Article Text

Abstract
Objective Visual performance and short-term tolerability of different designs of myopia correcting options, including therapeutically relevant bifocal contact lenses (CL) and spectacle lenses with ‘defocus incorporated multiple segments (DIMS)’ technology were compared.
Methods and analysis In myopic volunteering subjects (n=8; spherical equivalent range: −1 to −7 D) visual acuity (VA) using Landolt C and contrast sensitivity (CS) using contrast C were assessed at three different gaze positions (−22° nasal, +22° temporal and 0° central), corresponding to a gaze through the DIMS area or the clear area of the DIMS lens design, respectively, after short-term wear of each of single vision spectacle lenses (SV), DIMS spectacle lenses (DIMS), monofocal soft CL and centre-near multifocal soft CL (MCL). Also, CS was assessed under photopic and mesopic light conditions with and without glare using sinusoidal gratings at 1.5, 3, 6, 12 and 18 cpd.
Results Mean VA (Landolt C) was −0.12 to –0.10, −0.05 and 0.10 logMAR (SV, DIMS, CL, MCL) at central gaze (0°). At nasal gaze (−22°), VA differed by 0.12, 0.33, 0.05 and 0.01, and at temporal gaze (+22°) by 0.05, 0.26, 0 and −0.08 compared with central gaze values. Mean CS (Contrast C) was 1.74, 1.73, 1.69 and 1.61 logCS (SV, DIMS, CL, MCL) at central gaze at nasal gaze, CS differed by −0.02 to –0.13, −0.01 and −0.01, and at temporal gaze by −0.02 to –0.16, −0.01 and +0.06 compared with central gaze values.
Conclusion When compared with SV, MCL leads to a general decrease in VA and CS, while DIMS did not differ from SV at straight gaze (0° gaze). With DIMS, VA and CS are decreased to a similar level as with the MCL, but only at nasal and temporal gaze.
- Contact lens
- Optics and Refraction
- Treatment other
- Vision
Data availability statement
No data are available. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic?
Spectacle lenses with ‘defocus incorporated multiple segments (DIMS)’ technology reduce myopia progression.
What this study adds?
The reduction in visual performance, when first wearing DIMS, is less compared with centre-near multifocal contact lenses.
How this study might affect research, practice or policy?
The new DIMS technology is the least invasive and most compatible therapy to slow down myopia progression in children and adolescents.
Introduction
Modern myopia correction using spectacle lenses and contact lenses (CL) can be more than a mere correction of the apparent refractive error and the restoration of distance vision. Such optical intervention may also allow for the therapeutic control of myopia progression. As the risk of serious eye disorders in adulthood, such as retinal detachment, glaucoma, early-onset cataracts and myopic choroidal neovascularisation increases with the increase in axial myopia,1 there is a rising interest in the development of a most attractive, therefore, most efficient, option to control myopia progression. Almost all myopia progression in children is due to an excessive eye growth, leaving the eyeball too long for an image of a distant object to be focused on the eye’s retina. The onset and progression of myopia is mainly associated with several environmental factors such as near work, lack of outdoor activity during childhood2 3 and the level of education.4 5 Actual approaches of myopia control aim to slow down excessive eye growth and eventually restore normal growth of the eye in the developing child as described in.6 Well-established optical therapy options are orthokeratology, progressive addition lenses (PAL) and multifocal CL (MCL). Low dose atropine has been established as a pharmacological intervention to inhibit myopia progression.7 8 Atropine could be an available option for a combination therapy with any of the herein mentioned optical means to even enhance the efficiency of myopia control and first promising results were reported.9
Brennen et al advised that the decision to treat myopia should be based on the age of myopia onset and not on the past rate development of already present myopia as usually documented by biometry.10 That is why ideal myopia control options should be safe and applicable in children that have been diagnosed with progressive myopia but also with children that have a high probability of becoming myopic,11 that is, children at young ages with very little myopia or even with no apparent myopia at all.
Recently, novel designs that employ multiple lenslets embedded in a single vision spectacle lens have approached on the market, such as the defocus incorporated multiple segments (DIMS) lenses12 13 and special spectacle lenses with aspherical lenslets.14 These therapy options may provide the safest and least invasive approach for myopia control known to date.
As the developing eye growth towards emmetropia, the retina locally controls eye growth by a visually guided control loop.15 The growth rate of the posterior pole of the eye is influenced by foveal and peripheral image sharpness, and it has been found in several instances that local peripheral myopic defocus can slow down excessive eye growth that underlies myopia progression.16 17 This phenomenon is considered the leverage point for all current optical therapy options for myopia control.
Recent studies on DIMS lenses (MiYOSMART, Hoya Lens) and also on the closely related Highly Aspherical Lenslet Target (Stellest, Essilor) successfully demonstrated the efficacy in slowing myopia progression,18 19 with a therapeutic efficacy which is comparable to that of MCLs and low dose (0.01%, 0.025%) atropine.8 20
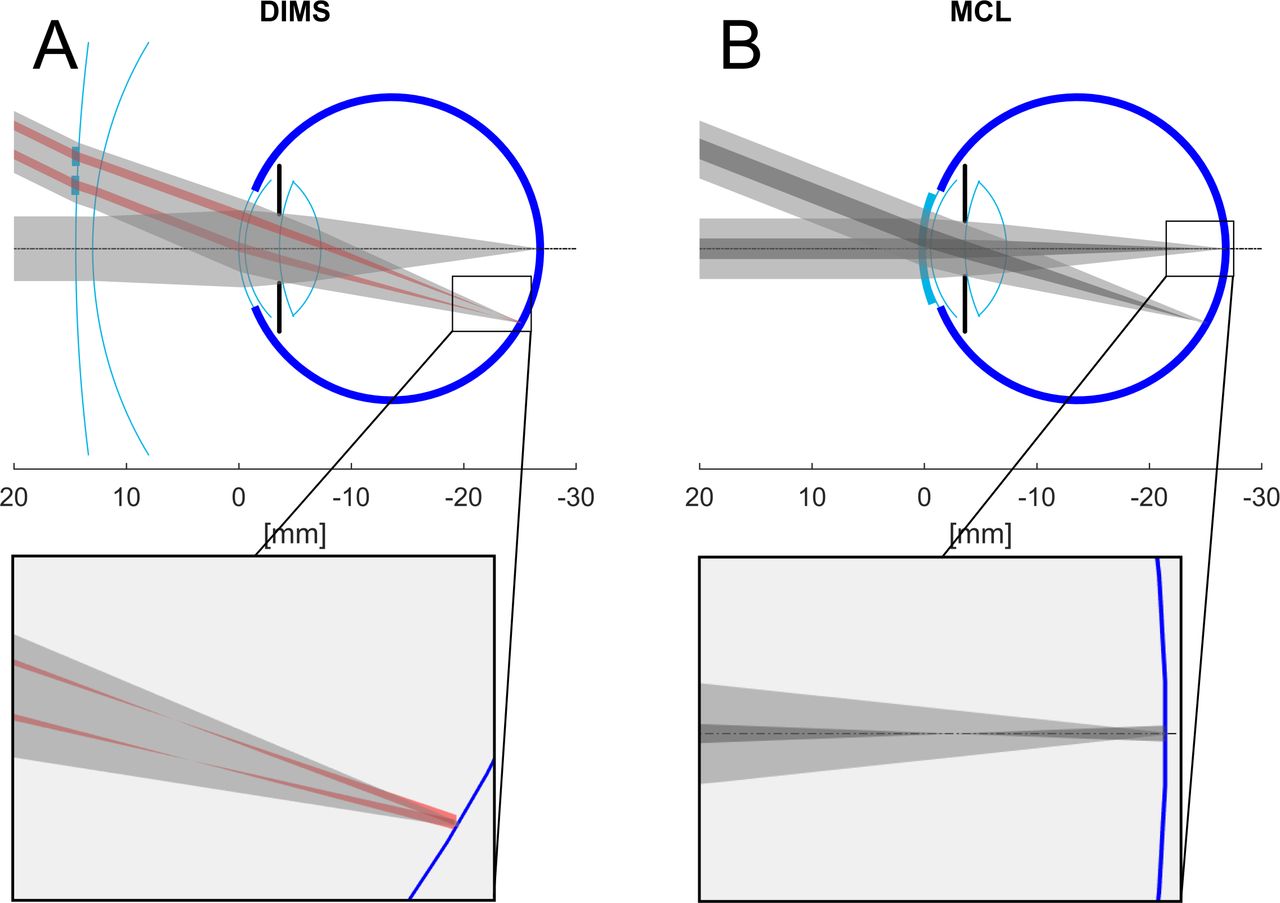
Figure 1 schematically depicts the central and peripheral paths of a bundle of rays passing through two different designs of myopia correcting lenses. Figure 1A shows a spectacle lens with DIMS technology, whose design is based on a plurality of small positive lenslets embedded in a single vision spectacle lens, thus producing a plurality of myopic defoci on the level of the retina; figure 1B shows the bundle of rays passing through an MCL, which owed to its concentric arrangement of near zone and far zone in the lens, forms two distinct focal planes. Figure 1B reveals that the near focus of an MCL forms a blur point on the retina that overlays the sharp far point image. Noteworthy, the DIMS lens does not allow the formation of a second focal plane as it is the case with the MCL, as each lenslet of the DIMS forms its separate focal point and its separate, although smaller blur point. On the basis of the ray tracing, one can picture the resulting image of the DIMS area on the level of the retina as the sharp far point image overlaid by a plurality of nearby and small blur points. The optical and imaging properties of the DIMS lenses have also been modelled in detail by Jaskulski et al.21 When compared with the optics of a traditional concentric-zone dual-focus CL, the DIMS lens generates higher-contrast images at low spatial frequencies (<7 cycles per degree), but lower-contrast at high spatial frequencies 21. It is of high interest, how the optical characteristics of the DIMS actually affects human visual performance.
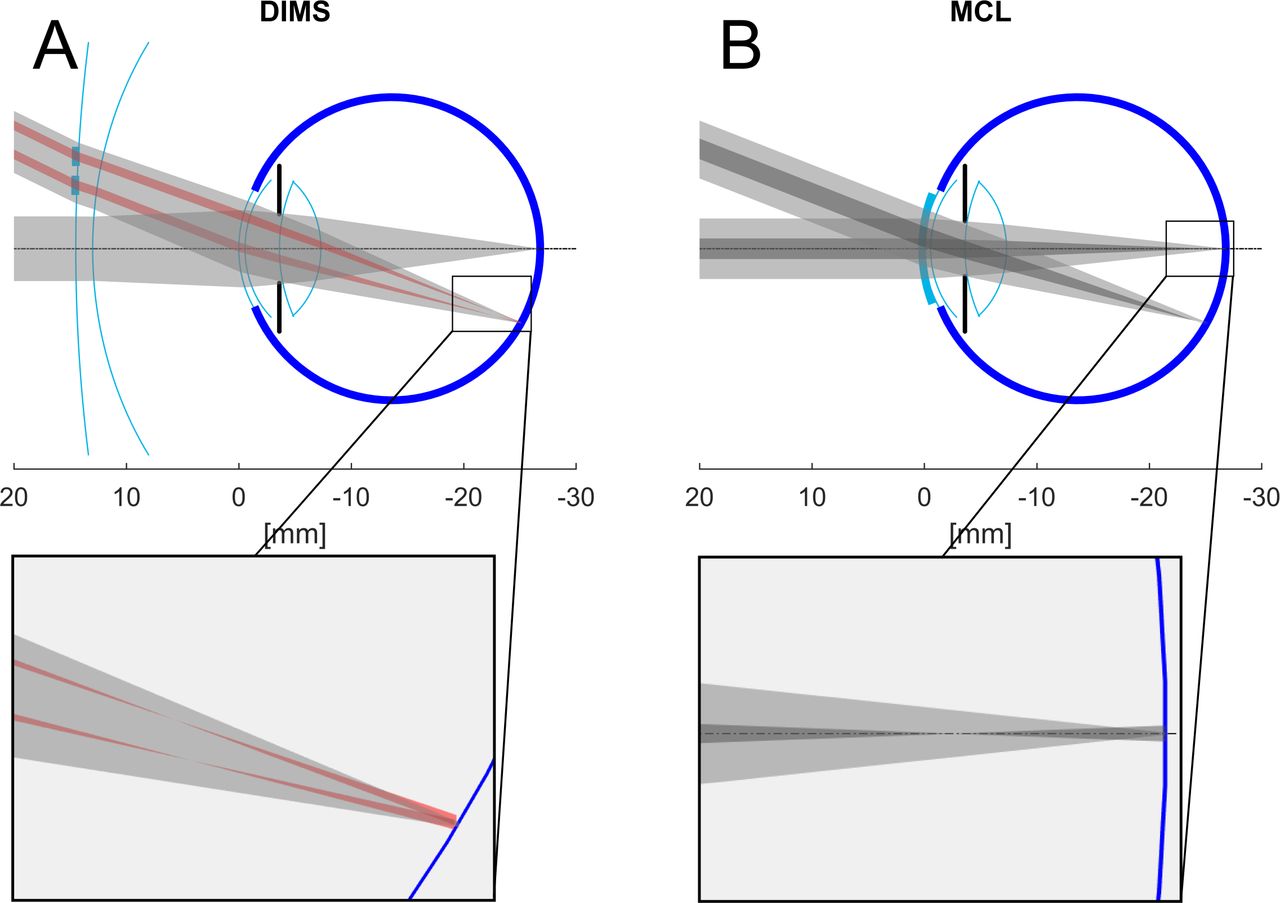
Schematic ray tracing through a myopic eye. Demonstration of ray bundles coming from infinity propagation towards the retina and being refracted by the lenses and the optical media of the eye under two incident angles: 0° (parallel to optical axis) and 22°. Ray tracing was performed using a custom written software routine in Matlab. Parameters were taken from the Lotmar eye model35, except for the axial length which was set to 27 mm (=myopic). (A) DIMS, (B) MCL. Zoomed in images show the foci of the ray bundles in the region of the retina. DIMS, Defocus Incorporated Multiple Segments; MCL, multifocal contact lenses.
In this study, the authors investigated the short-term tolerability and visual performance of the DIMS lenses and compared it to known single vision spectalce lenses, monofocal CL and MCL. The visual performance tests were extended to reflect the particular design of the DIMS lens which has an annular DIMS area with embedded defocussing lenslets around a central single vision area which is free of the lenslets.
Material and methods
Subject group and lenses
Eight myopes (sex: 6 female/2 male, age (mean±SD): 28, 1±3.0 years) with a spherical equivalent (SE) of −4,22±2,29 D (mean±SD) and corneal astigmatism of less than 0.75 D participated in this pilot study. Written informed consent was obtained from the subjects, all employees of the Breyer Kaymak Klabe Eye Clinic in Duesseldorf, after explanation of the nature and possible consequences of this study. All participants had clear optical media, regular corneal astigmatism less 1 D and no ocular pathology. All subjects were long used to wear CL as well as spectacle lenses (soft CL for sports and spectacle lenses for work) and no history of intolerance to either type of correction was reported.
Subjective refraction was performed at 6 m distance following the rule maximum plus to best visual acuity (VA). CL (Dailies Total 1 monofocal, Alcon) and MCL (Dailies Total 1 multifocal-medium centre-near add(+2 dpt.), Alcon) were ordered with SE values corrected by vertex distance. Overrefraction was performed 30 min after first wearing the CL and MCL and were reordered when values differed by 0.5 D or more. DIMS (MiyoSmart, Hoya Lens) and single vision (SV) (HOYA single vision spectacle lens with refractive properties equal to the MiyoSmart lens) were ordered with subjective refraction values corrected for vertex distance when wearing the chosen frames. DIMS and SV were properly mounted in the individually fitted frames at a local optician.
Short-term wear and visual performance
Subjects’ visual performance with each the four correction designs, SV, DIMS, CL, MCL, was examined after about 1 hour of initial short-term wear on four consecutive days, where the order of the optical design and tests were randomly selected. After the respective correction was handed out, the subject was asked to perform different visual tasks (pc work, looking into the distance, move around in the room, go for a walk outside, reading/smartphone) for 1 hour in a standardised environment, this initial and only adaptation phase immediately followed by the individual visual performance tests.
Measurement of VA and contrast sensitivity at three different gaze positions
The automated FrACT (Freiburg Acuity and Contrast Test) V.3.1022 was employed to assess VA and contrast sensitivity (CS) in three different horizontal gaze positions. FrACT using Landolt C has been chosen over the ETDRS chart as some ETDRS letters are considered to be recognised more easy than others under low contrast conditions and due to our observation that the subjects memorise the letters after repeated measurements at short intervals. The three gaze positions were chosen to test the visual performance where a subject gazing particularly through the annular DIMS area of the DIMS lens and compare it to the standard designs of optical corrections. Figure 2 shows the schematic top view of an eye looking through the central zone of the DIMS lens at a straight gaze (0° gaze) (figure 2A) or through the annular DIMS area of the lens with a nasal or temporal gaze (−22°/+22° gaze) (figure 2B).

Schematic drawing of an eye in central (A) and nasal or temporal (B) gaze position. Z’ is the centre of rotation of the eye. Gaze angle α is 22° when the distance from Z’ to the back of the DIMS lens is 25.5 mm and the distance from the centre of the DIMS area to the optical axis of the DIMS lens is 10.5 mm. DIMS, defocus incorporated multiple segments.
In all tests, high and low Landolt C optotypes were presented monocularly to the subject through a calibrated and gamma-corrected 23 inch LCD monitor (ColorEdge CS 230, Eizo Nanao, Japan) placed 3 m in front of the subject’s head that was fixed in a chinrest. For the contrast test, the size of the ‘contrast C’ corresponded to 30 arc min or 0.8 logMAR minimum angle of resolution (MAR). For the temporal and nasal gaze conditions, the optotype monitor was moved 1.16 m sideways left or right from the original forward position and the subjects were asked to turn their eye to the optotype monitor without moving their head, that was fixed in a chin rest, which then corresponded to a nasal or temporal gaze (−22°/+22° gaze), respectively.
CS and Glare
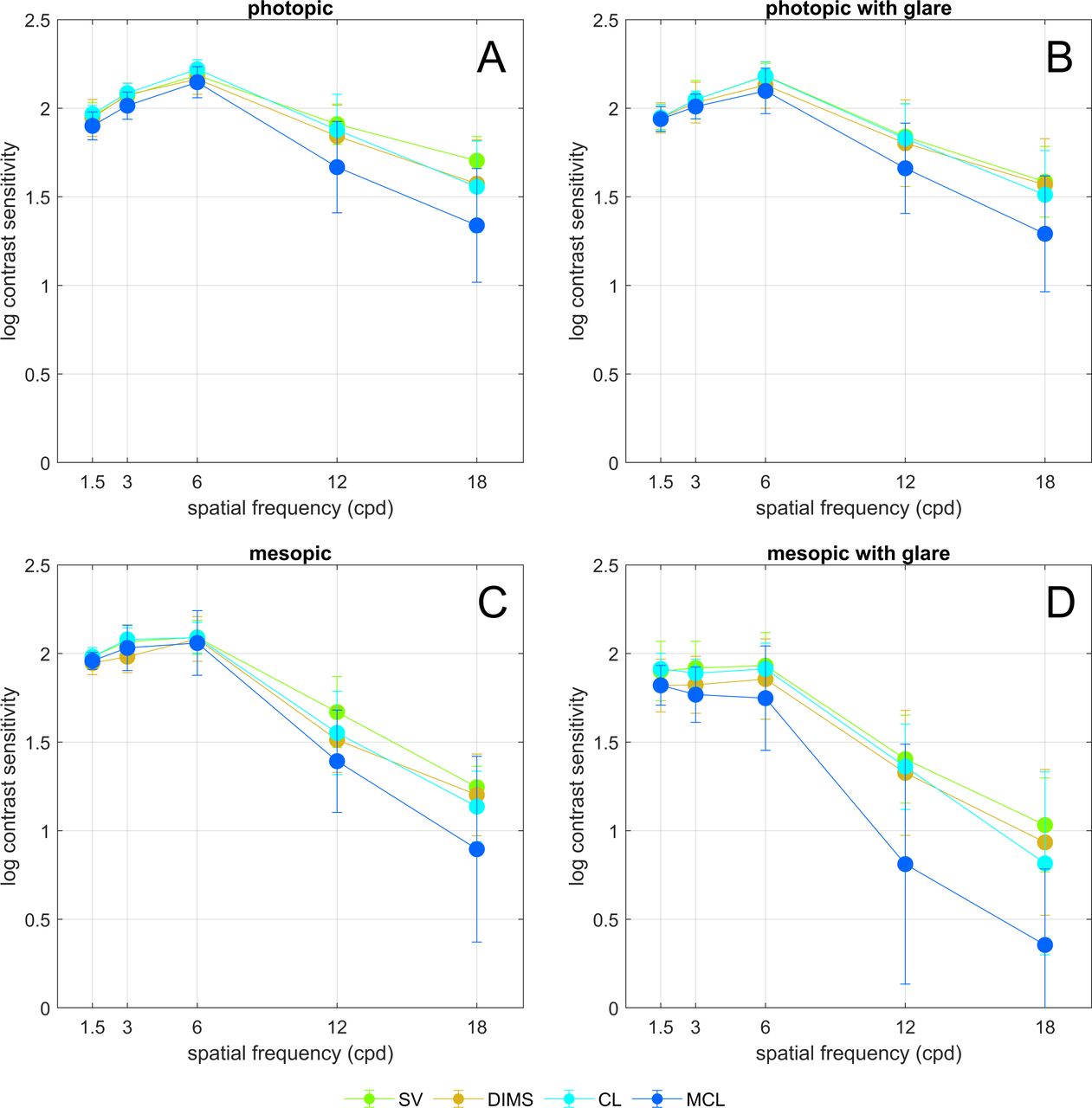
A visual function analyzer (VFA) OPTEC 6500P (Stereo Optical, Chicago, USA) was used to additionally evaluate the binocular CS under mesopic conditions (3 cd/m2), with or without glare light (28 Lux), and under photopic conditions (85 cd/m2), with or without glare light (135 Lux), for each the four corrections, SV, DIMS, CL, MCL, using the functional acuity contrast test (F.A.C.T.) protocol with sine wave gratings of 1.5, 3, 6, 12 and 18 cpd in 9 contrast steps, each corresponding to 0.15 logCS.23
Sample size calculation
G*Power (V.3.1.9.4)24 was used to perform sample size calculation for the Wilcoxon signed-rank test with an alpha error of 0.05 and power of 90% for two-sided testing. An assumed change in VA of (mean±SD) 0.3±0.2 logMAR from central to nasal/temporal gaze position lead to a total sample size of 8. Null hypothesis can be denied if calculated W is less than critical W of 3.
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Results
VA and CS at different gaze positions
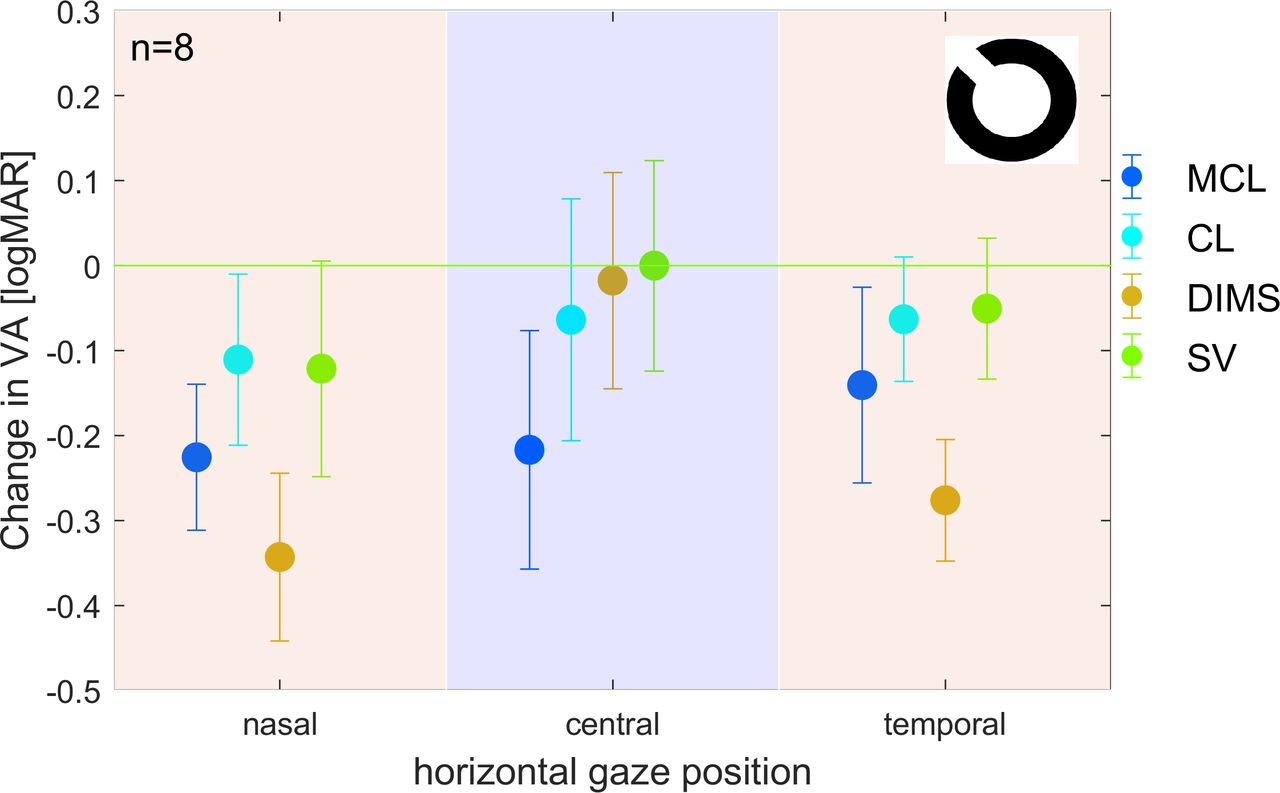
Figure 3 shows the VA as assessed after short-term wear of SV, DIMS, CL and MCL for each of the three gaze positions (−22°, 0°, +22°). Absolute values of central monocular VA (0° gaze) were (mean±SD in logMAR) −0.12±0.12, –0.10±0.13, –0.05±0.14 and 0.1±0.14, for SV, DIMS, CL and MCL respectively; nasal monocular VA (−22° gaze) were 0.00±0.17, 0.23±0.14, −0.01±0.18 and 0.11±0.12 (SV, DIMS, CL, MCL); and temporal monocular VA (+22° gaze) VA were (mean±SD in logMAR) −0.07±0.14, 0.16±0.12, −0.05±0.14 and 0.02±0.17 (SV, DIMS, CL, MCL).

Results of VA testing for the three different gaze positions (−22°, 0°, 22°) as measured with single vision lens (SV), spectacle lens with defocus incorporate multiple segments (DIMS), contact lens (CL) and multifocal CL (MCL). The measurements were performed under monocular conditions with the participants left eye occluded. Values for central gaze position are normalised to zero. Error bars represent SD. VA, visual acuity.
Figure 4 shows CS as assessed after short-term wear of SV, DIMS, CL and MCL for each of the three gaze positions (−22°, 0°, +22°). Absolute values of central monocular CS (0° gaze) were (mean±SD in logCS) 1.74±0.15, 1.73±0.18, 1.69±0.18 and 1.61±0.22 for SV, DIMS, CL and MCL, respectively; absolute values of monocular CS with nasal gaze were (mean±SD in logCS) 1.72±0.22, 1.60±0.18, 1.68±0.14, and 1.60±0.21 (SV, DIMS, CL, MCL); absolute values of monocular CS with temporal gaze were (mean±SD in logCS) 1.76±0.20, 1.58±0.17, 1.68±0.15 and 1.67±0.19 (SV, DIMS, CL, MCL).
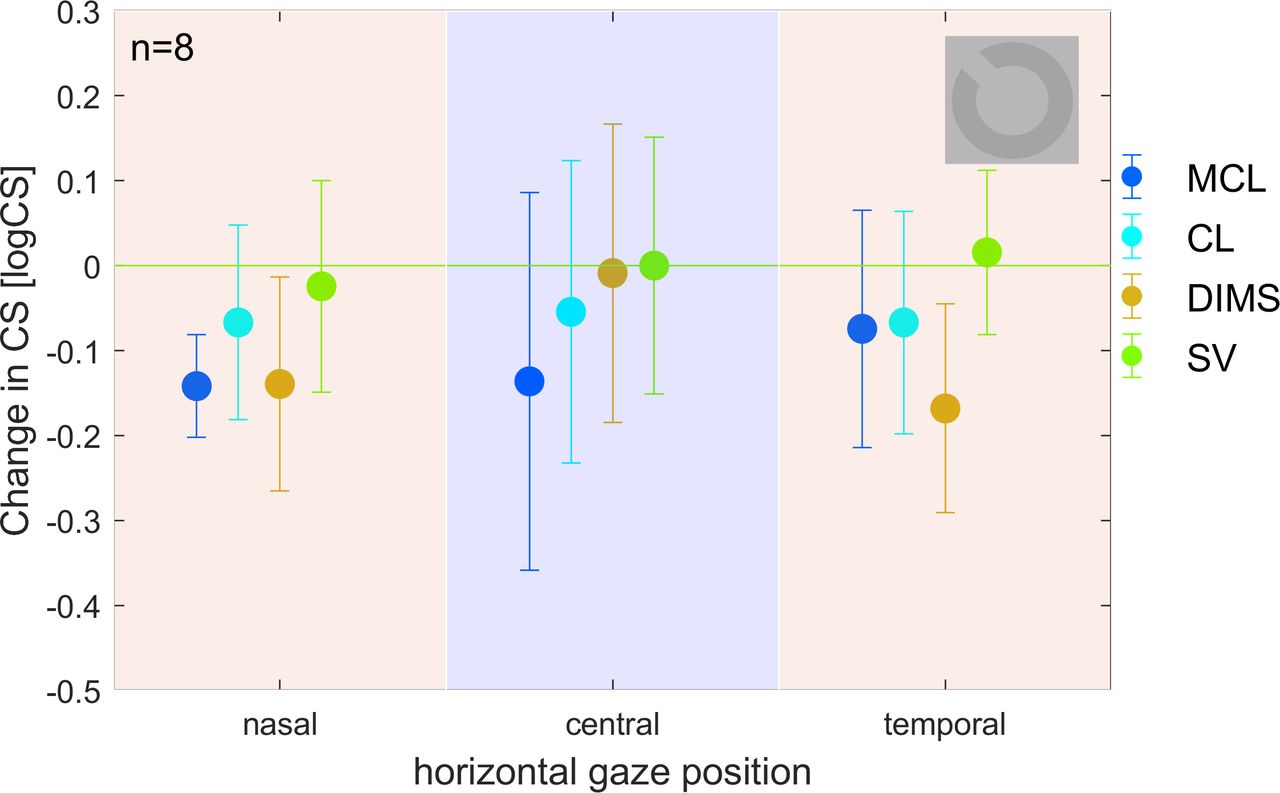
Results of CS testing for the three different gaze positions (−22°, 0°, 22°) as measured with single vision lens (SV), spectacle lens with defocus incorporate multiple segments (DIMS), contact lens (CL) and multifocal CL (MCL). The measurements were performed under monocular conditions with the participants left eye occluded. Values for central gaze position are normalised to 0 logCS. Error bars represent SD. CS, contrast sensitivity.
Photopic and Mesopic CS and Glare
Figure 5 shows the results of the CS testing with and without glare under photopic (figure 5A,B)and mesopic (figure 5C,D) conditions. SV, DIMS and CL did not differ in visual quality at all four illumination conditions. In contrast, MCL exhibited a decrease in CS at higher spatial frequencies most prominent in mesopic condition and/or with glare (eg, figure 5D).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CS measured at 1.5, 3, 6, 12 and 18 cpd with the Optec 6000P. (A) photopic, (B) photopic with glare, (C) mesopic, (D) mesopic with glare (single vision lens (SV), single vision lens with defocus incorporate multiple segments (DIMS), contactlens (CL), multifocal CL (MCL)). CS, contrast sensitivity.
Discussion
The impact of myopia controlling lenses on visual performance had been investigated in several studies. Li et al25 investigated the influence of different lenslet configurations on short-term visual performance expressed in differences in VA and CS25 and found a significant decrease in VA and CS for spatial frequencies from 6 to 18 cpd when wearing DIMS and looking through the lenslet zone as compared with SV. In line with these findings, our pilot study confirms that gazing through the central single vision zone of the DIMS does not reduce VA or CS of myopic subjects and the DIMS visual performance fully corresponds to the SV lens, and in the temporal and nasal gaze condition VA with DIMS lens is decreased by 0.23±0.19 logMAR over the SV lens. This is also confirmed by the previous findings of Lu et al26 who addressed the levels of adaptation and acceptance of the DIMS lenses with Chinese volunteers and found no significant difference in the central vision between DIMS lenses and traditional SV lenses. We claim that in real life, a subject would rather look through the central single vision zone of the DIMS at almost all instances for performing demanding visual tasks and thus would not practically experience a loss in VA conferred by the annular DIMS area. Of note, the absolute VA of the DIMS lens in the nasal and temporal gaze conditions was 0.23±0.14 and 0.16±0.12 logMAR, respectively, which is, compared with the VA in central gaze position a decrease in VA of about 0.3 logMAR which corresponds to a defocus of less than about 0.5 dpt27 and this would still not rule out the possibility to operate a motorised vehicle.28
Also for CS, we found a decrease in CS in the DIMS lenses as compared with the SV lenses only in the nasal and temporal gaze conditions and of only −0.12±0.20 and −0.18±0.20 logCS, respectively, which, according to the considerations of Radhakrishnan et al29 corresponds to a defocus of about 0.5 dpt. The observed loss in VA in nasal and temporal gaze position can also be used as a boundary to describe the usable width of the intermediate viewing zone of modern PAL. As shown in,30 the width of the intermediate viewing zone of PALs with a VA loss of less than 0.3 logMAR is smaller than the clear central zone in DIMS (9 mm). Noteworthy, PALs, which are reportedly safe and tolerable, unwanted astigmatism occurs in the peripheral zone of the lens,31 but in the DIMS lenslet design such astigmatism cannot develop.
Li et al25 compared the DIMS design with alternative optical lens designs which also showed efficient reduction in myopia progression.25 These designs are based on concentric rings of highly aspherical lenslets or of slightly aspherical lenslets and showed less reduction in CS at high spatial frequencies (>12 cpd) as compared with DIMS.
The MCL investigated in this study was a ‘centre-near’ type where the central optical zone refracts the incoming light for near vision and the peripheral zone for far vision (figure 1B). In general this design allows the perception of halo and glare being decreased when pupil size increases. This is important when one would opt for a myopia control therapy based on MCL combined with low dose atropine as even low dose atropine has some inevitable mydriatic effect. CL, as placed directly on the eye’s cornea are thought to provide the same visual performance at all gaze angles. In line with this, we found a decrease in both, VA and CS, imposed by the MCL over SV lenses at all gaze angles. In direct comparison to the DIMS lenses, the MCL had decreased VA and CS at the straight gaze angle (0° gaze) and at temporal and nasal gaze angles (−22°/+22° gaze) the decrease in VA and CS imposed by the MCL did not differ from the reduction imposed by the DIMS lenses.
From the binocular tests with the VFA, we found no significant differences in contrast vision with SV, CL and DIMS at all illumination levels and glare conditions. Noteworthy, MCL had inferior visual performance in particular at higher spatial frequencies. The measured CS with MCLs under photopic conditions (figure 5A,B) is in line with the findings of Piñero et al,32 who compared the visual performance achieved with different MCL models.
The current pilot study aimed to determine the individual visual performance of myopic subjects when wearing SV, DIMS, CL and MCL. Despite the small sample size of our pilot study, the results indicate that correcting myopia and inhibiting or preventing myopia progression by means of modern optical correction aids is a feasible and safe approach. When testing the novel DIMS design against standard corrections (SV and CL) and against a centre-near MCL, the DIMS design stands well, even under the critical and adverse conditions selected for this study, that is, (1) testing short-term performance only, without any chance for a considerable adaptation of the subject to the respective correction; (2) testing visual performance at artificial gaze conditions, characterised in continuously looking through the DIMS area the DIMS lenses during the tests, without the subjects being allowed to turn their head in the direction of the stimulus, what they would normally do in real life, and employing adult subjects which all had a background as optometrist or scientist in an ophthalmological clinic, which are considered to be more sensitive to potential visual impacts than children, subjectively, due to their experience an attitude, and objectively due to their smaller pupil sizes This has also been speculated by Lu et al.26
Our study shows that even under those artificial adverse conditions, subjects did not experience any significant impact on visual performance by the DIMS lenses. Even if the subject had looked constantly sideways and through the annular DIMS area the experienced reduction in visual quality had not been considerably larger than the general impairments imposed by the MCLs in this study or those known from PALs.30 As reported by Lam et al,33 DIMS and SV lens could hardly be differentiated by their appearance, and most children in the Asian DIMS study were not even aware of the DIMS features; and a few children in the treatment group had recognised the DIMS, but had had no particular difficulties in using the lens as their previous spectacle lenses. Thus, DIMS are the least invasive treatment option, which always cause an effect to reduce myopia progression due to the arrangement of the lens segments and cause hardly any side effects compared with atropine.34
Data availability statement
No data are available. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
The tenets of the Declaration of Helsinki were followed and the study was carried out as approved by the competent ethics committee (ÄK Nordrhein No. 2018124).
Acknowledgments
Results presented here had been generated as part of a master thesis at Ernst-Abbe University Jena by M. Sc. Saskia Schuetz who is also coauthor. The authors would like to thank the HOYA company for providing the MiYOSMART lenses.
References
Footnotes
Contributors HK created the concept and the study design, wrote the manuscript and acts as the guarantor, BG assisted in creating the study design; SS collected and analysed the data. KN analysed the data and wrote the manuscript; AL, BS and WS reviewed the manuscript. HS reviewed and revised the manuscript. HK and KN contributed equally to this work and share first authorship.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests HK is a consultant for Hoya Lens Germany performing presentations on the MiYOSMART lenses.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.