Article Text

Abstract
Objectives To develop a new dye formulation for vitreoretinal surgery, which shows increased transparency for better intraoperative handling with better parameters important for use.
Methods and analysis A new blue dye, DDG, was synthesised and tested for toxicity and staining. Diglycerol as new density-increasing additive was identified, and its toxicity and lack of influence of the staining with trypan blue (TB) on a collagen membrane as model for the epiretinal membrane was determined. Transparency of the dye solution was evaluated.
Results DDG is as alternative to Brilliant Blue G (BBG), with good staining properties for interna limitans models, and a good safety profile. Diglycerol is a new non-toxic additive replacing PEG3350, with reduced viscosity and no reduction in staining, allowing the reduction of TB to achieve the same staining level of the collagen membrane by 40%, with greater transparency of the dye solution and reduced viscosity. Both factors should facilitate a safe removal during surgery.
Conclusion A new dye preparation with improved performance in comparison to marketed combinations of BBG and TB was developed. Its reduced TB concentration and viscosity with maintained density allow better tolerance and handling.
- retina
- treatment surgery
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Trypan blue is a good stain for epiretinal membranes in vitreoretinal surgery. As its concentration is high, the fundus of the eye cannot be seen when the dye is present, which represents a risk to the patient.
WHAT THIS STUDY ADDS
By changing the agent necessary for sinking, from a polymer to diglycerol as a small additive, trypan blue concentration can be reduced.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Diglycerol allows to reduce the trypan blue concentration, making the solution more transparent, and inherently safer to use.
Introduction
For identifying epiretinal structures in vitreoretinal surgery, the present standard is to stain the structures before removal. For staining of the membrana interna limitans (ILM), Brilliant Blue G (BBG) is used mostly as standalone application. In addressing epiretinal membranes (ERM), trypan blue (TB) is most frequently applied, but it is not able to stain the ILM. Therefore, the combination of BBG and TB is the present standard as concomitant dyes.
The light blue BBG in commercial preparations has a concentration of 0.025% (w/v), allowing the surgeon to see the fundus during staining and removal of the dye solution. TB in commercially available staining solutions has a concentration of 0.15% (w/v) and is very dark blue, which allows no distance check to the sensitive surface of the ganglion cell layer, leading to the risk of inadvertently damaging the retina while aspirating excess dye.
For allowing the dye to settle rapidly on the fundus, mannitol, heavy water or polymers are in use. Disadvantage of polymeric substances is their property to abolish staining capacity, and in our observation, the polymer polyethylene glycol (PEG) acts as detergent. Mannitol is used clinically as hyperosmolar agent, and it, therefore, also influences the retinal cells. Therefore, we searched for a low-molecular weight substitute with less effect on staining (and less effect on the osmotic pressure felt by cells), in order to reduce the TB concentration and increase the transparency of the dye solution.
As the use of BBG for ocular use is patent protected,1 2 we have, therefore, synthesised another dye (DDG), with better characteristics in combination with TB.
Materials and methods
Synthesis of DDG
DDG was prepared as described in the online supplemental information. The dye, as sodium salt, is well soluble (well beyond the limits needed for staining) in water and phosphate-buffered saline (PBS).
Supplemental material
Dye solutions
Solutions with 0.02% DDG in PBS with diglycerol (Innovy, Brussels, Belgium) at 2.6%, either alone (single posterior dye, SPD) or in the presence of 0.09% TB (double posterior dye, DPD) were prepared under good laboratory practice conditions by an external company. TB was purified extensively from impurities.
For other dye solutions, see online supplemental information.
Evaluation of sinking
Sinking was recorded by a camcorder while injecting small amounts (10 µL total) into a 1 cm cuvette filled with PBS.
Staining models and their evaluation
A filter-membrane model and proteins on plastic were used. For details, see online supplemental information.
Evaluation of toxicity and phototoxicity
Toxicity and phototoxicity were evaluated as described before.3 See also online supplemental information for details.
F-test and t test data were computed using the proper Excel functions.
Evaluation of live-dead staining
Calcein-acetoxymethyl ester (living cells) and propidium iodide (dead cells) were used. For details, see online supplemental information.
Evaluation of transparency
An eye model (Fundus ADV, Bioniko, Miami, Florida) with a photorealistic fundus and a wedge-shaped cuvette were used. For details, see online supplemental information.
Patient and public involvement
Patients or the public were not involved in this laboratory work.
Results
Toxicity of DDG
The dye was found to be non-toxic in clinically relevant concentrations (see table 1). No significant difference in toxicity was observed between DDG and BBG at equal concentrations. As DDG differs from BBG only by a single methylene group (the ethoxy substituent of BBG has been changed to a methoxy substituent in DDG), this is not unexpected.
Survival (in per cent) and SD for the different exposures to the two dyes at the indicated concentrations, and results of F-test and t-test comparisons
Using the ISO 10 993–5 20094 criteria for toxicity (cell survival <70%), DDG is not toxic. With the same criteria, BBG is also non-toxic, in agreement with the literature data.3 With respect to toxicity, DDG and BBG are, therefore, equivalent.
Staining by DDG in models
Before clinical trials can be performed, staining by the new preparations in model systems should be known. The model systems used were a PVDF (polyvinylidene difluoride) filter to mimic the ILM, and a collagen type I membrane to mimic the ERM. Additionally, we used proteins adsorbed to a plastic surface for components of the ILM.
The filter-membrane model appeared being a good and ethically unproblematic substitute for the staining of tissues in patients (see figure 1). We, therefore, used it for comparing the properties of the new dye preparations with the dyes presently used.

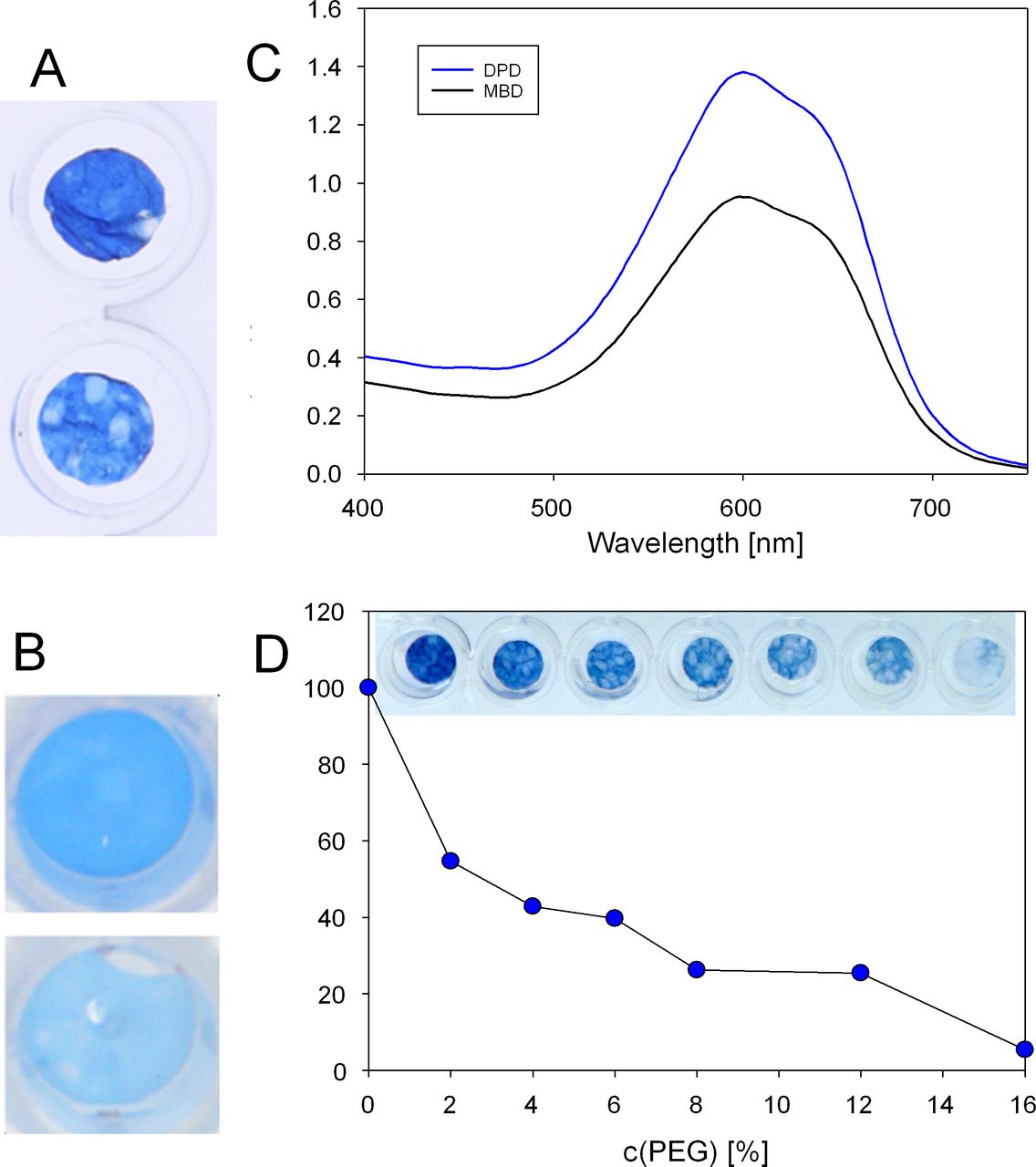
(A) Photos of membranes stained with DPD (dual posterior dye) (top) and MBD (Membrane Blue Dual) (bottom). (B) Photos of filters stained with DPD (top) and MBD (bottom). (C) Absorbance spectra of membranes stained with DPD and MBD. (D) Photo of membranes and absorbance of dimethylsulfoxide extracts stained with TB in the presence of increasing concentrations of PEG. DPD, double posterior dye; PEG, polyethylene glycol; TB, trypan blue.
A representation of the staining is shown in figure 1. As expected, the membrane is stained strongly only by the two TB-containing dyes MBD (Membrane Blue Dual) and DPD. Staining of the membrane by DPD, with a TB concentration of 0.09%, is at least as strong as staining by MBD, which contains TB at 0.15%. The staining of the membrane is about 40% higher with DPD than with MBD. DDG as stain for the ILM in DPD stains the filter better than BBG, which is the stain in MBD for the ILM. Clinical trials will have to show whether this is true also for human ILM.
Staining in the presence of excipients
As mentioned in the introduction, we saw a dramatic decrease on the staining ability of TB with polymers such as Kollidon VA64 and Kolliphor HS 15 and also with PEG3350; PEG inhibits the staining increasingly with increasing molecular weight (data not shown). Staining of the collagen membrane by TB in combination with TB (dye concentrations as in MBD) in the presence of PEG3350 shows a considerable decrease with increasing PEG concentration, already at concentrations of a few per cent (see online supplemental figure S6). Exchanging polymeric PEG for non-polymeric DG, therefore, allows to reduce the concentration of TB in the staining solutions, and as consequence increases the transparency. We could not find an influence of diglycerol on the staining ability of the dyes.
Staining of proteins on surfaces
As the ILM consists of proteins and we presume that these proteins are stained by the different dyes (TB, BBG, DDG and their combinations), we checked staining of proteins adsorbed to plastic surfaces. Individual proteins and protein mixtures were tested. Results are shown in online supplemental figure S5. Absorbance at around 600 nm is due to the blue dyes BBG and TB. TB is known to stain the ERM well, and ERM contains newly formed collagen type I.5 Literature data showed the presence of a number of different proteins (collagen IV, laminin-I, nidogen, perlecan, collagen XVIII and agrin) in the ILM.6 Collagen IV and laminin-I were used here.
The staining of protein surfaces by all TB-containing dyes is stronger than that of the triphenylmethyl dyes DDG and BBG. There are, however, differences between the two excipients with respect to staining with TB: DPD with only 60% of the TB present in MBD, stains at least equal to MBD (collagen IV, laminin, laminin/fibronectin/collagen IV) and surpasses that of MBD for the other proteins, including collagen I. As PEG reduces the staining of collagen I membranes (see online supplemental figure S5), this is not surprising. SPD stains proteins better than ILB, with the exception of collagen I.
BBG has been shown before to stain only dead cells.7 We found this also for DDG (see online supplemental figure S8). DDG, therefore, behaves as BBG in this respect.7
Sinking of dye preparations
For clinical applications, the dye solutions should sink rapidly to the bottom of the liquid-filled eye. Sinking was tested by injecting simultaneously 10 µL of DPD, parallel with 10 µL of MBD, into 1 cm optical cuvettes filled with PBS (see online supplemental video). A snapshot is shown in figure 2.
Supplementary video
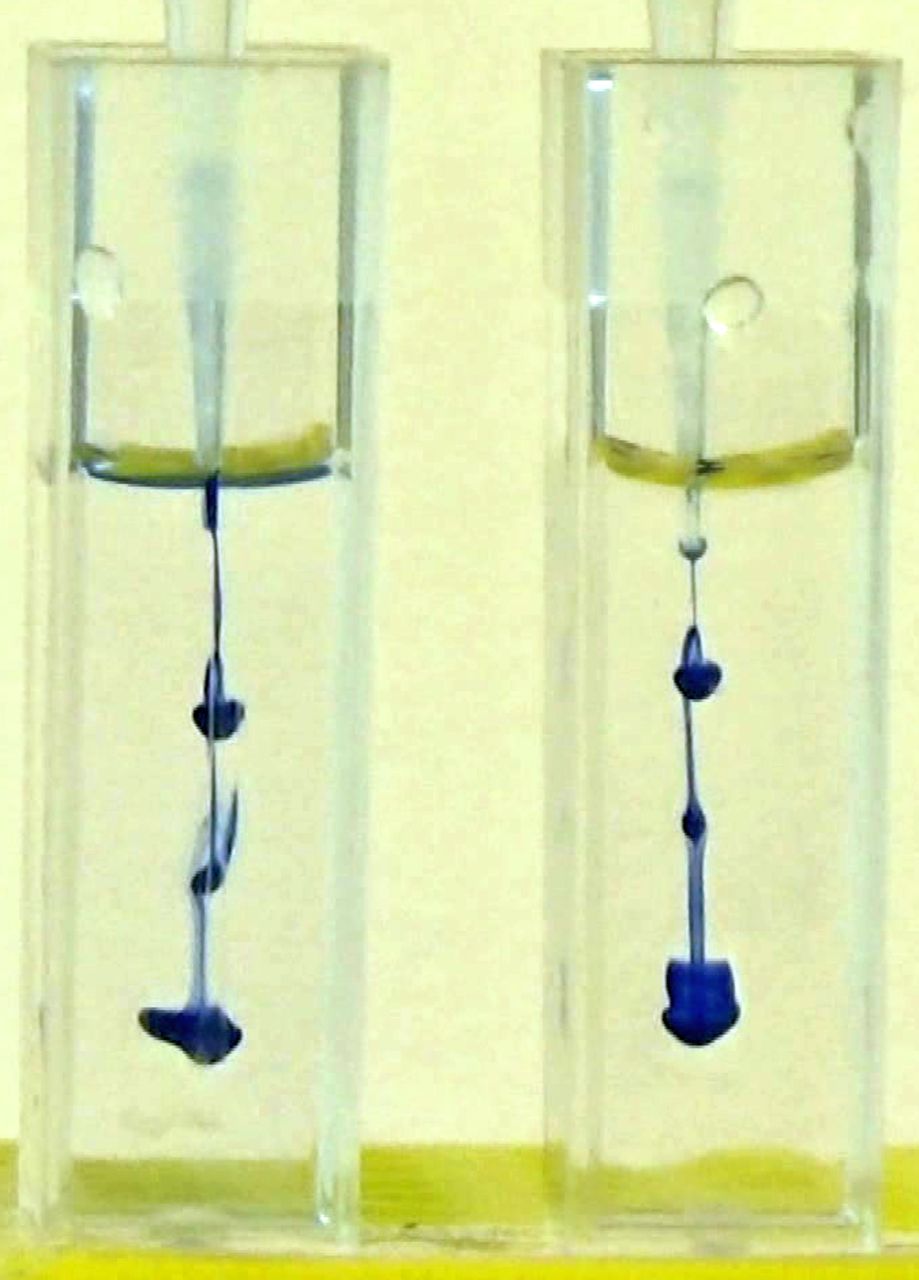
Sinking of MBD (left) and DPD (right), taken at 4.9 s after the start of the injection. DPD, double posterior dye.
MBD sinks a little faster than DPD (MBD requires 7.4 s to reach the bottom, DPD 8.8 s). Both dyes sink, however, rapidly, and no diffusion of dye away from the injected droplet is seen.
Toxicity of diglycerol
High concentrations of neutral solutes, and even more so of salts, can be detrimental to the survival of cells. On the other hand, solutes such as glycerol are known to penetrate the cell wall freely, and their contribution to osmotic stress of cells is, therefore minimal.8
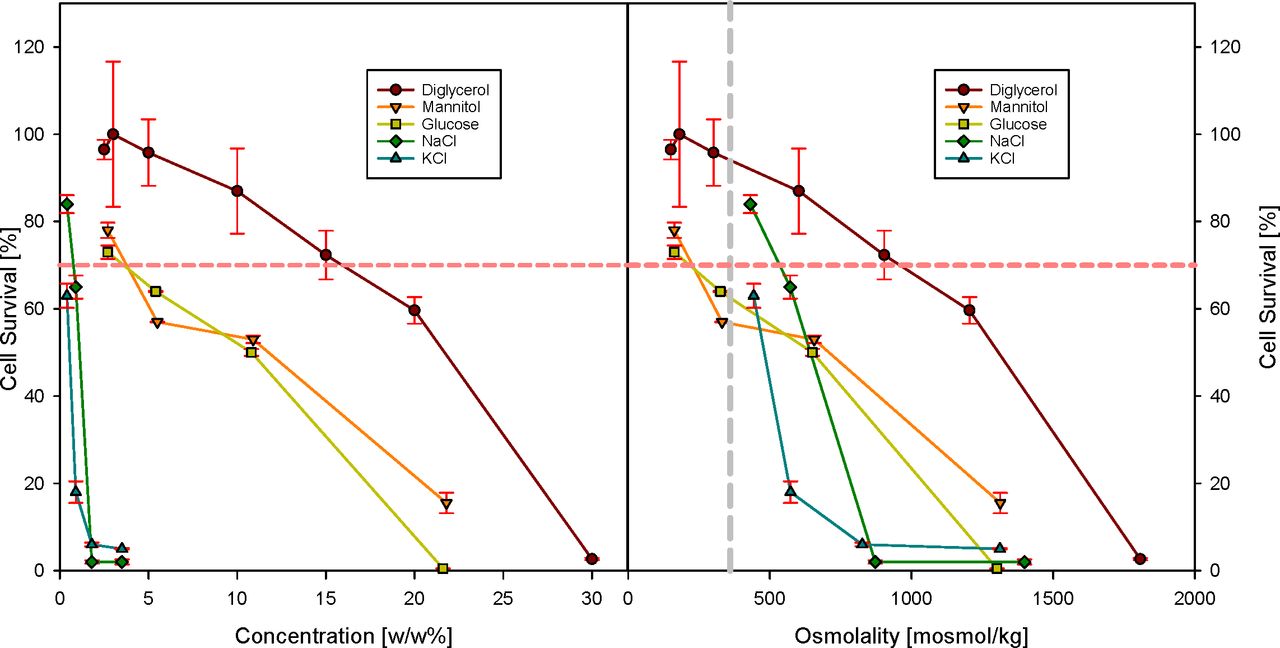
We compared the toxicity of diglycerol with that of mannitol, glucose, and the salts NaCl and KCl (figure 3). While for short exposure times of 15 min, no big difference is seen up to around 20% (w/w) of the neutral solutes and 3% (w/w) of the salts (data not shown), incubation for 24 hours in culture medium enriched with the additives showed dramatic differences. The two salts led to complete loss of cells already at concentrations of 3%, and glucose and mannitol were cell toxic (survival <70%) starting at concentrations of 5%. For diglycerol, this occurred at a three times higher concentration of 15% (w/w). Using osmolality as measure, the salts and the neutral compounds led to cell survival of less (or even much less) than 70% with concentrations corresponding to a tripling of the original osmotic pressure, whereas diglycerol was still very well tolerated by the cells.
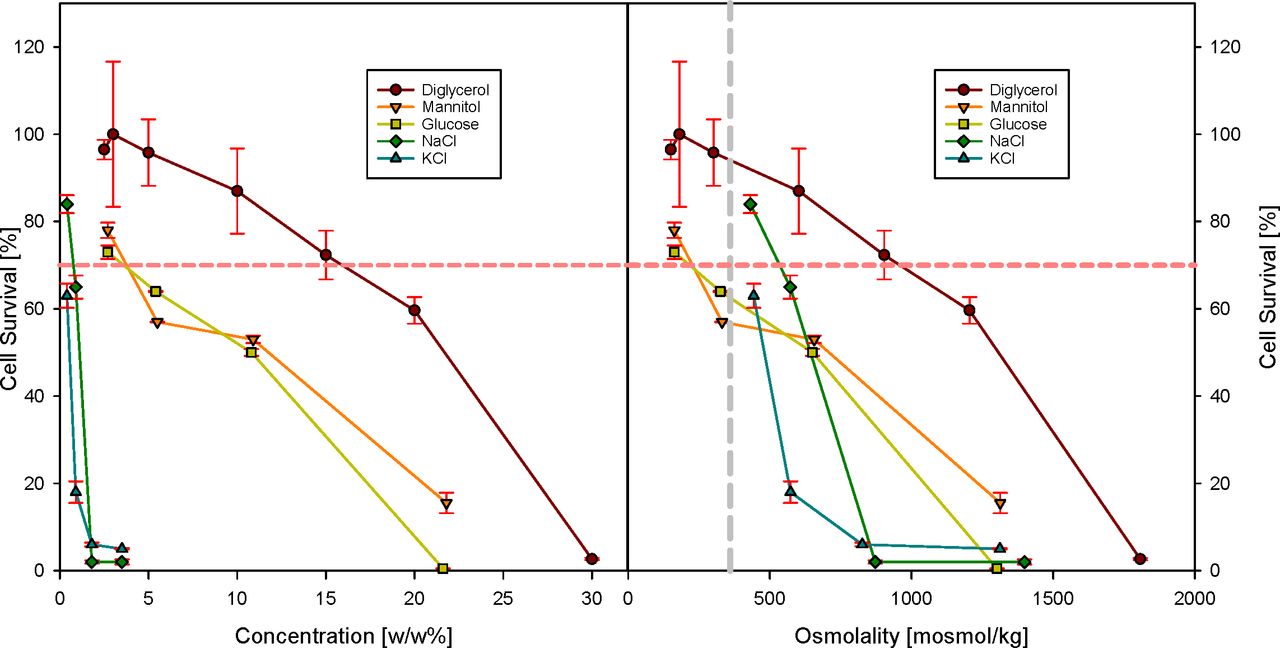
Survival of ARPE-19 cells after exposure to the indicated compounds. Exposure was in complete growth medium for 24 hours at 37°C and 5% CO2, to which the compounds had been added. The left panel shows the concentration data expressed as concentration, and the right panel as increase in osmotic pressure (osmotic pressure of the growth medium 380 mosmol/kg). The horizontal dashed line indicates the cell survival level below which a compound is considered cell-toxic.4 The vertical dashed line in the right panel indicates where the total osmotic pressure has been increased to twice the physiological value.
Transparency
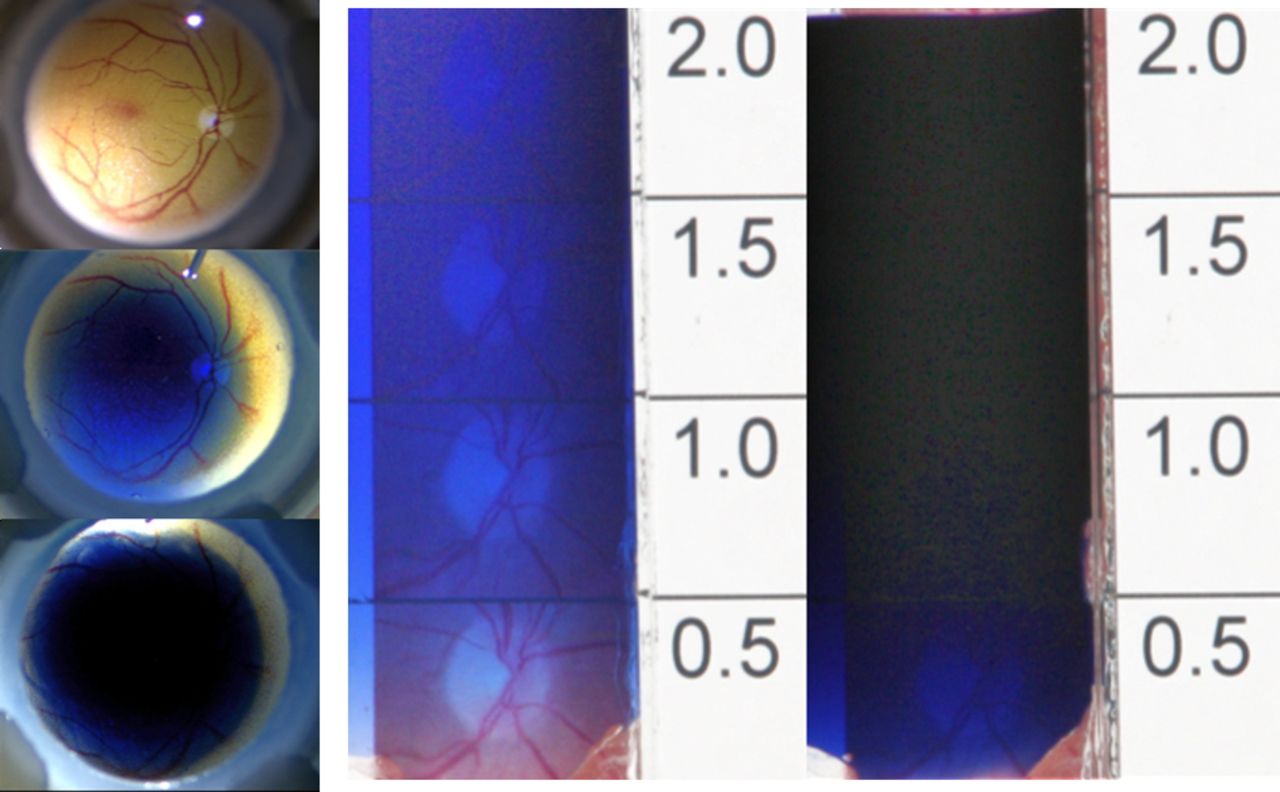
Due to the reduced concentration of TB in DPD (0.09%), transparency of the solution in the eye is much better than MBD (0.15% TB). As shown in figure 4, much of the blood vessels in the fundus is still visible with DPD, whereas MBD allows only a very small rim of blood vessels to be seen. This is also observed in a wedge cuvette. The amount of 100 µl used in the eye model is roughly what is applied in human surgery procedure. The translucent appearance of DPD allows a safe aspiration of the applied dye without the risk of touching the retina surface, which is not given for MBD due to its dark blue aspect.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Transparency of dye solutions in an eye model. Left from top to bottom: Photo of model without dye; photo of model filled with 100 µL DPD; photo of model filled with 100 µL MBD. Centre and right: Transparency of DPD (centre) and MBD (right), visualised in a wedge cuvette. The numbers give the thickness of the liquid layer (in mm) at the line above the number. The pink part in the lower right corner (where glue moved into the cuvette through capillary forces) shows the original colour of the background picture. DPD, double posterior dye; MBD, Membrane Blue Dual.
Discussion
The main results from this study are the introduction of diglycerol as osmotically benign agent to enhance density, and the introduction of a new dye as alternative to the commonly used BBG. DPD combines the translucent properties of ICG with the high affinity of TB and BBG to the target tissues ILM and ERM in marketed products.
The use of diglycerol, replacing PEG polymers, allows to decrease the concentration of TB in the staining solutions from 0.15% to 0.09% with maintaining the same staining level in the collagen membrane model used for evaluation. The considerable decrease adds greatly to the safety during surgery, as the surgeon can still see the fundus through the edge of the staining solutions, minimising the risk of touching the retina while removing the dye solution. In comparison to other low-molecular weight additives, diglycerol does not add much to the osmotic stress sensed by the ARPE-19 cells, presumably because it can move relatively freely from the solution into the cell and back, similar to glycerol.
In contrast to the PEG solutions, diglycerol solutions are less viscous, and aspiration with a flute needle is easier, without compromising the other desired properties.
The new dye DDG has similar staining properties similar to BBG and is not (photo)-toxic in the concentrations used. We tested the toxicity of DDG and of diglycerol on ARPE-19 cells, following the recommendations in ISO 10993 where permanent cell lines are preferred over primary cell lines.4
The use of porcine eyes obtained from the slaughterhouse gave non-consistent results for staining, as it was difficult to remove the vitreous completely prior to the staining. This might be attributed to the young age of the animals. We could demonstrate the presence of remaining vitreous, as it can be stained with a dye evaluated by us for use in anterior chamber surgery.9
In summary, we have been able to prepare a new formulation of dyes for vitreoretinal surgery to bridge the need between the translucent ILM-selective stains BBG and (off-label) ICG and the ERM-staining by TB, with improved properties over available dye combinations. Further studies in patients will show whether the new formulation is safe, while maintaining sufficient staining for the surgical procedure.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AM and DG designed the study and wrote the manuscript. PC established the formulation and measured sinking. JW did the toxicity and live-dead staining experiments. MA-J supervised the synthetic work. MA, EA, JJ and TW developed the synthesis of the new dye. GR optimised the synthesis. All authors approved the manuscript.
Funding This work was supported by the Meyer-Schwarting Stiftung Bremen.
Competing interests AM and DG have a patent on use of diglycerol in vitreoretinal surgery. DG has submitted a patent on DDG in vitreoretinal surgery, and a patent on solutions for staining the posterior with reduced TB concentrations.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.