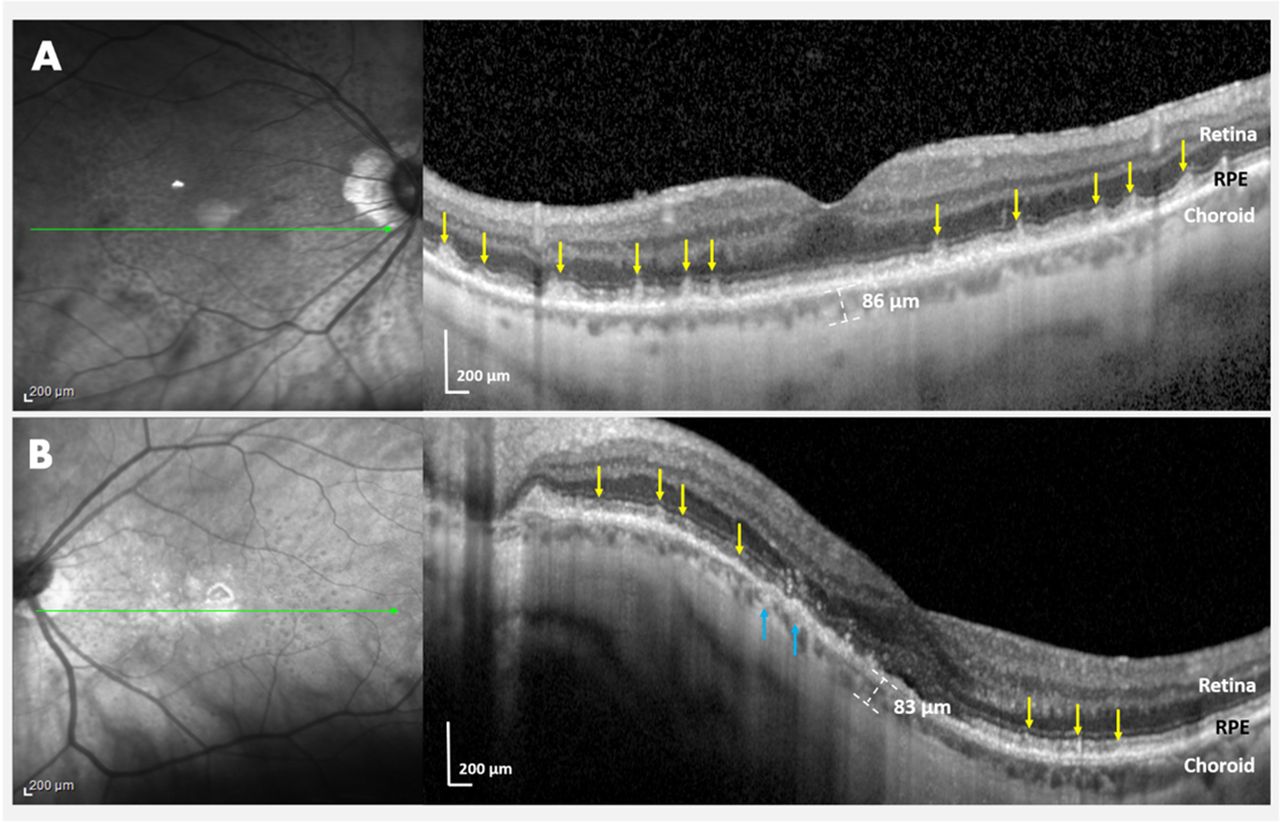
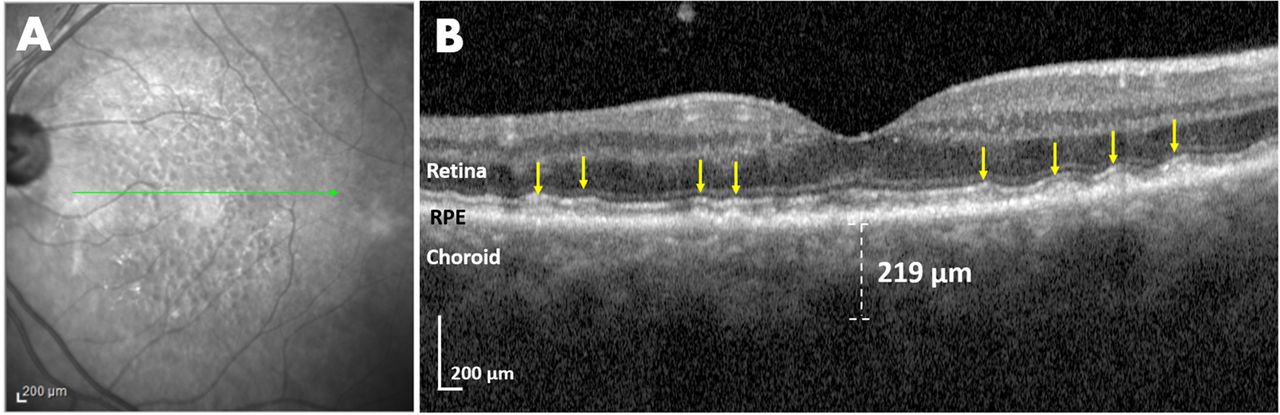
Total CVD and stroke subjects were 81. Total HRVD subjects were 47: 40/47 had SDDs and 7/47 had drusen only. Total non-HRVD subjects were 153, 57/153 SDD, 96/153 drusen only, OR for HRVD given SDD 9.62, 95% CI 4.04 to 22.91; p=9×10−9. The HRVD subgroups were 17 valve defects, 14/17 SDD; 19 myocardial defects, 16/19 SDD; 11 stroke/TIA, 10/11 SDD. Individual diseases in each category are listed in table 1. Examples: figure 2, left-sided stroke, left ICA stenosis and SDDs OS only; figure 3, MI, bilateral pure SDDs (no drusen); figure 4, aortic stenosis, pure SDDs. All subjects are 75–85 years old.
High-risk vascular diseases (HRVDs) and subretinal drusenoid deposits by HRVD category

Near-infrared reflectance (NIR) and spectral domain optical coherence tomography (SD-OCT) imaging of a subject with left-sided stroke, left internal carotid artery (ICA) stenosis and ipsilateral pure subretinal drusenoid deposits (SDDs). (A) Right eye. NIR imaging (left) showed a few hyper-reflective foci suggestive of drusen (green line, location of OCT scan). SD-OCT (right) revealed confluent soft drusen (blue arrows) and overlying retinal pigment epithelium (RPE) disruption and migration (red star). Subfoveal choroidal thickness was 189 μm. (B) Left eye. NIR (left) showed a well-defined group of homogeneous hyporeflectant lesions, typical of SDDs (green line, location of SD-OCT scan). SD-OCT scan (left) revealed multiple smooth confluent hyper-reflective lesions (‘ribbons’ pattern, yellow arrows) between the RPE and ellipsoid zone (EZ) and a subfoveal choroidal thickness of 90 μm. There are no drusen. Note that the structural features of SDDs and choroidal thinning are present purely and exclusively in the left eye, where the perfusion of the choroid by the ophthalmic artery may be compromised by ICA stenosis. This supports hypoperfusion as a mechanism for SDDs, a perfect experiment in nature in which stenosis of one ICA produced SDDs only ipsilaterally.

Near-infrared reflectance (NIR) and spectral domain optical coherence tomography (SD-OCT) imaging of a subject with high myopia, myocardial deficiency due to myocardial infarction (MI) and bilateral subretinal drusenoid deposits (SDDs). (A) Right eye. NIR imaging (left) showed myriad homogeneous hyporeflectant lesions, typical of SDDs (green lines, location of OCT scan). SD-OCT scan (right) revealed SDDs as multiple hyper-reflective subretinal lesions (yellow arrows) with a conical appearance (‘dots’ pattern) above the retinal pigment epithelium (RPE), distorting (stage 2) and penetrating (stage 3) the ellipsoid zone (EZ) and a thin choroid of 86 μm. (B) Left eye. NIR imaging (left) showed myriad homogeneous hyporeflectant SDDs. SD-OCT (right). The curvature of the scan is due to a posterior staphyloma. The SDDs are multiple discrete hyper-reflective lesions between the RPE and EZ, again in a ‘dots’ pattern (yellow arrows). Few drusen are seen (blue arrows). There is a thin choroid of 83 μm. Marked choroidal thinning OU in this subject has risk factors of both high myopia and SDDs. The myriad SDDs OU, seldom seen in high myopia with choroidal thinning per se, are ascribed to the choriocapillaris insufficiency resulting from myocardial deficiency post-MI.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Near-infrared reflectance (NIR) and spectral domain optical coherence tomography (SD-OCT) imaging of the left eye of a subject with severe aortic stenosis, no systemic atherosclerosis and pure subretinal drusenoid deposits (SDDs). (A) NIR imaging showed the typical SDD pattern of multiple hyporeflectant lesions, some with hyper-reflectant centres (target pattern). Green line, location of SD-OCT scan. (B) SD-OCT scan revealed a pure SDD phenotype, multiple discrete hyper-reflective lesions (‘dots’, left) with a conical appearance above the retinal pigment epithelium, distorting the ellipsoid zone, and a smoother wave like series of subretinal lesions (‘ribbons’, right) (yellow arrows), with no sign of drusen. The subject has 8 diopters of hyperopia, which can produce ~50 μm of choroidal thickening over emmetropic controls. The measured choroidal thickness of 219 μm corrected for refractive error is thus ~169 μm, more typical for SDDs with choroidal insufficiency. Right eye was not evaluable due to a chronic neovascular glaucoma following an ischaemic central vein occlusion.
Multivariate regression and data modeling
Multivariate regression for HRVD risk, controlling for all significant categorical variables in Methods section, including HDL2, found SDD status, blood thinners and HDL2 remained significant (p=9.8×10−5, 0.010 and 0.021, respectively). Blood thinners correlate with HRVD because they are a treatment, hence were excluded from the final regression equation (Eqn 1) for HRVD risk, built on the binary variables SDD status and HDL2.
Eqn 1. HRVD = −0.62+[HDL2 = (Q1 and Q2)]*0.1+[SDD]*0.6
In this model, HRVD is predicted positive if both HDL is less than the median 61 and the subject has SDDs and is predicted negative otherwise.
The model achieved specificity of 83.0%, sensitivity of 63.8% and accuracy of 78.5%.
95% CIs 76.1% to 88.6%, 48.5% to 77.3%, 72.2% to 84.0%, respectively.
Multivariate regression for SDD risk found only HRVD status significant, p=0.000333.
Discussion
Within all cardiovascular and neurovascular diseases, we have identified certain HRVDs that are both high risk systemically for mortality and morbidity and also high risk for compromised ocular perfusion. The HRVDs are cardiac diseases (valve defects, MI, CABG, CHF) and stroke/TIA. Our data support the hypothesis that within AMD, only SDDs, with or without drusen, are biomarkers for coexistent HRVDs. In the literature, there is a historic finding of the Wisconsin Study that SDDs are associated with decreased longevity,15 compared with drusen. The association of SDDs, not drusen, with life-threatening HRVDs is consistent with and could now explain this finding. A specific HRVD is MI from CAD. The reduced systemic perfusion from the MI is a risk for compromised ocular perfusion. In 38 cardiovascular subjects with and without documented CAD and without known maculopathy, we found a significant association of CAD with SDDs on SD-OCT imaging.11 Recently, preliminary data (126 subjects) for the present study demonstrated a strong association between the broad category of CVD and stroke (not the specific HRVDs studied herein) and subjects with SDDs.22 To the best of our knowledge, this is the first demonstration of an association of vascular disease with a lesion of AMD.
We further hypothesise, and the data are also consistent with, a straightforward vascular mechanism for the association: the inadequate ophthalmic perfusion associated with HRVDs drives SDDs. SDDs form in the photoreceptor (PR) layer (figure 1), whose blood supply is the CC.10 The PRs, with the highest demand for O2, per unit mass in the body,23 are supplied by the choroid, which has the greatest blood flow per unit mass.24 We thus hypothesise that SDDs result from hypoxaemic damage to these vulnerable PRs due to HRVD-associated perfusion deficits.
Because the ophthalmic artery (OA) is the main blood supply of the retina and choroid, our hypothesis also includes inadequate OA perfusion. The fact that the CC is particularly vulnerable to inadequate OA perfusion adds physiological consistency to these hypotheses. As demonstrated by Hayreh, the choroid is an end-arterial system supplying CC lobules10 without adjacent anastomoses. This places these lobules at particular risk. Second, the retinal circulation derives protection from inadequate OA perfusion by autoregulation, which is not present in the choroid.25 The literature also confirms choroidal abnormalities in the setting of CAD. We showed CAD was associated with generalised choroidal thinning,12 confirmed by a later study with OCTA that also documented CC insufficiency.26
Inadequate OA perfusion in AMD was demonstrated by magnetic resonance angiography, with further reduction in advanced AMD,27 consistent with our vascular hypothesis. Further direct evidence came from improved choroidal vascular indices following ipsilateral carotid endarterectomy.28 Even more directly, OA angioplasty has been performed for advanced AMD with good results reported, again consistent with our hypothesis.29
However, relationships of SDDs to CC insufficiency30 remain controversial. Hence, although we have proposed combining CC insufficiency and SDDs as the reticular macular disease phenotype of AMD,11 we have confined this report to SDDs and associations with HRVD, without claiming, or depending on, any mechanism. Hence, all statistical results and risk models from the data are also independent of the proposed mechanism.
In this paradigm HRVD and SDDs share risk factors, for example, hypertension, but do not share mechanisms: the mechanism of an HRVD may be atherosclerotic disease (ASD), but the HRVD, in turn, is the perfusion-based mechanism for SDDs. Thus, ASD is quite rare in the OA itself,31 but perfusion of the OA, the first intracranial branch of the internal carotid artery (ICA), is vulnerable to plaque in the ICA.
Bilateral SDDs in this study were also found associated with compromised cardiac output from causes other than ASD. There was one case of idiopathic CHF and 14 of valvular disease (table 1). To the best of our knowledge, this is the first reported association of any AMD lesion with cardiac valve defects.
Cholesterol has roles in both AMD and ASD. However, drusen dynamics are now correctly associated with local lipid pathways and lipid genetics,9 and not with atherosclerosis. The risk marker of low-serum HDL for ASD actually runs contrary for AMD, with higher HDL increasing AMD risk.32 This may now be clarified: high HDL was only established as a risk for drusen, because prior studies used colour photography, which is sensitive to drusen but not SDD.32 Low HDL is a risk for ASD, which in its HRVD forms is a risk for SDD, the other iAMD lesion. Hence, low HDL is a risk for SDDs, as demonstrated. Thus, HDL effect on AMD depends on the AMD lesion, drusen or SDD. The well-known risk of high LDL for ASD, however, translated into statin use if needed in our private clinics, without multivariate significance.
The further finding that lower HDL and SDDs are significantly and independently associated with HRVD is consistent with cardiovascular literature: increasing HDL confers increasing protection against ASD between HDL levels 35 and 60, but not beyond.33 No other covariates showed risks for the presence of HRVD with multivariate adjustment. The corresponding risk model displayed good accuracy, sensitivity and specificity. Future work should consider all the main vascular serum risks, which may vary in significance across age, gender and ethnicity.
Many lines of evidence suggest SDDs are markers for a retinal disease distinct from drusen22 and may even, like diabetic retinopathy, be a retinal disease driven by systemic vascular disease. Examples of pure SDDs from the three major HRVDs are shown in figures 2–4, respectively. The vascular paradigm for SDDs also helps explain the preponderance of women (~85%) among older AMD subjects with SDDs.11 18 The significantly earlier death of men from HRVD1 and the strong linkage of HRVD with SDDs found herein would make female preponderance of SDDs in later years more likely.
The study has several limitations. Selection bias against elderly and infirm subjects was discouraged but may have reduced CVD and stroke numbers. These, however, totalled 81/200, with 47/200 HRVD, spread across multiple disorders, which supported robust associations. The elderly mean age of ~80 years in both SDD and pure drusen groups also suggests our policies were effective. The multivariate regression model for HRVD has not yet been tested on a separate dataset. This would be required for population screening. For example, the results from this moderate-sized, mostly Caucasian elderly cohort invite replication in larger and diverse cohorts, for example, in Asians, with the prevalent polypoidal vasculopathy form of AMD,34 and in the disadvantaged, with excess CAD mortality.35 LDL might well have a stronger association with HRVD in the underserved. Vascular histories were patient reported, and HRVDs were verified from medical records. However, disease metrics such as cardiac ejection fraction and per cent ICA stenosis would have helped interpreting the results and should be included in future studies.
Strengths of this cross-sectional study at two tertiary retina referral centres include rigorous patient selection and AMD phenotyping with high-quality multimodal imaging for drusen and SDD, and contemporaneous lipid levels. The strong associations found between HRVD and SDDs suggest that the targeted subsets of vascular disease and AMD were the correct ones to answer old questions.3–5 Further, these associations can all be explained by a single vascular mechanism: systemic vasculopathy driving CC insufficiency. However, the data, which strongly associated HRVD with the presence of SDDs after the correction for multiple known risks, are independent of a particular mechanism. Hence, larger and detailed studies from both the ophthalmic and vascular perspectives are warranted to explore the mechanism and assess the full impact of these findings. In particular, the detection of SDDs in women could prompt evaluation for undiagnosed CAD, a serious issue in women’s health.36 37
In summary, the strong associations found herein between HRVD and SDDs in AMD subjects warrant validation on larger and varied cohorts, which in turn might lead to inexpensive screening for HRVD in population and eye clinics. The care of HRVD might likewise include retinal imaging for SDDs, with their high risk of AMD progression.13–15 Such programmes could be high impact initiatives in public health for the reduction of mortality, morbidity and blindness.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the institutional review board (IRB) of MSSM (IRB approval no 19-00437). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are grateful to Professor Sohan Singh Hayreh for critical review of the manuscript.
References
Footnotes
GL-G and OO-M are joint first authors.
GL-G and OO-M contributed equally.
Contributors GL-G, OO-M, SA, YT and LAY: acquisition of data, analysis and interpretation of data, manuscript preparation. KT, MS, CY, AD and RR: acquisition of data. HL and MK: acquisition of data, analysis and interpretation of data. CP, KBF and RTS: design, acquisition of data, analysis and interpretation of data, manuscript preparation. AG and AB: design, analysis and interpretation of data, manuscript preparation. MSD and JN: design. GL: manuscript preparation. RBR: acquisition of data. RTS, Guarantor.
Funding Regeneron Pharmaceuticals Investigator-Initiated Study, Research to Prevent Blindness Challenge Grant (RTS and RBR), Macula Foundation (KBF), Bayer-Global Ophthalmology Awards (GL-G), International Council of Ophthalmology-Alcon Fellowship (OO-M) and New York Eye and Ear Infirmary Foundation (SA).
Disclaimer The funders played no role in the design or execution of the study.
Competing interests RBR is a consultant to OptoVue, Boehringer-Ingelheim, Astellas, Genentech-Roche, NanoRetina, OD-OS, Regeneron, Bayer, Diopsys and Teva. He has personal financial interests in Opticology, Guardion and CellView. KBF is a consultant to Regeneron, Allergan, Zeiss, Bayer, Heidelberg Engineering and Novartis. He receives research funding from Genentech/Roche. RTS is a consultant to Ora Technologies. The remaining authors have no relevant disclosures.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.