Article Text

Abstract
Background/aims To describe the clinical presentation and treatment response of dupilumab-associated ocular surface disease (DAOSD).
Methods This is a retrospective case series of atopic dermatitis patients with DAOSD treated with dupilumab. All consecutive patients with atopic dermatitis referred by dermatologists for suspicion of DAOSD between May 2018 and June 2020 were systemically assessed by a single ophthalmologist. Presenting signs of DAOSD, duration of treatment and associated response are described.
Results Twenty-eight patients had DAOSD during the study period. Average age was 45.6±14.8 years and 13 (46%) were female. Average follow-up was 15±10 months. Most presentations consisted in diffuse, inflammatory conjunctivitis (n=19, 68%). Other signs included peripheral corneal infiltrates (n=7, 25%), limbal nodules (n=7, 25%) and dry eye syndrome (n=6, 21%). To control ocular symptoms, tapering of corticosteroid eyedrops was slow: taper duration of strong and mild corticosteroid eyedrops averaged 10±8 weeks and 49±34 weeks, respectively. Four patients (14%) required an increase of corticosteroid eyedrops during taper due to clinical deterioration. Corticosteroid eyedrops were still required at final follow-up among 10 patients (36%). Dupilumab was temporarily stopped in 3 patients (11%), one of which did not wish to resume dupilumab for unrelated reasons. Symptomatic improvement and/or complete resolution was achieved in 25/26 patients at follow-up (96%) with empirical treatment.
Conclusions DAOSD may follow the course of a chronic illness. Long-term corticosteroid eyedrops were required in many patients and when taper was possible, this was done after a prolonged treatment duration. Most patients’ ocular symptoms could be controlled, allowing dupilumab continuation.
- Conjunctiva
- Cornea
- Drugs
- Inflammation
- Treatment Medical
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known about this subject?
Studies have described many clinical signs that can be found in dupilumab-associated ocular surface disease (DAOSD). It is also known that it occurs frequently in patients treated with dupilumab for atopic dermatitis.
What are the new findings?
We report the evolution of patients with DAOSD under treatment. Notably, patients improved under topical corticosteroid eyedrops, but they required long durations of treatment: 2–3 months of strong topical corticosteroid eyedrops and around a year of mild topical corticosteroid eyedrops to improve and maintain their state.
How might these results change the focus of research or clinical practice?
This might encourage clinicians to taper topical corticosteroids more slowly and carefully in patients with DAOSD to avoid recurrences of disease and deterioration of symptoms. It will also be important to explore possible corticosteroid-sparing treatments for these patients to reduce the possible adverse effects associated with corticosteroids.
Introduction
The mainstay of treatment in atopic dermatitis (AD) includes moisturising lotions and topical corticosteroids. However, in select patients, newer generation therapies can be used, including biologics such as dupilumab. Dupilumab is a human monoclonal antibody targeting the α subunit of the interleukin 4 receptor, which affects the interleukin 4 and interleukin 13 pathways. It is the first antibody-based treatment approved by the United States Food and Drug Administration (FDA) for the management of moderate to severe AD since 2017.1 In randomised placebo-controlled trials, dupilumab increased patients’ quality of life, reduced mental health symptoms and improved AD signs and symptoms2 but was not without adverse effects.
Conjunctivitis is a common complication2 reported in 8.6%–22.1% of patients treated with dupilumab compared with 2.1%–11.1% of patients treated with placebo with AD.3 A similar increase was not found in patients treated with dupilumab with other diseases.3 Additionally, 23 of 85 patients (27%) developed ocular surface disease while on dupilumab4 and case reports have described different instances of blepharoconjunctivitis,5 cicatricial ectropion,6 nodular swelling of the limbus,7–10 cicatricial conjunctivitis,11 punctal stenosis,12 13 proliferative conjunctivitis,14 episcleritis15 and corneal ulceration16 17 under dupilumab treatment.
Patients with AD are already at an increased risk of ocular complications,18 including signs and symptoms which may resemble dupilumab-associated ocular surface disease (DAOSD). These include periocular AD, atopic keratoconjunctivitis, bacterial blepharoconjunctivitis, herpetic eye disease, keratoconus and tear film dysfunction.19 Current research aims to detail the spectrum of DAOSD, which is now recognised as an entity under the name DAOSD or dupilumab-induced ocular surface disease.20 It, however, remains to be seen how to best treat this entity and what to expect long term. We, therefore, describe a retrospective cohort of patients with DAOSD and detail duration of treatment and corticosteroid requirements over time.
Methods
Study design and population
This retrospective case series adhered to the tenets of the Declaration of Helsinki. We reviewed the medical records of all consecutive patients treated with dupilumab for AD who had suspicion of DAOSD. These patients were referred to our cornea service by dermatology between May 2018 and June 2020. Referrals came from outpatient dermatology clinics or an academic tertiary dermatology care centre. Referring dermatologists included general dermatologists and subspecialty dermatologists (eg, skin allergies and contact dermatitis specialists). They were recommended to send all patients who had ocular symptoms following start of dupilumab to the cornea service for assessment. All ophthalmological follow-ups until August 2021 were included.
Patient charts were reviewed, and the following characteristics were included: demographics, severity of AD as described by the referring dermatologist, including Eczema Area and Severity Index (EASI), body surface area (BSA), Dermatology Life Quality Index (DLQI), Investigator Global Assessment (IGA) Scale and Numerical Rating Scale (NRS), when available, date of initiation of dupilumab treatment, date of cessation of dupilumab treatment if applicable, pinhole visual acuity (PHVA) at first consultation and at final follow-up in metric Snellen notation defined as the best visual acuity obtained using the patient’s current refraction with or without improvement with pinhole, previous ocular history, including conjunctivitis, atopic blepharitis, rosacea or meibomian gland dysfunction, dry eye syndrome and herpes simplex keratitis, time to onset of ocular symptoms, ocular treatment attempted prior to cornea consultation and treatment started by the cornea specialist, including preservative-free artificial tears, strong corticosteroid eyedrops (eg, prednisolone 0.12%, prednisolone 1%, dexamethasone 0.1% and difluprednate 0.05%), mild corticosteroid eyedrops (eg, fluorometholone 0.1%, fluorometholone 0.25%, loteprednol 0.2%, loteprednol 0.5% and rimexolone 1%), antihistamine-mast cell stabilisers (eg, olopatadine 0.2%), periocular corticosteroids (eg, hydrocortisone 0.5%) and periocular calcineurin inhibitors (eg, tacrolimus 0.03%), duration of treatment using topical corticosteroid eyedrops and patient evolution under ocular treatment.
Typically, patients were started on artificial tears and antihistamine-mast cell stabilisers to control the portion of the ocular symptoms similar to dry eyes and allergic keratoconjunctivitis, respectively, as both topical medications may target some hypothetical pathophysiological mechanisms involved and have been used with some success in DAOSD.8 21 Next, initial treatment could also include a loading dose of a strong or mild corticosteroid eyedrop depending on the severity of the symptoms and the inflammatory component (eg, diffuse conjunctivitis). Eyedrops were often started at 4 times daily with a taper of one drop every 2–4 weeks depending on treatment response. This was tailored to the patient’s symptoms and clinical response. Periocular corticosteroids or calcineurin inhibitors were prescribed to address remaining cutaneous irritation from AD at the time of consultation. Patient evolution was categorised as improvement, stable and deterioration of disease activity based on a combination of subjective patient symptoms and on clinical aspect. This was established by comparing symptoms as reported by the patient and objective findings at final follow-up to findings at initial presentation. A treatment failure was defined as the need for an unplanned increase in topical corticosteroid eyedrops due to clinical deterioration after start of treatment. Patients who had stopped their treatment prematurely or did not follow the taper as prescribed were not deemed to have had a treatment failure.
Ophthalmological assessment
Every patient treated with dupilumab and referred to the cornea service by dermatologists were systematically assessed using slit lamp biomicroscopy by a single experienced cornea subspecialist (P-AL) with more than 30 years of clinical experience. The presence of blepharitis, conjunctivitis, episcleritis, limbal involvement with nodules and Horner-Trantas-like dots and keratitis, particularly peripheral or central corneal infiltrates, was specifically sought.
Suspicion of DAOSD was established following appearance of new or increased ocular surface anomalies based on the clinical assessment of the patient. Suspicion of DAOSD was also diagnosed if the patient had experienced an increase in their symptoms of keratoconjunctivitis on starting the treatment, in the absence of another explanation for the symptoms and findings, and if symptoms recurred after restarting dupilumab as was defined by Nahum et al.21
Statistical analysis
Data are presented as mean and SD for continuous, normally distributed variables, as median (first quartile and third quartile) for continuous, non-normally distributed variables and as frequencies (percentages) for categorical variables. Shapiro-Wilk test and Q–Q plots with 95% CIs were used to test for normal distribution of continuous variables. Vision was converted from metric Snellen notation to logarithm of the minimum angle of resolution for analysis purpose.22 Initial and final PHVA were compared using Wilcoxon signed-rank test. Statistical analyses were performed using IBM SPSS Statistics for Windows (V.27.0). All analyses were conducted at the 0.05 significance level.
Results
Patient baseline characteristics
Twenty-eight patients with dupilumab-treated AD referred to the cornea service during this period were deemed to have suspicion of DAOSD and were included in this study. Other cases referred by dermatology during this period with other clear diagnoses were excluded (n=3). Two of these patients had herpes simplex virus keratitis, while the other had staphylococcal and seborrhoeic blepharitis, which was already known and had not deteriorated after starting dupilumab.
Patient baseline characteristics are presented in table 1. Average age was 45.6±14.8 years at the time of consultation. Of these, 13 patients were female (46%). The severity of AD was graded as severe by the referring dermatologist in 23 patients and was not provided in the others. Among 6 patients who had available AD severity scores prior to start of dupilumab treatment, average scores were as follows: EASI 22.75±4.11, BSA 35.25%±18.89%, DLQI 23.0±4.3, IGA 3.7±0.6 and NRS 9.75±0.35. Some patients did not have previous ocular history or known AD eye involvement (n=6, 21%); however, many were previously known for atopic blepharitis (n=17, 61%).
Baseline characteristics and ocular presentation of 28 patients who presented with suspicion of dupilumab-associated ocular surface disease
Ophthalmological manifestations
Median presenting PHVA was 0.02 (0.00, 0.055) (Snellen equivalent: 20/20–1). Following initiation of dupilumab, median time to onset of ocular symptoms was 4 months (1 month, 7 months) (range: 0–16 months). Most patients had a time to onset greater than 4 months (n=17, 61%) and most had bilateral ocular signs or symptoms (n=26, 93%). The frequency of the different ocular signs is illustrated in table 1. The most common finding was conjunctivitis (n=19, 68%), often important and diffuse giving it an appearance of possible episcleritis. The inflammation could also include keratitis with or without perilimbal nodules or frank sectorial episcleritis. Photographic evidence of these specific findings is shown in figures 1 and 2. Most patients (n=15, 54%) had 1 ocular sign at presentation (ie, among blepharitis, conjunctivitis, dry eye syndrome, limbal involvement, peripheral corneal infiltrates, central corneal infiltrates or episcleritis), while 6 patients (21%) had 2, 4 patients (14%) had 3, 2 patients (7%) had 4 and 1 patient (4%) had five.

Appearance of limbal inflammation in patients with dupilumab-associated ocular surface disease characterised by sectorial retrolimbal hyperaemia and the presence at the superior limbus of (A, B) Horner-Trantas-like dots and (C) limbal nodules.
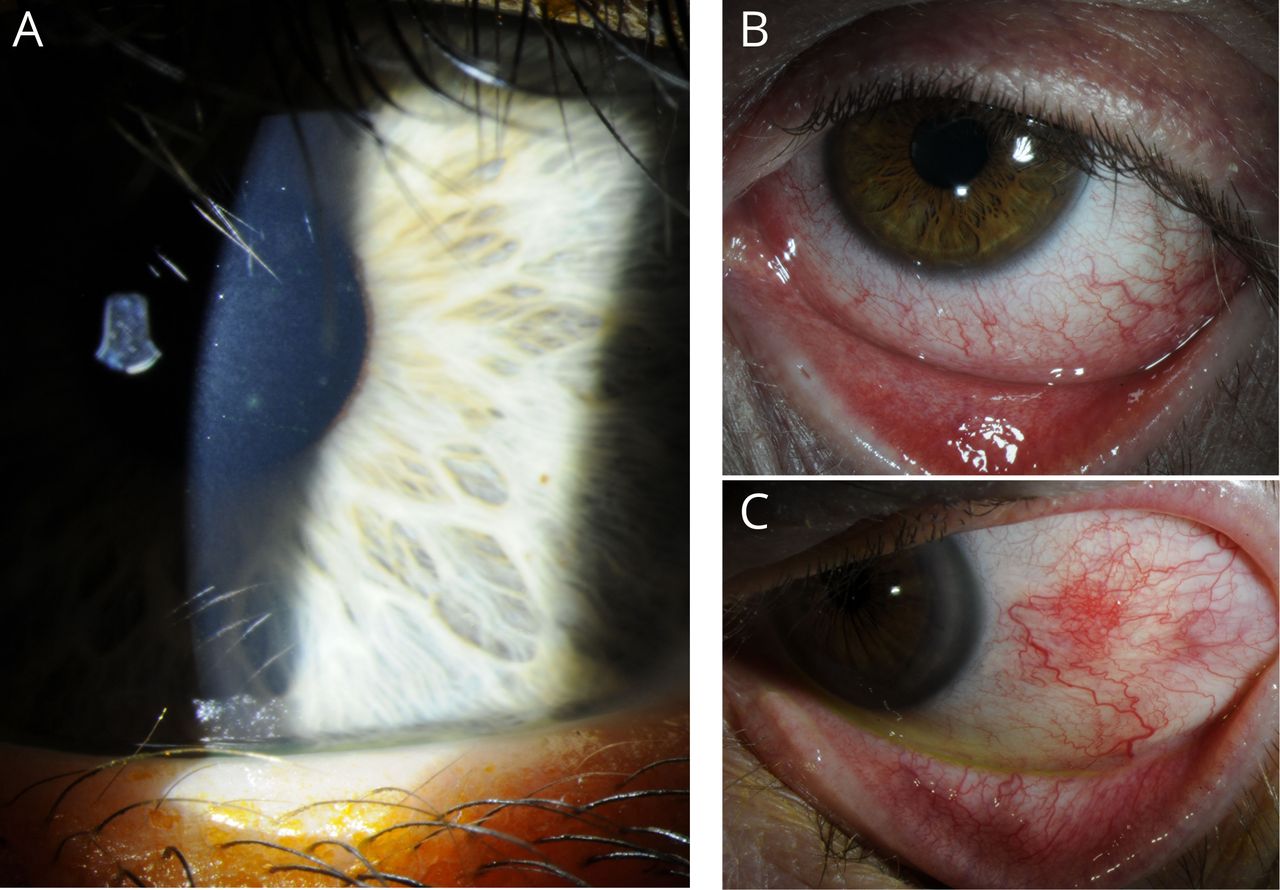
Findings of dupilumab-associated ocular surface disease illustrating (A) paracentral corneal infiltrates, (B) diffuse inflammatory conjunctivitis and (C) sectorial episcleritis.
Among 6 patients who did not have any previous ocular history or known AD eye involvement, the presentation included 3 patients (11%) with inflammatory conjunctivitis only, 1 patient (3%) with blepharitis only, 1 patient (3%) with peripheral corneal infiltrates only and 1 patient (3%) with blepharitis, limbal nodules and peripheral corneal infiltrates.
Treatment modalities and response
Prior to consulting the cornea service, most patients (n=27, 96%) had tried treatments for their ocular condition using combinations of periocular topical creams or ointments prescribed for their AD and/or ocular eyedrops. These include artificial tears (n=18, 64%), antihistamine-mast cell stabilisers (n=7, 25%), antibiotic eyedrops (n=7, 25%), periocular corticosteroid creams (n=8, 29%), periocular calcineurin inhibitors (n=7, 25%) and tetryzoline eyedrops (n=2, 7%). Three patients (11%) had consulted another eyecare professional prior to their initial cornea consultation and were prescribed mild corticosteroid eyedrops. One of them was also prescribed calcineurin inhibitor (ie, cyclosporine) eyedrops.
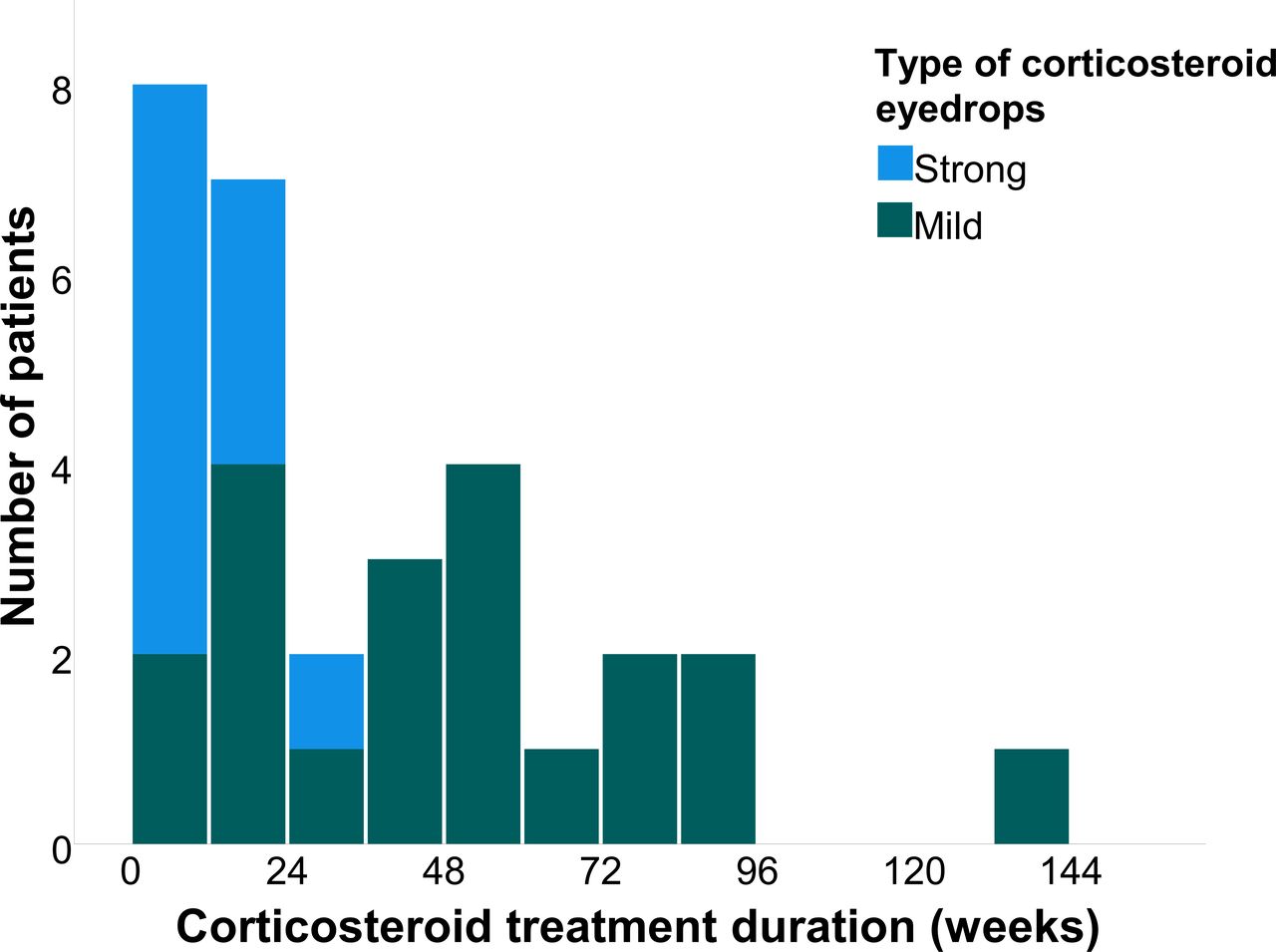
After the initial cornea consultation, patients were followed for an average duration of 15±10 months. Two patients (7%) were discharged after the first consultation with supportive care due to mild DAOSD with dry eye symptoms and no indication for follow-up in ophthalmology. Most patients were empirically treated with antihistamine-mast cell stabilisers in 24 patients (86%), strong ocular corticosteroid drops in 12 patients (43%), mild ocular corticosteroid drops in 17 patients (61%), preservative-free artificial tears in 24 patients (86%), periocular topical corticosteroids in 12 patients (43%) and periocular calcineurin inhibitors in 11 patients (39%). Among patients receiving topical ocular corticosteroids with tapers, strong corticosteroid eyedrops duration averaged 10±8 weeks (range: 2–30 weeks), while mild corticosteroid eyedrops duration averaged 49±34 weeks (range: 4–142 weeks). The number of patients who required different durations of corticosteroid eyedrops treatments are illustrated in figure 3. Among the entire cohort, corticosteroid eyedrops were still required at final follow-up among 10 patients (36%).

{kind=link}
{kind=link}
{kind=link}
Histogram illustrating the number of patients and corresponding treatment duration of strong and mild corticosteroid eyedrops in weeks that were required in managing dupilumab-associated ocular surface disease.
In 3 patients with DAOSD (11%), dupilumab treatment was stopped. The first stopped treatment for 4 months, then had a recurrence while dupilumab was stopped, and recurred once again after dupilumab was restarted. The second stopped dupilumab within 4 months of having started for reasons unrelated to their ocular condition as they only had mild dry eye disease. The third had stopped the treatment for 1 month without change to their ocular condition.
In this last patient, cationic emulsion cyclosporine 0.1% was initiated as an off-label use due to uncontrolled DAOSD. They presented with blepharitis, conjunctivitis, limbal nodules, as well as peripheral and central corneal infiltrates. Previous treatments included artificial tears, antihistamine-mast cell stabilisers, strong and mild corticosteroids eyedrops and periocular corticosteroids. Under cationic emulsion cyclosporine 0.1%, the patient could resume dupilumab therapy.
At follow-up, four patients fit the criteria for treatment failure (ie, need to increase topical corticosteroid eyedrops due to clinical deterioration). This occurred on average 17±11 months after the start of corticosteroid therapy. Two other patients had recurrence of symptoms on premature cessation of treatments for whom treatment needed to be reinstated. That said, there was symptomatic improvement and/or complete resolution of ocular findings in 25/26 patients with follow-ups (96%), while disease remained stable in the patient under cationic emulsion cyclosporine 0.1%. At final follow-up, median PHVA was 0.02 (0.00, 0.040) (Snellen equivalent: 20/20–1). This was not significantly different from initial PHVA (p=0.62).
Discussion
Our study reports on clinical characteristics and ophthalmologic examination findings of patients with DAOSD. We identified clinical findings of DAOSD that are uncommon in the literature.23 A significant proportion of our patients presented with limbal nodules, sometimes accompanied by Horner-Trantas-like dots. This form of limbal inflammation may be seen in the limbal form of vernal keratoconjunctivitis, but it is very rarely encountered in our geographic area and is also less common in adults. These are likely accumulation of inflammatory cells at the limbus due to the upregulation of structural proteins and lipid metabolism proteins brought up by dupilumab, an interleukin 13 inhibitor.17 Another important finding was the inflammatory corneal infiltrates. These were similar to the ones seen in staphylococcal marginal keratitis but were found in our patients without the usually associated blepharitis. These corneal infiltrates were indicative of DAOSD as they would be atypical of other causes of blepharoconjunctivitis, including atopic, allergic perennial or seasonal conjunctivitis. Finally, episcleritis is another finding that has been rarely reported in DAOSD.
Importantly, we have detailed the duration of treatment required in these patients using corticosteroid eyedrops over 2 months for strong corticosteroids and over 11 months for mild corticosteroids. The long duration and significant proportion of patients requiring corticosteroid eyedrops at final follow-up (36%) suggests this is a chronic illness, which requires maintenance treatment to avoid recurrences. Good control of DAOSD remains possible with ocular medication and allows the continuation of dupilumab treatment in patients for whom it is most beneficial. This is increasingly important as research now support long-term use of dupilumab for some patients’ disease management.24
The time to onset of ocular symptoms was often ≥4 months. This delayed timeline for onset of symptoms may be explained by the pharmacokinetic properties of dupilumab, with steady-state concentrations of dupilumab achieved by 16 weeks.1 Recognising the bioavailability profile of dupilumab may assist clinicians in differentiating between adverse ocular effects caused by dupilumab and those caused by AD or other pathologies. Patients’ ocular findings that appear immediately or soon after initiation of dupilumab may be less likely associated with dupilumab given that peak serum concentrations would not have been reached and maintained at steady-state concentrations.25
This differs somewhat from results from Nahum et al, where patients presented with DAOSD as early as 2 weeks following initiation of dupilumab and up to 4 months.21 This could be explained in part by differences in definition of DAOSD. Nahum et al defined DAOSD as an increase in ocular symptoms following start of dupilumab therapy, while we considered a combination of symptoms and findings in the absence of another explanation or diagnosis. Mild cases of dry eyes that could be considered part of the spectrum of DAOSD were also not likely to be referred to our institution given that dermatologists generally empirically treat these patients with artificial tears. Our time to onset of DAOSD resembles the results of Bohner et al with an average of 40 weeks between dupilumab initiation and ophthalmology referral.26 This may also be explained by a similar study framework whereby patients were also referred to ophthalmology by dermatology for management as needed.
Since the reports of conjunctivitis in the initial trials studying dupilumab, a few case series have examined the occurrence of DAOSD, though definitions varied widely.21 26 Also, patients identified with DAOSD did not always undergo an ophthalmological examination to characterise the nature of the ocular manifestations. The largest cohort included 210 patients with AD and examined the onset of DAOSD in general.23 They identified 78 patients as having developed DAOSD, among whom 15 patients were seen in ophthalmology. Other large case series included 10–23 patients and described the clinical manifestations of DAOSD as being predominantly characterised by eyelid dermatitis, blepharitis, limbal inflammation and conjunctivitis.4 7 8 27 28 Popiela et al identified 13 patients assessed in ophthalmology with 9 diagnosed with DAOSD, primarily conjunctivitis, among whom 6 still required topical corticosteroid eyedrops at a mean follow-up of 16 months.29 Similarly to our cohort, treatments for these cases included corticosteroid eyedrops, periocular calcineurin inhibitors, antihistamine eyedrops and artificial tears, with good results but discontinuation of dupilumab was necessary in select patients. The use of preservative-free artificial tears and antihistamine-mast cell stabilisers as initial treatment can be helpful to reduce the need for topical corticosteroid eyedrops if this is sufficient to control symptoms, and their use is recommended as a first-line therapy.21 26 Other smaller case series have reported similar clinical manifestations, treatments and outcomes.30 Rarer findings include corneal ulceration with infiltrates within 3 weeks of dupilumab treatment17 similar to what was seen in this case series, as well as corneal thinning to the point of perforation occurring 3 months and 9 months after start of dupilumab.16 Importantly, collaboration between ophthalmology and dermatology is necessary to establish proper diagnosis and early recognition of DAOSD and to prevent delayed or inappropriate treatments, which could prolong duration of symptoms and cause permanent ocular lesions.
Determination of adverse effect
Unfortunately, a gold standard for the diagnosis of DAOSD has not yet been established; therefore, clinical judgement must be used. In some (21%) patients with DAOSD, there was no significant ocular history, notably of ocular AD involvement. This reinforces the probability that findings were attributable to dupilumab rather than an exacerbation of their previous ocular AD through an immunomodulatory action of dupilumab. Nahum et al instead found that 87.5% of patients with DAOSD had previous atopic keratoconjunctivitis compared with 23.5% of patients without DAOSD (p<0.001),21 while Bohner et al had similar results to ours with only 7% of patients with a history of previous atopic keratoconjunctivitis.26 Bortoluzzi et al also had 28% of their patients with previous atopic keratoconjunctivitis, but importantly performing baseline exams prior to start of dupilumab revealed an important proportion of patients with altered ocular surface.31 This suggests that patients may have worsening of ocular AD symptoms following start of dupilumab treatment, which may explain discrepancies between study conclusions.
Pathophysiological mechanism
Consistent with other reports, conjunctivitis was the most common adverse effect secondary to dupilumab, observed in 18 patients (62%) in our cohort. It occurred in up to 28% of patients in the LIBERTY AD CAFÉ trial combining dupilumab and topical corticosteroids.3 32 It is likely that inflammation and dysfunctional physical barrier functions, including the ocular surface epithelium, are involved in the disease pathway, rendering patients with AD on dupilumab particularly susceptible to these side effects.8 Furthermore, while dupilumab blocks inflammation through interleukin 4 and interleukin 13, it also upregulates interferon–gamma-mediated inflammation, which has previously been implicated in evaporative dry eye disease due to loss of conjunctival goblet cells as well as inflammatory response in mucosal tissues.30 It has been hypothesised that the spectrum of disorders seen with dupilumab treatment for AD, including blepharitis, meibomian gland dysfunction, tear film deficiency and keratitis, may result from paradoxical proinflammatory action in the eyes induced by interferon gamma upregulation by dupilumab, despite abatement of other inflammatory symptoms in AD.8
Limitations
This is a single-centre study, which largely confirmed the presence of DAOSD through the expert opinion of a single cornea specialist with over 30 years of experience and the subjective symptoms of patients. Given the small sample size and the limited data on patients’ dermatological condition, this study is underpowered to detect certain associations between AD and DAOSD, specifically between severity of AD and onset of DAOSD as was previously reported for associated conjunctivitis.9 Likewise, detection of small differences in initial and final PHVA could be limited by sample size. This was also measured as PHVA rather than best-corrected visual acuity given that manifest refractions are not systematically done at our centre, but this is not likely to significantly alter the conclusions of our study given that vision loss is not a clinically significant presentation in DAOSD. Additionally, since this study included only patients treated with dupilumab referred to ophthalmology, this may reduce its external validity and generalisability to other patients treated with dupilumab who may not have presented ocular symptoms yet and those with mild ocular conditions and symptoms, which may have been managed empirically with artificial tears or antihistamine-mast cell stabilisers by their dermatologist or another eyecare professional.
In conclusion, although dupilumab is recognised to be associated with an increased incidence of conjunctivitis, we found that it may also be linked with other unusual ocular findings like limbal nodules, corneal infiltrates and episcleritis as adverse effects. The prevalence and severity of these adverse effects should be recognised by ophthalmologists and referring dermatologists. Many patients required prolonged courses of strong and mild corticosteroid eyedrops supplemented with other agents, such as antihistamine-mast cell stabiliser eyedrops, periocular corticosteroids, periocular calcineurin inhibitors and/or preservative-free artificial tears. Most patients’ ocular condition may be improved with this supportive treatment without having to discontinue dupilumab therapy. The evolution under treatment often appears to follow a chronic course that may require long-term maintenance therapy using topical corticosteroids.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Centre hospitalier universitaire de Québec-Université Laval (2021-5463) who waived individual patient consent. The institutional review board waived the need for individual signed patient consent.
References
Footnotes
Contributors MH, SRQ and EY conceived the work, performed the literature review, interpreted the data and drafted and reviewed the manuscript. MH also performed the data curation and data analysis. MM conceived the work and substantively revised the submitted version. P-AL conceived the work, examined all the included patients, performed the data acquisition, performed the literature review, substantively revised the submitted version, and acts as guarantor for the published work. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MM discloses having received lecture fees from Sanofi Genzyme. P-AL discloses having received lecture fees from Sanofi Genzyme. The authors’ relationships did not influence the elaboration of this study nor were the other entities involved in the study.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.