Article Text

Abstract
Objective This study aimed to investigate the anatomical and functional changes in patients with central retinal artery occlusion (CRAO) (n=21) treated with 10 µg/day intravenous liposomal prostaglandin E1 (lipo-PGE1).
Methods and analysis We used best-corrected visual acuity (BCVA), central retinal thickness with spectral domain optical coherence photography, optical intensity ratio (OIR) with imageJ software and retinal vessel diameter with fundus photography as indicators. Data were analysed using Tukey’s multiple comparisons, Wilcoxon test or Spearman’s correlation analysis as appropriate.
Results BCVA was significantly improved at 1 month and 3 months after the initial visit (from 2.18±0.60 to 1.54±0.84 and 1.53±0.88, p=0.030 and p=0.027, respectively). The ratio of retinal vein diameter to optic disc diameter increased in the first month (from 0.40%±0.13% to 0.52%±0.16%, p=0.005). In addition, the OIR at the initial visit was significantly correlated with BCVA at 3 months (p=0.006, r=0.58). No severe adverse effects were observed.
Conclusion The results showed that visual acuity and retinal vein constriction improved after lipo-PGE1 therapy. In addition, the OIR in the initial phase can be an indicator of visual prognosis after treatment with PGE1 in patients with CRAO.
- retina
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Prostaglandin E1 (PGE1) is known to dilate blood vessels and inhibit platelet aggregation to increase blood flow; liposomal PGE1, which was designed to accumulate in vascular lesions, has recently been widely used at lower dosages than those of free PGE1, and has shown better outcomes for various diseases, such as peripheral arterial occlusive disease, diabetic neuropathy and leg ulcers.
WHAT THIS STUDY ADDS
Best-corrected visual acuity (BCVA) was significantly improved at 1 month and 3 months after the initial visit. The ratio of retinal vein diameter to optic disc diameter increased in the first month. In addition, the optical intensity ratio (OIR) at the initial visit was significantly correlated with BCVA at 3 months.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
OIR in the initial phase can be an indicator of visual prognosis after treatment with PGE1 in patients with central retinal artery occlusion.
Introduction
Central retinal artery occlusion (CRAO) is associated with severe vision loss and poor visual prognosis. It is typically classified into four categories: non-arteritic CRAO, non-arteritic CRAO with cilioretinal artery sparing, transient non-arteritic CRAO and arteritic CRAO.1 Non-arteritic CRAO is caused by thrombus or embolus.2 3 The anoxic intracellular oedema resulting from CRAO observed histologically appears on optical coherence tomography (OCT) as a thickening of the inner retinal layers in the acute stage of the condition, and inner retinal layers become atrophic gradually.4 CRAO is a well-known disease, and several studies have been conducted on various therapies. These include studies on anterior chamber paracentesis, digital ocular massage, intraocular pressure (IOP)-lowering drugs, antiplatelet or anticoagulant drugs, administration of a mixture of carbon dioxide and oxygen gas, and various combinations of these therapies,5–18 although none of these therapies have proved to be significantly effective for visual prognosis. The options for the management of this disorder remain controversial. Aspirin is commonly used in conservative therapy, but the risk of bleeding is observed to be consistently higher in aspirin treatment groups than that in control groups, suggesting that the use of aspirin is still a concern.19
Prostaglandin E1 (PGE1) is known to dilate blood vessels and inhibit platelet aggregation to increase blood flow.20 21 In previous reports, CRAO eyes showed better visual outcomes after PGE1 treatment (using a dosage of 80 µg/day) than that before PGE1 treatment,22 23 suggesting that PGE1 treatment is an option for treatment of CRAO. However, fatal side effects, such as cerebral haemorrhage, have been reported with high-dose PGE1 therapy.24
Liposomal PGE1 (lipo-PGE1), which was designed to accumulate in vascular lesions, has recently been widely used at lower dosages than those of free PGE1, and it has shown better outcomes for various diseases, such as peripheral arterial occlusive disease, diabetic neuropathy and leg ulcers.25 26 The dosage of lipo-PGE1 commonly used for various diseases has been reported to be 10 µg/day.26 Administration of lower dosages of lipo-PGE1 can potentially decrease the risk of adverse events; however, no previous studies have investigated the clinical course of low-dose lipo-PGE1 treatment in CRAO.
We investigated the anatomical and functional outcomes of intravenous low-dose lipo-PGE1 therapy in patients with CRAO.
Materials and methods
Patients
The patient’s database at Shinseikai Toyama Hospital was searched, and patient’s records from between October 2008 and April 2021 were reviewed. Patients included were those who met the following criteria: (1) diagnosed with non-arteritic CRAO without a cilioretinal artery using fluorescein angiography (FA) and (2) completed follow-up for more than 90 days. The exclusion criteria were (1) non-arteritic CRAO with cilioretinal artery sparing, transient non-arteritic CRAO and arteritic CRAO using FA and (2) not undergoing FA.
Ophthalmic examinations
All patients in this study underwent comprehensive examinations, including best-corrected visual acuity (BCVA) assessment, non-contact tonometry, slit-lamp biomicroscopy, fundus photography, spectral domain OCT (SD-OCT; Heidelberg Engineering GmbH, Dossenheim, Germany) and FA.
The macula was scanned using a standard 6×6 mm protocol. SD-OCT scanning and analysis of all study eyes was performed by an experienced investigator (HT).
Protocol for PGE1 therapy
All patients received an intravenous bolus of 10 µg PGE1 (Alprostadil, Taisho Pharmaceutical, Tokyo, Japan) once a day on an outpatient basis for 7 or 14 days. First, we performed a 7-day treatment for each patient. If the BCVA improved, the treatment was extended for another week, that is, for a total of 14 days. Participants did not receive any other treatment, such as ocular massage or IOP-lowering therapy.
Evaluation of the effectiveness of PGE1 treatment
The primary outcome compared BCVA at the initial visit, with BCVA after 1 month and 3 months, respectively. BCVA was measured using a Landolt decimal acuity chart and converted into the logarithm of the minimal angle of resolution (logMAR). ‘Light perception’, ‘counting fingers’, and ‘hand motions’ were calculated as logMAR values of 2.8, 2.5 and 2.3, respectively, as previously described.27
The secondary outcomes were (1) optical intensity ratio (OIR) and central retinal thickness (CRT) at the initial visit and after 1 month and 3 months, respectively; (2) retinal vessel diameter at the initial visit and 1 month; and (3) adverse events.
Measurement of CRT and OIR
CRT was measured using SD-OCT (Spectralis, Heidelberg Engineering GmbH, Dossenheim, Germany), and optical intensity was obtained using ImageJ software V.2.0.0 (National Institutes of Health, Bethesda, Maryland, USA). Regions of interest were manually selected, as in a previous report,27 by two of the authors (TS and CO). OIR was calculated as the ratio of optical intensity of the inner retinal layers, including the retinal nerve fibre, ganglion cell, inner plexiform, inner nuclear and outer plexiform layers to that of the outer plexiform and photoreceptor/retinal pigment epithelium layers, based on a previous report27 (online supplemental figure 1). The inter-rater intraclass correlation coefficient among the two graders was 85.3%. It was performed in a blind way. We considered the reproducibility to be excellent, and the following analyses were performed using data from only one examiner.
Supplemental material
Measurement of retinal vessel diameter
We followed the method of a previous report,22 which examined the changes in retinal vessel diameters during PGE1 treatment of CRAO. However, with this method, image conditions, including magnification power, have a great influence on the accuracy of retinal vessel diameter measurements; therefore, we also measured longitudinal papillary diameter and calculated the ratio of retinal artery diameter to longitudinal papillary diameter (A/D), and retinal vein diameter to longitudinal papillary diameter (V/D). Two examiners (TS and HT) performed the measurements in a blind manner. The inter-rater intraclass correlation coefficients among the two graders were 92.7% and 93.7% for A/D and V/D, respectively. We considered the reproducibility to be excellent, and the following analyses were performed using data from only one examiner.
Statistical analysis
BCVA, CRT and OIR at the initial visit and after 1 month and 3 months, respectively, were analysed using Tukey’s multiple comparisons. A/D or V/D at the initial visit and after 1 month was compared using the Wilcoxon test. Statistical significance was set at p<0.05.
Using Spearman’s correlation analysis, correlations between OIR at the initial visit or after 1 month and BCVA at the initial visit or at 3 months, as well as correlations between CRT at the initial visit or after 1 month and BCVA at the initial visit or at 3 months, were assessed. The correlation between OIR at the initial visit and the change in BCVA from the initial visit to 3 months was also assessed. The correlation coefficient (r) was calculated, with statistical significance set at p<0.05. Statistical analyses were performed using R V.4.0.2 (The R Foundation for Statistical Computing, Vienna, Austria).
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Patient characteristics
The characteristics of the included patients at the initial visit at 1 month and at 3 months are shown in table 1. Two patients without FA, two patients with cilioretinal artery sparing and one patient with transient CRAO were excluded. The patients included 13 men (13 eyes) and 8 women (eight eyes) (mean age, 73.3±11.1 years; range, 45–91 years): 3 had diabetic retinopathy (non-proliferative diabetic retinopathy without macular oedema), 2 had glaucoma without central visual field loss, 1 was post-treatment for peripheral retinal tear without retinal detachment and 1 had mild epiretinal membrane of cellophane maculopathy. These comorbidities were not considered to significantly confound the study results. Seventeen patients received lipo-PGE1 for 14 days and the other four patients for 7 days. The mean time from onset to PGE1 administration was 54.7 hours; range, 2–240 hours. There were no adverse effects including cerebral haemorrhage recognised in the current study.
Summary of results for the current study
Changes in BCVA, CRT, OIR and vessel diameter
The results are shown in table 1. The mean logMAR BCVA values were 2.18±0.60 (range, 0.82–2.80) at the first visit, 1.54±0.84 (range, 0–2.5) after 1 month and 1.53±0.88 (range, 0–2.8) after 3 months (online supplemental figure 2). The BCVA values at 1 month and 3 months were significantly better than that at the first visit (p=0.030 and p=0.027, respectively). However, there was no significant difference between months 1 and 3 (p=0.999).
Supplemental material
The mean CRT was 221±66 µm (range, 130–444 µm) at the first visit, 184±30 µm (range, 136–241 µm) after 1 month and 169±21 µm (range, 123–207 µm) at 3 months. The CRT at 3 months was significantly thinner than that at the first visit and at 1 month (p=0.033 and p=0.0043, respectively).
The mean OIRs were 1.09±0.22 (range, 0.68–1.54) at the first visit, 0.84±0.17 (range, 0.61–1.27) after 1 month and 0.68±0.11 (range, 0.61–0.91) at 3 months. The OIRs at 1 month and 3 months were significantly lower than that at the first visit (p<0.001 and p<0.001, respectively). The OIR at 3 months was significantly lower than that at 1 month (p=0.040).
The mean A/D was 0.034±0.0095 (range, 0.021–0.054) at the first visit and 0.035±0.010 (range, 0.020–0.051) after 1 month. There was no significant difference between values for the first visit and those observed after 1 month (p=1.000).
The mean V/D was 0.040±0.013 (range, 0.012–0.068) at the first visit and 0.052±0.016 (range, 0.025–0.076) after 1 month. The V/D at 1 month was significantly larger than that at the first visit (p=0.005). A representative case is shown in online supplemental figure 3).
Supplemental material
Correlation between BCVA and CRT, and between BCVA and OIR
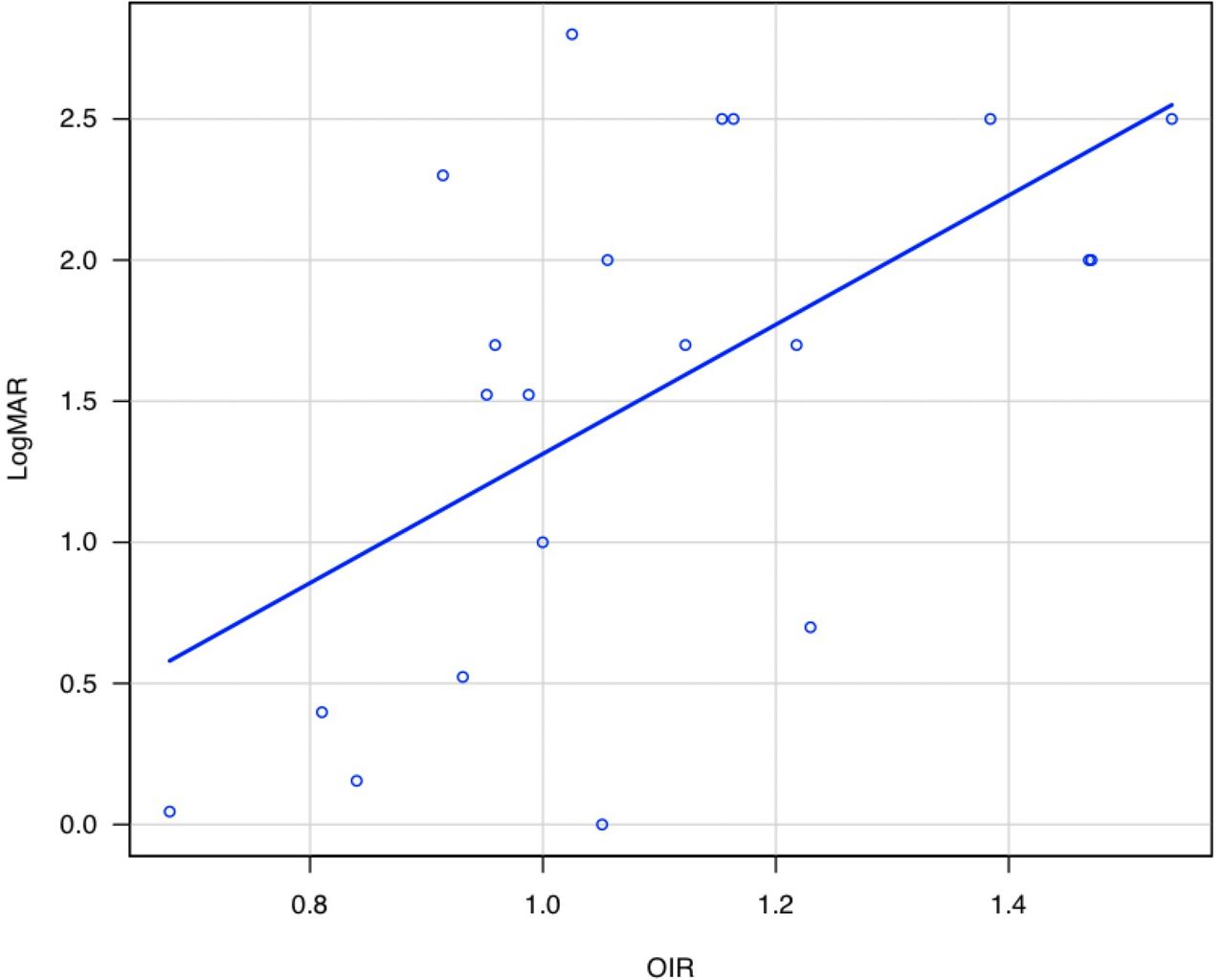
The BCVA at 3 months was significantly correlated with OIR at the initial visit (p=0.006, r=0.58; table 2, figure 1). Meanwhile, it was not significantly correlated with OIR at 1 month (p=0.104), CRT at the initial visit (p=0.500) and CRT at 1 month (p=0.625). The BCVA at the initial visit was not significantly correlated with OIR at the initial visit (p=0.187) and at 1 month (p=0.260), or CRT at the initial visit (p=0.496) and at 1 month (p=0.284).

Correlation between best-corrected visual acuity at 3 months and OIR at the first visit. P=0.006, r=0.58. LogMAR, logarithm of the minimal angle of resolution; OIR, optical intensity ratio.
Correlations between BCVA at the first visit and OIR at the first visit or 1 month or CRT at the first visit or 1 month, and correlations between BCVA at 3 months and OIR at the first visit or at 1 month or CRT at the first visit or 1 month
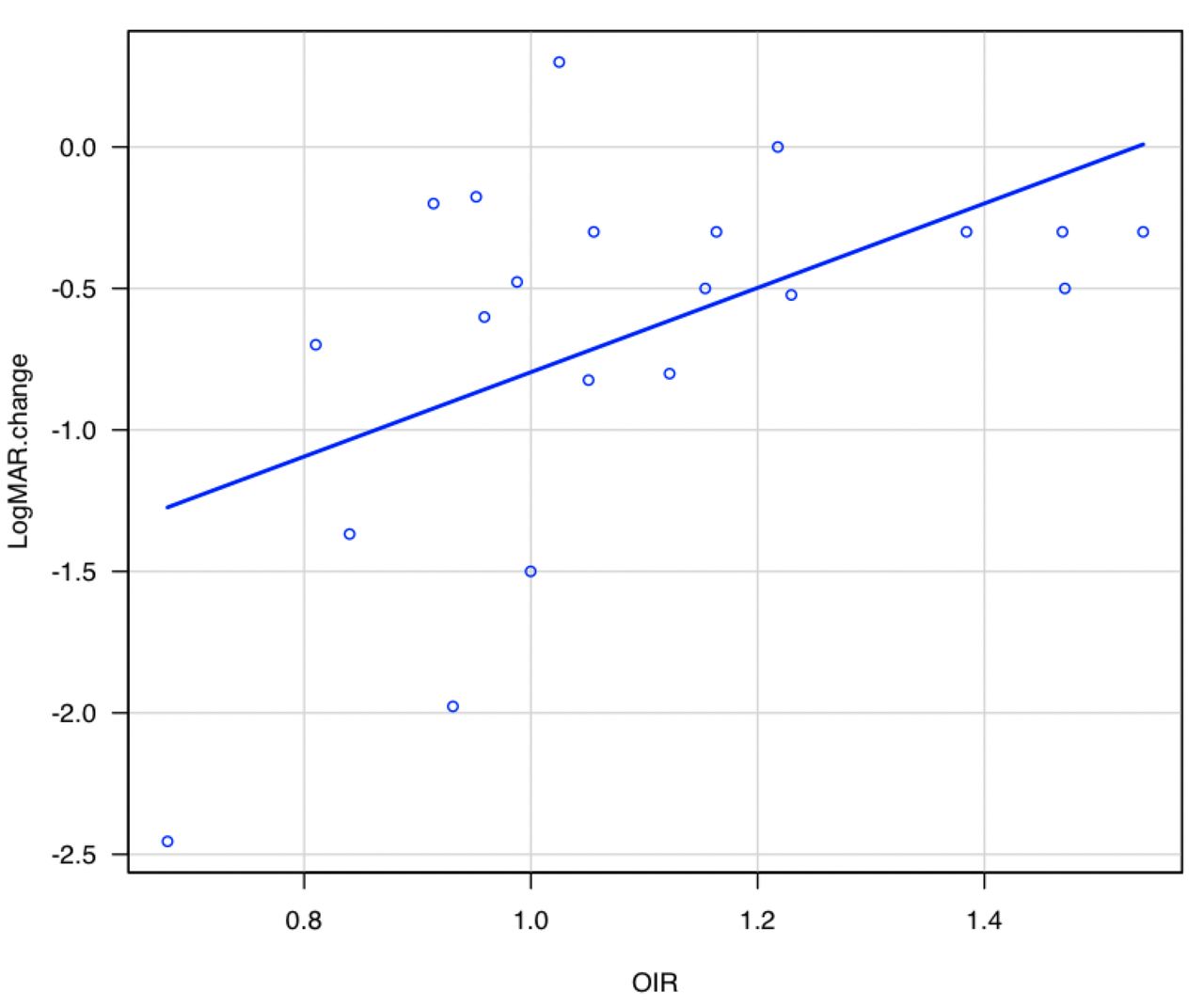
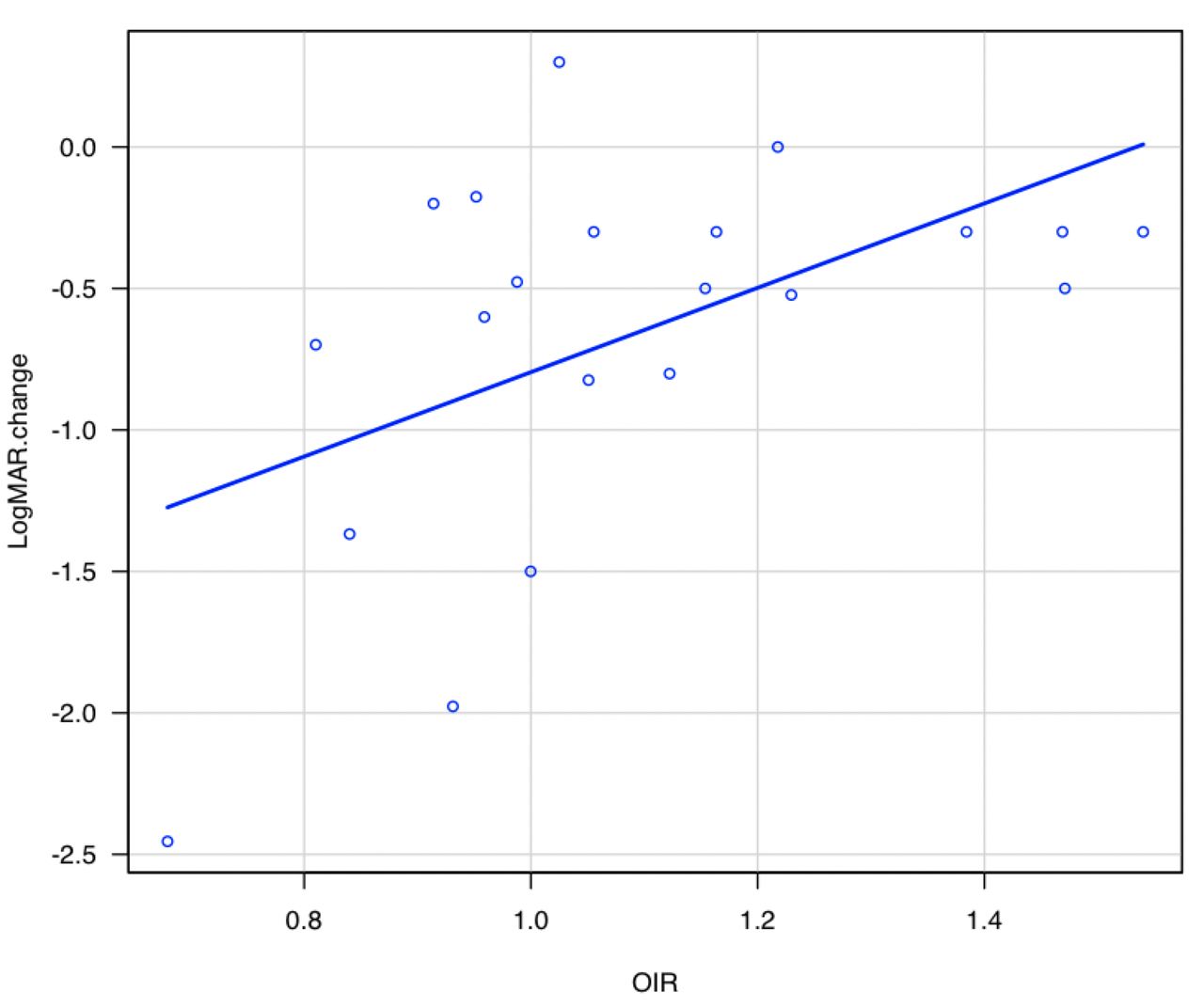
Change in BCVA from the initial visit to 3 months was significantly correlated with OIR at the initial visit (p=0.017, r=0.52; figure 2).
{kind=link}
{kind=link}
The correlation between OIR at the first visit and the change in best-corrected visual acuity from the initial visit to 3 months. P=0.017, r=0.52. LogMAR change and best-corrected visual acuity at 3 months—the one at the first visit. LogMAR, logarithm of the minimal angle of resolution; OIR, optical intensity ratio.
Discussion
In the present study, we assessed the anatomic and functional outcomes of patients with CRAO that were treated with low-dose lipo-PGE1 therapy. The results showed that visual acuity and retinal vein constriction improved after the treatment. In addition, the OIR in the initial phase can be an indicator of visual prognosis after treatment with PGE1 in patients with CRAO.
There have been only two reports of intravenous PGE1 administration being used in the treatment of CRAO.22 23 Takai et al22 reported in 2013 that 10 patients were administered 80 µg/day free PGE1 (intravenous drip infusion 80 µg/day in two doses for 5 days+ oral 30 µg/day for 1 month) and followed up for approximately 1 month. Additionally, Malbin et al23 investigated the BCVA of six eyes that were administered 80 µg/day free PGE1 (intravenous drip infusion 80 µg/day in two doses for 3–5 days) and followed up for approximately 1 month. In contrast, lipo-PGE1 is commonly used at doses of 10 µg/day for various diseases.26 There have been reports of fatal side effects such as cerebral haemorrhage with high-dose lipo-PEG1 therapy (60 to 180 µg/day),24 although 10 µg/day lipo-PGE1 therapy has not been considered to cause fatal side effects.26 However, to the best of our knowledge, there have been no published reports that investigated the results of 10 µg/day lipo-PGE1 treatment of CRAO.
Three other studies22 23 28 gave outcomes relevant for our study. A summary is shown in table 3. It includes two reports22 23 about PGE1 therapy for CRAO and one report28 on a large cohort study without any treatment. In the previous natural history report, the BCVA of 171 patients did not significantly improve. Meanwhile, the two studies with standard-dose free PGE1 treatment showed significant improvement in BCVA after 1 month.22 23 In the current study, the BCVA improvement was comparable with that observed in the standard-dose free PGE1 treatment, although the mean age was older and time to treatment was longer than those in the free PGE1 studies. The results of the current study suggest that BCVA changes in low-dose lipo-PGE1 might be similar to those seen with standard-dose free PGE1 treatment.
Summary of the current study and previous studies on PGE1 therapy, as well as natural history studies on CRAO
In a previous study,27 OIR at the initial visit was significantly correlated with BCVA after more than 3 months. Our study supports this finding. OIR is thought to reflect the degree of retinal damage in the inner retinal layer and is therefore related to visual prognosis. However, the detailed pathological mechanism of increased optical intensity remains unknown as the study describes. As observed in the previous report,27 OIR can be a helpful biomarker associated with visual prognosis in CRAO, even with PEG1 treatment. However, we could not prove a correlation between OIR at 1 month and BCVA at 3 months. This suggests that OIR is a good indicator of visual prognosis within the first month from onset.
Considering figure 2, in patients with high OIR, the change in BCVA after Lipo-PGE1 treatment is relatively poor compared with that in patients with low OIR. The response to lipo-PGE1 in patients with high OIR, indicating severe retinal damage, should be further investigated.
In the current study, only retinal vein diameter was significantly increased with lipo-PGE1 treatment. PGE1 is reported to improve endothelial function,29 dilate vessels20 and inhibit platelet aggregation.21
Atherosclerosis of blood vessels occurs mainly in arteries.30 In addition, in atherosclerosis patients, normal vasodilatation is impaired due to endothelial dysfunction.31 Therefore, we should consider the possibility that arteries may be more difficult to dilate than veins. Care should be taken that vessel diameter could not assess the degree of improvement in blood flow after the treatment directly. Detailed assessment using angiography might help to elucidate the point. Moreover, how the venous dilation is involved in the visual improvement or OIR changes is still unclear, and it requires to be elucidated in the future analysis.
This study had several limitations. A major limitation is that the current study is a retrospective, observational, small case series study. The design is not sufficient to verify the effectiveness and of the lipo-PGE1 treatment compared especially with observation. Prospective, large-scale studies are necessary to assess the efficacy or to investigate the associating factors. Because the primary purpose of our study was to review the clinical course of lipo-PGE1 therapy, which has not been previously reported, the time from onset to treatment has a relatively wide range. Furthermore, the retinal diseases other than CRAO in a part of the patients were not thought to have direct or major impacts on visual acuity, although we cannot deny indirect effects on visual acuity. In the future, we will perform condition-matched statistical comparisons between lipo-PGE1 treatment and standard-dose PGE1 treatment, natural history or other kinds of treatment.
We investigated the anatomic and functional outcomes of patients with CRAO that underwent 10 µg/day lipo-PGE1 therapy. BCVA was significantly improved after 3 months, similar to what was observed in previous reports with 80 µg/day free PGE1 treatment. OIR at the first visit only was significantly correlated with BCVA at 3 months. Retinal vein diameter was significantly larger at 1 month than at the initial visit.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Shinseikai Toyama Hospital (approval number 210524-1). Our study was retrospective, and we used an opt out consent process; informed consent was waived by the Institutional Review Board of Shinseikai Toyama Hospital and participants who did not grant authorisation to use their medical records for the research were excluded from the study.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TS was involved in the study design, data collection, analysis of the results and manuscript drafting. RO participated in the study design, data collection and manuscript review and editing, and is an author responsible for the overall content as the guarantor. TI participated in the study design and data collection. YU, KA, HT, KK, CO, YH, MA and NT participated in data collection, manuscript review and editing. All authors have read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.