Article Text

Abstract
Objectives This study aims to investigate the expression of Ki67 in formalin-fixed paraffin-embedded tissue blocks from patients with a diagnosis of retinoblastoma tumour (RbT) as well as determining its association with histopathological high-risk factors (HHRFs).
Methods and analysis Retrospectively, a total of 194 eyeball specimens from 163 children with RbT were reviewed at Muhimbili National Hospital between 2009 and 2013. Immunohistochemical expression of Ki67 using MIB-1 antibody (Abcam, batch ab93680, Cambridge, UK) was determined and correlated with the conventional HHRFs. The predictors of Ki67 expression were determined using binary logistic regression model in multivariate analysis. A two-tailed p<0.05 was considered statistically significant.
Results Majority (67.5%) of the patients had leukocoria and extraocular disease was found in 20.9% of all the patients. High expression of Ki67 was present in 63.8% of the 80 eyeballs that were tested. Massive choroidal invasion (adjusted OR (AOR)=9.32, 95% CI=2.82 to 10.89), positive retrolaminar optic nerve invasion (AOR=3.01, 95% CI=4.43 to 9.11), positive surgical margin (AOR=7.10, 95% CI=1.63 to 11.40) and pT4 (AOR=7.49, 95% CI=0.12 to 0.89) were the potential HHRFs that were associated with Ki67 overexpression.
Conclusion Overexpression of Ki67 may be of prognostic value for patients with RbT as it has been shown in the present study that high expression was common in tumours with massive choroidal invasion, positive retrolaminar optic nerve invasion, positive surgical margin and advanced tumour stage, which are the conventional HHRFs associated with prognosis of RbT.
- pathology
- neoplasia
- medical education
- eye (globe)
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
The prognostic role of both clinical and pathological factors in patients with retinoblastoma tumour has been extensive, however, the prognostic role of Ki67 among patients with retinoblastoma tumour has rarely been investigated.
Although there are few studies which have reported on the association of Ki67 expression among patients with retinoblastoma tumours, there no studies that focus on association of high-risk histopathological factors with Ki67 expression.
What this study adds
This study provides insights on the association of Ki67 expression with high-risk histopathological factors such as pathological stage, optic nerve invasion and massive choroid invasion, which is of utmost importance for the management of patients with retinoblastoma tumour.
This study also gives emphasis on the need of having a large study in the future, which should analyse the correlation of Ki67 expression with long-term survival of the patients with retinoblastoma tumour in order to provide data with high level of evidence.
How this study might affect research, practice or policy
The findings obtained from this study may help in the future for providing additional prognostic biomarkers in helping to improve the prognosis of patients with retinoblastoma tumours.
Introduction
Retinoblastoma tumour (RbT) is the most common primary ocular malignant tumour affecting the paediatric population.1 It is caused by mutation of the retinoblastoma gene (Rb1), which is located on the chromosome 13q14.2 The mutations are 40% germline in nature and the other 60% of the mutations are sporadic.3 The annual incidence of RbT for children with age ranging from 0 to 4 years in high-income countries (HICs) is 10.0–11.8 per 1 000 000 person-years.4 The incidence reported in the literature for Africa particularly in the sub-Saharan African region is 9000 new cases per year, which corresponds to the incidence of 1 in 15 000 births.5 In low- and middle-income countries (LMICs), children who are diagnosed with RbT usually are older than those in HICs and also, they tend to have poor prognosis because they are diagnosed at late stage.6
Studies have outlined different histopathological features as high-risk factors (HHRFs) and are associated with tumour progression, metastasis and overall poor prognosis.7 A number of HHRFs has been found to be associated with higher risk of metastasis and poor overall survival including massive choroidal invasion, extrascleral extension and optic nerve involvement.8 Thaung and Karaa also reported tumour extension to the anterior chamber, iris, trabecular meshwork, Schlemm’s canal, ciliary body, choroid (above a certain threshhold), sclera, extraocular structures, retrolaminar optic nerve (including the cut end) as the HHRFs in their series.9 In one study it was reported that, HHRFs, for example, massive choroidal invasion and positive retrolaminar invasion of the optic nerve were associated with recurrence, metastasis and poor overall survival.10
Determination of the HHFRs in paediatric patients with RbTs is of utmost importance in assessing the prognosis of the patients as well as establishing the proper type of treatment for better clinical outcomes, although enucleation remains to be the main type of management for paediatric patients who are diagnosed with RbTs. Additionally, for those with advanced RbTs treatment of the patients usually must involve adjuvant chemotherapy.11 12 Complementing with biomarkers has shown to be of benefit in the determination of prognosis of the paediatric patients with RbT. Studies have shown that increased expression of cell proliferation biomarkers such as Ki67 is associated with advanced tumour stage and poor clinical outcomes.13–15 Other tumour markers such as p53 have been found to correlate significantly with the HHRFs including massive choroidal invasion and positive surgical margin of the optic nerve.16
Despite the poor clinical outcomes of patients with RbT in Tanzania, there are not yet established data in addressing the HHRFs in the paediatric population with RbTs. Also, this study is of its kind in analysing the HHRFs and their association with Ki67 in Tanzania.
Materials and methods
Study design and patients
This was a cross-sectional analytical retrospective laboratory-based study. The study was conducted at the Central Pathology Laboratory of the Muhimbili National Hospital in Dar es Salaam, Tanzania. The study included review of 194 eyeball specimens from 163 children who were diagnosed with RbT between January 2009 and December 2013. Patients’ files and laboratory investigation request forms were used to extract the required clinical data and histological results. Only cases with histologically confirmed diagnosis of RbT were enrolled in the present study. All cases with missing formalin-fixed paraffin-embedded (FFPE) tissue blocks and those with insufficient tissue as a result of being spoiled by insects were excluded from the study.
Sampling method
Convenience sampling method was applied to enrol all available FFPE tissue blocks due to limited RbT provided that they had met the inclusion criteria. Seventeen cases were excluded from the study (10 cases due to FFPE tissue blocks being spoiled by insects and 7 cases due to missing previous histological report).
H&E staining
After retrieving the FFPE tissue blocks, the tissue were sectioned and stained with H&E for re-evaluation of the previous histological diagnosis. Histological re-evaluation of the eyeball specimens was done by an independent and experienced pathologist (EAMV), who was blinded of the patients’ clinical details.
Immunohistochemical staining of MIB-1 antibody
The eyeball specimens for immunohistochemical (IHC) procedure were sectioned at the thickness of 4 μm by using a micrometre. The sections were de-waxed by placing them on a hot plate at a temperature of 60°C for 30 min. This was followed by hydration by dipping the tissue sections in decreasing concentration of ethanol (100%, 95%, 80% and 70%). Two drops of 3% hydrogen peroxide solution were added to each section for 15 min to block endogenous peroxidase for inhibiting background staining. Then the slides were put into running tap water for rinsing purpose. A 100X EDTA citrate buffer, pH 8.0 heat antigen retrieval solution was used. The antigen retrieval solution was heated in a pressure cooker until it started boiling followed by placing the slides in the retrieval solution and closing the lid of the pressure cooker from which the slides were removed 2 min after full pressure. Then the slides were placed in tap water to prevent drying.
The slides were washed using phosphate-buffered saline solution (PBS) for 3 min. PBS was then drained from the slides. A ring was made around the section placed on a glass slide using a hydrophobic Pap pen so as to limit spreading of the primary antibody solution. Then the primary antibody MIB-1 (Abcam, ab93680 model, Cambridge, UK) was applied and allowed to react with the antigen by incubating for 60 min at room temperature. The slides were then washed with PBS for 5 min and then two to three drops of horse radish peroxidase was added to each section for 30 min. The slides were again washed with PBS for 5 min. PBS was drained from the sections, and then one drop of chromogen diaminobenzidine was added to the sections for 5 min as the detection system. The sections were washed with tap water for 1 min, counterstained in haematoxylin for 10 s, differentiated by two dips into 1% acid alcohol. The sections were blued in warm water for 2 min, dehydrated through 70%, 95% and 100% ethanol and then cleared in two changes of xylene for 10 min. Positive controls for MIB-1 were known cases of diffuse large B cell lymphoma. Negative controls for the immunostain were achieved by omitting the primary antibody.
The areas of highest proliferative activity (hot spots) were identified by scanning the tumour sections at low magnification of ×40. The method of determining the positive tumour cells in this study was adopted from the previous study which was done by Kouzegaran et al,17 in which approximately 1000 tumour cells from 20 systematically randomised fields were counted, and the proportion of positive tumour cells was determined. The percentage scoring of immunoreactive tumour cells was as follows: 0 for <1% positive tumour cells; 1 for 1%–10% positive tumour cells; 2 for 11%–50% positive tumour cells; 3 for 50%–75% positive tumour cells; 4 for >75% positive tumour cells. Then intensity was evaluated as follows: negative staining (0), weak staining (1+), moderate staining (2+) and strong staining (3+). The scores of intensity and percentage were added to obtain the final score which ranged from 0 to 7. The results of immunostaining were divided into two groups; 0–2 was considered negative and 3–7 was considered positive. Reporting of the IHC tissue slides was performed by an experienced pathologist who was blinded of both clinical and histopathological data.
Quality assurance
To ensure validity and reliability of the collected data as well as the findings of the study, stringent measures were adhered to all steps of data extraction including use of negative and positive controls and blinding during histological re-evaluation of the tissue sections.
Statistical analysis
Data were analysed by using SPSS V.23.0. The coded data were cross-checked for possible error and any missing data after running frequency tables and crosstabs. Categorical and continuous variables were summarised in proportions and mean±SD, respectively. Inferential statistics were used in determining the predictors of Ki67 immunohistochemical expression by using binary logistic regression. Variables that were statistically significant as well as those which had p≤0.2 in univariate analysis were then fitted in the multivariate analysis after adjusting for each confounding factor. A two-tailed p<0.05 was considered statistically significant.
Patient and public involvement statement
This work did not include direct interaction with patients or the public in designing and conceptualisation of this work.
Results
Selection process of the study subjects
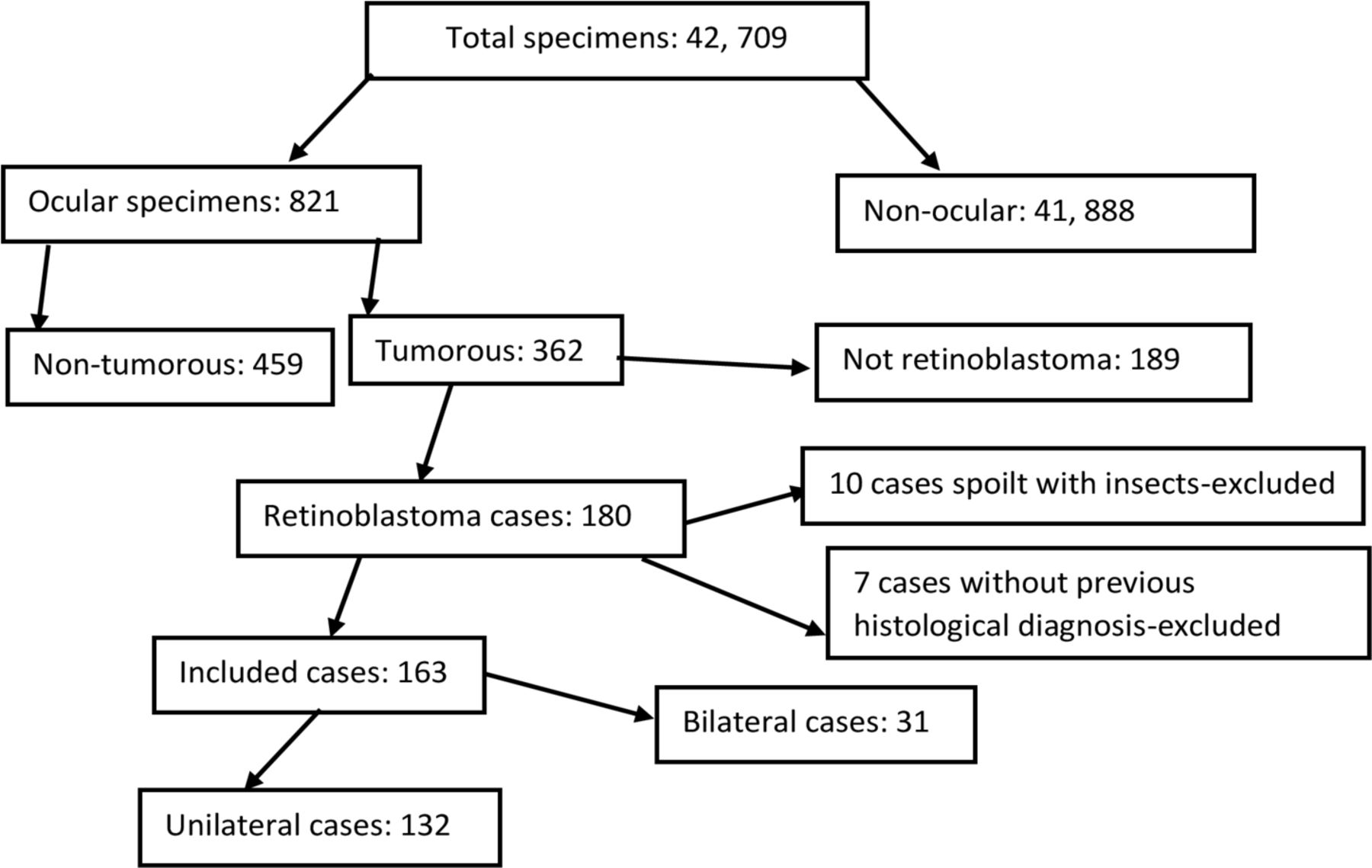
The process of selection of the study cases is presented in figure 1. For a period of 5 years (2009–2013), there were 173 cases of RbT that were diagnosed among all ocular tumours (OTs). Of the OTs that were retrievable, 17 cases were excluded due to either being spoilt by insects while in the archive room or missing previous histological diagnosis. Therefore, a total of 163 cases were retained for review in the present study.

{kind=link}
Schematic presentation of the process of the study subjects (n=163).
Sociodemographic and clinical characteristics of the patients
This study included a total of 163 patients, 80.9% (132/163) patients had unilateral disease and the remaining 19% (31/163) patients had bilateral diseases. The total number of eyeball specimens that were examined from the 163 patients was 194. The vast majority of the patients 65% (106/163) in the present study were aged 2 years and above and the mean age of the patients was 4.8±2.42 years. Males were slightly more than females and they consisted of 57.7% (94/163). The lag period of 3 months and above in terms of seeking medical attention among the patients was observed in 41.1% (67/163) of all the cases with an average of 2.1±1.94 months.
Table 1 presents the clinical characteristics of the patients. The varsity majority 67.5% (110/163) had leukocoria followed by proptosis, which consisted of 22.7% (37/163). Also, 20.9% (57/163) patients had extraocular extension (EOE). Majority (49/57) of those with EOE had optic nerve invasion. Additionally, 6.7% (11/163) of the patients had metastasis to distant organs; central nervous system—10 cases and bone marrow—1 case.
Sociodemographic and clinical characteristics of the patients (n=163)
Treatment given to the patients based on the local treatment guidelines
Table 2 presents the treatment modalities as per eyeball which were given to the patients in the study based on the International Classification of Retinoblastoma (ICRB). All eyeballs with EOE for both bilateral 15.9% (31/194) and unilateral 21.6% (42/194) cases were exenterated (upfront enucleation), which involved removal of the eyeball, optic nerve (at least 2 cm) and clearing of the socket. There were as more eyeballs with a history of salvage attempt for bilateral disease 50% (31/62) than unilateral disease 31.8% (42/132). Chemoreduction involved a combination of carboplatin, vincristine and etoposide, which were given in six cycles at the interval of 3 weeks. Chemoreduction was given to shrink the tumour for patients with ICRB group B–D and some patients in whom the affected eyeballs were in ICRB class E. None of the cases with ICRB group A were included in the present study because they are not enucleated either upfront or after chemoreduction. Eyeballs found to have class A, usually were managed by focal therapy by either cryotherapy or thermotherapy alone for smaller tumours (<3 mm in diameter and height) located in visually non-crucial area. Cryotherapy was usually administered 3–6 hours prior to chemotherapy if systemic treatment was indicated.
Treatment modalities as per eyeball based on the International Classification of Retinoblastoma (ICRB) (n=194)
Not all eyeballs had advanced disease for patients with bilateral RbT, as summarised in table 2. In some eyeballs 4.1% (8/194), there was an attempt to salvage the affected eyeballs for vision preservation, and nevertheless, after assessment of improvement they were finally enucleated.
Histopathological high-risk factors evaluated from the eyeball specimens
Of all the eyeball specimens that we examined in the present study, massive choroidal invasion was present in 18.6% (36/194) and focal involvement of the choroid layer was found in 7.2% (14/194). Anterior chamber involvement by the tumour cells was observed in 4.6% (9/194) and 20.1% (39/194) of the eyeball specimens had scleral extension of the disease. Concerning spreading of the cancer cells to the optic nerve among the eyeball specimens evaluated, we found that 25.3% (49/194) of the eyeball specimens had retrolaminar optic nerve extension (online supplemental figure 1A) and involvement by the tumour for the surgical margin of the optic nerve (online supplemental figure 1B) was found in 4.6% (9/163). Also, 20.6% (40/194) showed advanced disease (29 for pT3 and 11 for pT4). Other HHRFs are shown in table 3.
Supplemental material
Histopathological high-risk features in the eyeball specimens included in the study (n=194)
Clinical characteristics of patients with eyeballs stained with MIB-1
Ki67 immunostaining was performed in 80 eyeball specimens and not for all 194 eyeball specimens due to lack of funds to purchase sufficient antibody (MIB-1). Table 4 shows the clinical characteristics of the 65 patients of whom the 80 eyeball specimens were obtained and stained with MIB-1. Of the 65 patients, 23.1% (15/65) and 76.9% (50/65) patients had bilateral and unilateral RbT, respectively. The mean age of the patients whose eyeball specimens were subjected to Ki67 immunostaining was 4.5±1.96 years.
Clinical features for patients with eyeball specimens stained with MIB-1 (n=65)
Expression of Ki67 as detected by MIB-1 and its association with histopathological high-risk factors
The Ki67 labelling index (LI) was ranging from 3.2% to 70.8%. There was variation in expression of Ki67 in poorly differentiated cases (online supplemental figure 2A,B). The mean expression of Ki67 was 38±17.6%. Expression of Ki67 was present in 66.3% (53/80). Almost all the HHRFs had an increased chance for having high expression of Ki67 in the present study; however, massive choroidal invasion, retrolaminar optic nerve invasion positive surgical margin of the optic nerve and advanced tumour stage were the HHRFs that were significantly associated with high expression of Ki67.
Supplemental material
The chance for eyeball specimens with massive choroidal invasion to have high expression of Ki67 was 9.32 times more than that without choroidal invasion (adjusted OR (AOR)=9.32, 95% CI=2.82 to 10.89). This showed a noticeable difference for eyeball specimens with focal choroidal invasion which even though had a 1.22-fold increased chance for high expression of Ki67 compared with the eyeball specimens without choroidal invasion, but the difference was not significant (AOR=1.22, 95% CI=0.49 to 2.82).
The odds of high expression of Ki67 in eyeball specimens with positive retrolaminar part of the optic nerve was 3 times more than that of the eyeball specimens that had no invasion of the retrolaminar part of the optic nerve and the difference was significant (AOR=3.01, 95% CI=4.43 to 9.11). Also, there was a 7.10-fold increased chance for the odds of having high expression of Ki67 for eyeball specimens with positive surgical margin of the optic nerve as compared with eyeball specimens (AOR=7.10, 95% CI=1.63 to 11.40). Interestingly, there was a linear increase of the percentage of high expression of Ki67 as per pT stage (pT1–pT2=18.5%, pT3=34.5% and pT4=75%). Eyeball specimens with pT4 had a 7.49-fold increased chance of having high expression of Ki67 compared with cases which were of pT1–pT2 (AOR=7.49, 95% CI=0.12 to 0.89). Despite the fact that other variables showed increased odds of high expression of Ki67, they showed no statistical difference between the compared groups of each variable (online supplemental table 1).
Supplemental material
Discussion
RbT being the most common intraocular malignancy in the paediatric population, it carries the highest mortality rate in LMICs unlike in HICs. This has been mainly associated with remarkable delay in diagnosis for the LMICs. In this series, the main HHRFs in a cohort of paediatric patients with RbT were described along with association with immunoreactivity of Ki67.
The key and promising finding which has further strengthened the evidence that Ki67 may be used as a prognostic biomarker is that, in this study Ki67 LI was associated with increased tumour aggressiveness as indicated by extent of invasion into various structures of the eyeballs. This observation is in agreement with findings in previously reported studies elsewhere.17 18 The Ki67 LI of 66.3% in the present study was higher than 53.33% which was reported in the study by Kouzegaran et al,17 but lower than 73%, 90% and 91% which were reported in Mexico19 and other two studies in China, respectively.20 The discrepancies in the incidence of Ki67 LI observed across studies may be contributed by a number of factors including extensive necrosis in the FFPE tissue blocks,21 challenges with other pre-analytical phase procedures like delayed fixation and prolonged fixation which may be associated with antigen masking.22 Furthermore, it has also shown that neoadjuvant therapy affects the expression of immunohistochemical biomarkers. For example, in a study which was done by Wu et al, it was shown that the expression of oestrogen receptor (ER) and Ki67 before chemotherapy and after chemotherapy decreased from 65.3% to 42.6% for ER and from 51% to 43.4% for Ki67.23
Ki67 expression in the present study was found to increase with invasion of the disease. This has also been reported in other studies. For example, Kim et al showed that Ki67 expression was associated with advanced tumour stage.18 This is also similar to the finding that was reported by Kouzegaran et al.17 Ki67 being a nuclear cell proliferation biomarker, is usually associated with tumour invasiveness and metastasis. It indicates how fast the tumour cells tend to quickly divide when the tumour is at advanced stage. Furthermore, Orjuela et al in Mexico also reported that Ki67 expression was associated with clinical stage of RbT.19
Massive choroidal invasion has been reported to correlate with poor prognosis in patients with RbT. It is one of the most important HHRFs with short survival and other associated adverse effects for patients with RbT. In the present study, children in whom the eyeball specimens had massive choroidal invasion they had ninefold increased odds of having Ki67 expression compared with other cases in which there was no massive choroidal invasion. This finding was also reported in the study by Kouzegaran et al, in which under univariate analysis, the expression of Ki67 was associated with massive choroidal invasion.17
This study had some limitations including the following: the relatively small number of cases analysed for Ki67 limits the strength of the study. Also, considering the methodology used in selecting the cases for the study which was convenient, this might have contributed to selection bias and therefore making the inferences to be biased.
In conclusion, the present study further reports the importance of Ki67 to be a biomarker, which has shown prognostic role by virtue of its expression to be associated with HHRFs including massive choroidal invasion, positive retrolaminar and surgical margin of the optic nerve as well as advanced tumour stage. Use of Ki67 immunoreactivity may be supplemented as a prognostic biomarker in the planning of the management of the patients. This may help to improve the prognosis of the patients with RbT.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JY: contributed to the designing, data collection and methodology. EAMV: contributed to supervision, designing and methodology. SJ: designing, methodology and critical review of manuscript. All authors contributed to the data analysis and/or interpretation. JY: accepts to be the guarantor of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.