Article Text

Abstract
Objective To evaluate safety and postoperative visual outcomes of low-energy femtosecond laser-assisted (FLA) anterior capsulotomy in paediatric cataract surgery.
Methods and analysis We report a retrospective single-centre consecutive case series of 51 eyes of 33 paediatric cataract patients with a mean age of 3.22 years (range: 2 months to 13 years) who underwent cataract surgery with FLA anterior capsulotomy, using FEMTO LDV Z8 femtosecond laser (Ziemer Ophthalmic Systems). Anterior laser capsulotomy, phacoaspiration and intraocular lens implantation were performed in all eyes. Both intraoperative and long-term postoperative complications, along with long-term monocular corrected distance visual acuity (CDVA), were assessed during average follow-up period of 32.96 months (range: 13–69 months).
Results In 48 out of 51 eyes, a well-sized and well-located anterior capsulotomy was achieved without intraoperative complications. Anterior capsule tears occurred in three eyes; however, they did not extend posteriorly and the intraocular lens were placed in the bags without any further complications. Posterior capsular opacification developed in 45.10% of eyes (23 out of 51) and was subsequently treated with neodymium:yttrium-aluminum-garnet (Nd:YAG) laser capsulotomy. Mean CDVA at final follow-up was 20/40 (range: 20/63 to 20/32) in unilateral cases younger than 12 months, 20/40 (range: 20/1000 to 20/25) in unilateral cases older than 12 months, 20/66 (range: 20/400 to 20/32) in bilateral cases younger than 12 months and 20/40 (range: 20/200 to 20/20) in bilateral cases older than 12 months.
Conclusions Paediatric cataract surgery with low-energy FLA anterior capsulotomy is a procedure with long-term safety, resulting in significant improvement in CDVA.
- Child health (paediatrics)
- Treatment Surgery
- Vision
- Treatment Lasers
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Femtosecond laser-assisted paediatric cataract surgery has been reported to be successful and safe in small case series.
WHAT THIS STUDY ADDS
The use of a low-energy femtosecond laser to perform laser-assisted anterior capsulotomy during paediatric cataract surgery is safe and efficacious in a large patient cohort.
Visual outcomes after paediatric cataract surgery with femtosecond laser-assisted anterior capsulotomy are in line with the existing literature on conventional manual paediatric cataract surgery.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Based on the results of our study, the widespread use of the femtosecond laser-assisted anterior capsulotomy in paediatric patients can be justified.
Introduction
Cataract surgery is the most common eye surgical procedure treating cataract, a disease with a morbidity that increases with advancing age.1 Paediatric cataracts are rare with an estimated prevalence of 3–4 out of 10 000 children throughout the world.2 3 Due to their early onset and subsequent deprivation amblyopia, paediatric cataracts generally have a significant impact on the affected patients’ normal visual development.4 Early management of paediatric cataracts can have a tremendous impact on the quality of lives of these individuals and their families.
The application of femtosecond laser in adult patients’ cataract surgery has become very popular since its first use in Europe in 2008 and FDA’s clearance in 2010, having proven its strong reliability and safety ever since.5 One of the benefits of the femtosecond laser-assisted cataract surgery (FLACS) is the possibility to create a perfectly positioned, sized and shaped capsulotomy.6
Cataract surgery in children essentially differs from that in adults, due to lens capsule being highly elastic. Therefore, capsulorhexis in children is usually more difficult to perform than in adults with an increased risk of runaway capsulorhexis and capsular tear.7
Although FLACS in paediatric population has been reported to be safe and effective, the use of femtosecond lasers during paediatric cataract surgeries has always been restricted to studies with a very limited number of patients.8–11 For this reason, it is of high scientific and clinical interest to confirm both safety and efficacy of paediatric cataract surgery with FLA anterior capsulotomy in a larger patient cohort.
We describe a consecutive case series of 51 eyes of 33 paediatric patients who underwent cataract surgery with low-energy FLA anterior capsulotomy. To our knowledge, this is one of the largest studies looking at both intraoperative and long-term postoperative complications as well as long-term visual outcomes in paediatric patients undergoing cataract surgery with FLA anterior capsulotomy.
Materials and methods
All paediatric cataract surgeries with FLA anterior capsulotomy were performed using the low-energy FEMTO LDV Z8 femtosecond laser (Ziemer Ophthalmic Systems) at the Kaluga branch of the S. Fyodorov Eye Microsurgery Federal State Institution, Russia, between 2015 and 2018. All interventions were performed off-label as the FEMTO LDV Z8 received European CE approval for use in paediatric cataract surgery in 2020. The study was approved by S. Fyodorov Eye Microsurgery Federal State Institution ethics committee (No. 105.4, 08.04.2021), which waived the requirement for informed consent due to a retrospective nature of the study. All relevant aspects of the Declaration of Helsinki were duly followed. Patients’ legal representatives were duly informed about the nature of the procedure, as well as the associated risks, and were given ample time to provide written consent prior to the surgery.
Out of the 51 eyes, 49 were diagnosed with congenital, 1 with traumatic and 1 with secondary cataracts. The secondary cataract case refers to a patient with a history of previous retinal detachment in the right eye related to congenital myopia, which required a circular episcleral buckling surgery. All surgeries were performed by the same surgeon (IGT). All patients with bilateral cataract had delayed sequential bilateral cataract surgery. In all eyes, anterior capsulotomy was performed with the femtosecond laser system, followed by complete aspiration of the lens and intraocular lens (IOL) implantation. The IOL focal power was calculated using the Sanders-Retzlaff-Kraff theoretic formula,12 taking into consideration future growth of the eye ball. The focal power of the used IOLs ranged from 11 diopters (D) to 40 D.
All patients underwent preoperative and postoperative ophthalmologic examination. In patients under the age of 3–4 years, the ophthalmologic examination was performed under sevoflurane anaesthesia using a face mask. The examination included slit lamp biomicroscopy, indirect ophthalmoscopy with dilated pupils, keratometry, intraocular pressure measurement and A and B ultrasound scanning. Preoperative and postoperative visual assessment included monocular corrected distance visual acuity (CDVA) (measured with age-appropriated testing methods), which was assessed exclusively in children from 3 years on. The presence of any intraoperative and postoperative complications was documented.
Surgical technique
All patients underwent surgery under general sevoflurane air mix anaesthesia with a laryngeal mask. A recommended 11 mm rounded wire blades lid speculum designed to accommodate the suction ring of the laser was inserted (Thorlakson Eye Speculum, Katena) and the patient head was positioned according to the manufacturer’s surgical manual recommendations. The surgical procedure started with a fixation suture of superior rectus muscle. Afterwards, the FEMTO LDV Z8 sterile liquid patient interface was accurately-centred relative to the limbus and fixed to the eye using vacuum. The patient interface was then filled with 5 mL balanced salt solution (BSS), which was followed by docking of the laser handpiece onto the patient interface. Once the docking was complete, anterior segment imaging was performed with the built-in optical coherence tomography. Anatomical landmarks were used for precise laser pattern mapping to perform a well-centred anterior capsulotomy. In 40 cases, the target capsulotomy diameter was 5 mm, while in 11, it was 4.5 mm. Bochum formula was used to account for the capsulotomy enlargement factor, related to high elasticity of lens capsules in paediatric patients.10 The following laser settings were used for the anterior capsulotomy: capsulotomy diameter: 3.4 mm to 4.5 mm; laser power: 75%–90%, depending on the presence and severity of the anterior capsule fibrotic changes (higher power used in more pronounced fibrosis); resection height: 0.7 mm and velocity: 50 mm/s. On completion of the capsulotomy, the vacuum fixation was automatically released and the laser handpiece with the patient interface was disconnected from the patient’s eye. Paracentesis incisions were performed with a 1.2 mm disposable knife at 3 and 9 o’clock; a phenylephrine solution (10%) was introduced into the anterior chamber, and the anterior chamber was filled with an ophthalmic viscosurgical device. The floating edge of the anterior capsule was grasped with capsulorhexis forceps or aspirated using an aspiration tip and removed from the anterior chamber through the paracentesis. The main tunnel sclerocorneal incision was performed with a 2.2 mm knife after separation of the conjunctiva from the limbus. Hydrodissection was performed. Phacoaspiration step was performed with the Centurion Vision System (Alcon) using a standard bimanual technique. In this case series, the femtosecond laser or the ultrasound to ‘soften’ the lens matter prior aspiration, was never used. The remaining lens’ cortical material was gently and meticulously aspirated from the capsular bag. Posterior capsular polishing was then performed. Finally, an intraocular lens (AcrySof IQ or AcrySof Natural, Alcon) was injected through the 2.2 mm incision and accurately centred within the capsular bag. The conjunctival incisions were closed by coagulation at the edge. The surgery ended with a closure of corneal incisions by hydration with BSS and a subconjunctival injection of 0.4 mg of dexamethasone. The standard postoperative topical medication regimen required the use of antibiotic drops 4 times a day for 1 week, cyclopentolate drops 3 times a day for 1 week, dexamethasone drops and diclofenac sodium drops 4 times a day for 1 month.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of the study.
Results
The cataract surgery with FLA anterior capsulotomy was performed in 51 consecutive eyes of 33 paediatric patients. Fifteen of these cases were unilateral and 36 were bilateral. The age at the time of primary surgery ranged from 2 months to 13 years, with a mean of 3.22 years±3.93 (SD) (median age: 1.36 years, IQR: 0.61–3.64 years). Twenty of the reported cases (39.22%) were performed in 13 children younger than 12 months. The mean age of the unilateral cases was 42.09±48.27 months (range: 3–146 months; median age: 16.03 months, IQR: 4.26–76.26 months) and of the bilateral cases, 36.10±44.56 months (range: 2–160 months; median age: 14.77 months, IQR: 7.57–41.83 months). After surgery, patients were followed up for a mean period of 32.96±14.29 months (range: 13–69 months). All patients attended at least two follow-up visits. The mean number of postoperative evaluation sessions was 4.04±1.02 per patient (range: 2–5 sessions).
Table 1 shows baseline characteristics of all operated eyes.
Characteristics of the operated eyes at baseline (N=51)
Intraoperative outcomes
In 48 eyes out of 51 (94.12%), a well-sized and well-located anterior capsulotomy with an optimal diameter, that allowed the capsular bag to completely envelop the IOL optic, was achieved without any kind of intraoperative complications. In most cases, a completely free capsulotomy disc was found immediately after the femtosecond laser procedure and easily removed from the anterior chamber through the paracentesis with a capsulorhexis forceps or aspirated using an aspiration tip. Three eyes (5.88%) had a capsule tear during manual completion of the FLA anterior capsulotomy in cases with residual unidentified tissue bridges. However, the capsular tears did not extend posteriorly and the IOLs were placed and centred in the bag with no further complications.
Postoperative outcomes
An inflammatory reaction with few fibrin strands in the anterior chamber in response to surgical trauma was observed in four eyes 1 day postsurgery. However, in all cases, it resolved spontaneously within 1–2 days. The age at time of surgery of the four patients with an inflammatory reaction was 10 years, 4 years, 7 months and 5 months.
Posterior capsular opacification (PCO) developed in 23 eyes (45.10%) of 17 patients. Mean postoperative time to PCO development was 20.47±9.42 months (range: 4–33 months). The mean age at time of primary surgery of eyes developing PCO was 23.38±26.96 months (range: 2–117 months; median: 10.23 months, IQR: 5.03–39.68 months). Thirteen out of 20 eyes (65.00%) with an age at time of surgery younger than 12 months developed PCO. PCO developed in 46.67% (7 out of 15 cases) of all unilateral cases and in 44.44% (16 out of 36 cases) of all bilateral cases.
PCO obscured the visual axis to an extent that all of the 23 eyes required to undergo neodymium:yttrium-aluminum-garnet (Nd:YAG) laser capsulotomy. The mean time from cataract surgery to the Nd:YAG laser posterior capsulotomy treatment was 32.24±10.92 months (range: 6–48 months).
Ideally round and smooth edges of anterior capsulotomies were maintained throughout the observation period. No IOL rotation, tilting or decentration were observed in any case (figure 1).
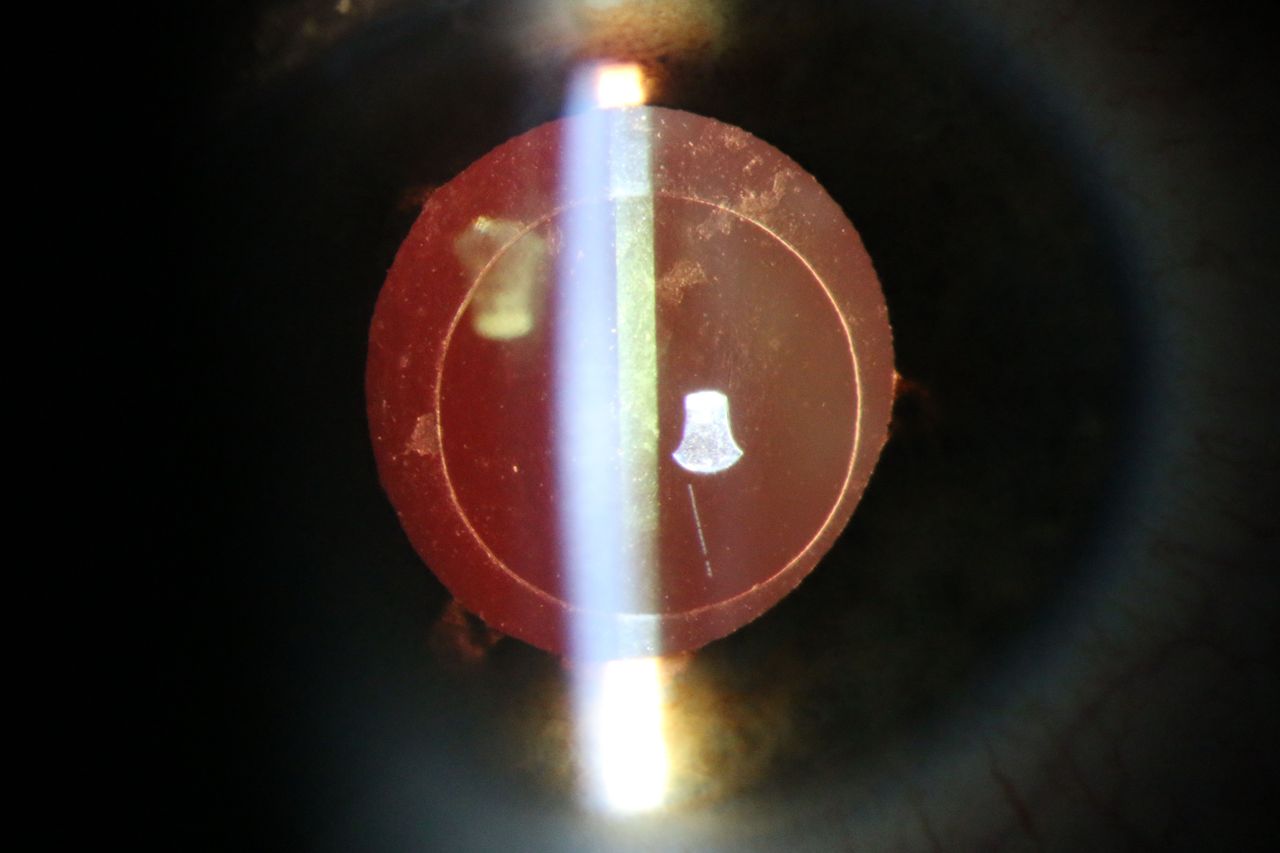
Example of the surgery results, 10 days postoperatively. Surgery performed in a 12-year-old female, who was diagnosed with a traumatic cataract in the right eye.
Visual outcome
Postoperative CDVA was recorded at last patient visit. In 34 eyes of 22 patients (66.67%), preoperative assessment of the visual acuity was not possible due to young age of study participants or because density of the cataract completely obscured the vision. The postoperative assessment of CDVA was possible in 46 eyes of 29 patients (87.88%). Three children without recordable postoperative visual acuity (two unilateral surgeries and one bilateral surgery) were younger than 3 years of age at their last follow-up visit. In addition, in one patient, it was not possible to assess visual acuity in OD (bilateral surgery), despite the child being older than 3 years during the last follow-up visit, due to esotropia (10 degrees), a high degree of congenital myopia and amblyopia. Postoperative CDVA at last patient visit is presented in figure 2. In general, a CDVA equal to or better than 20/40 was attained in 53.85% of all unilateral cases (7 out of 13 cases) and in 42.42% of all bilateral cases (14 out of 33 cases).
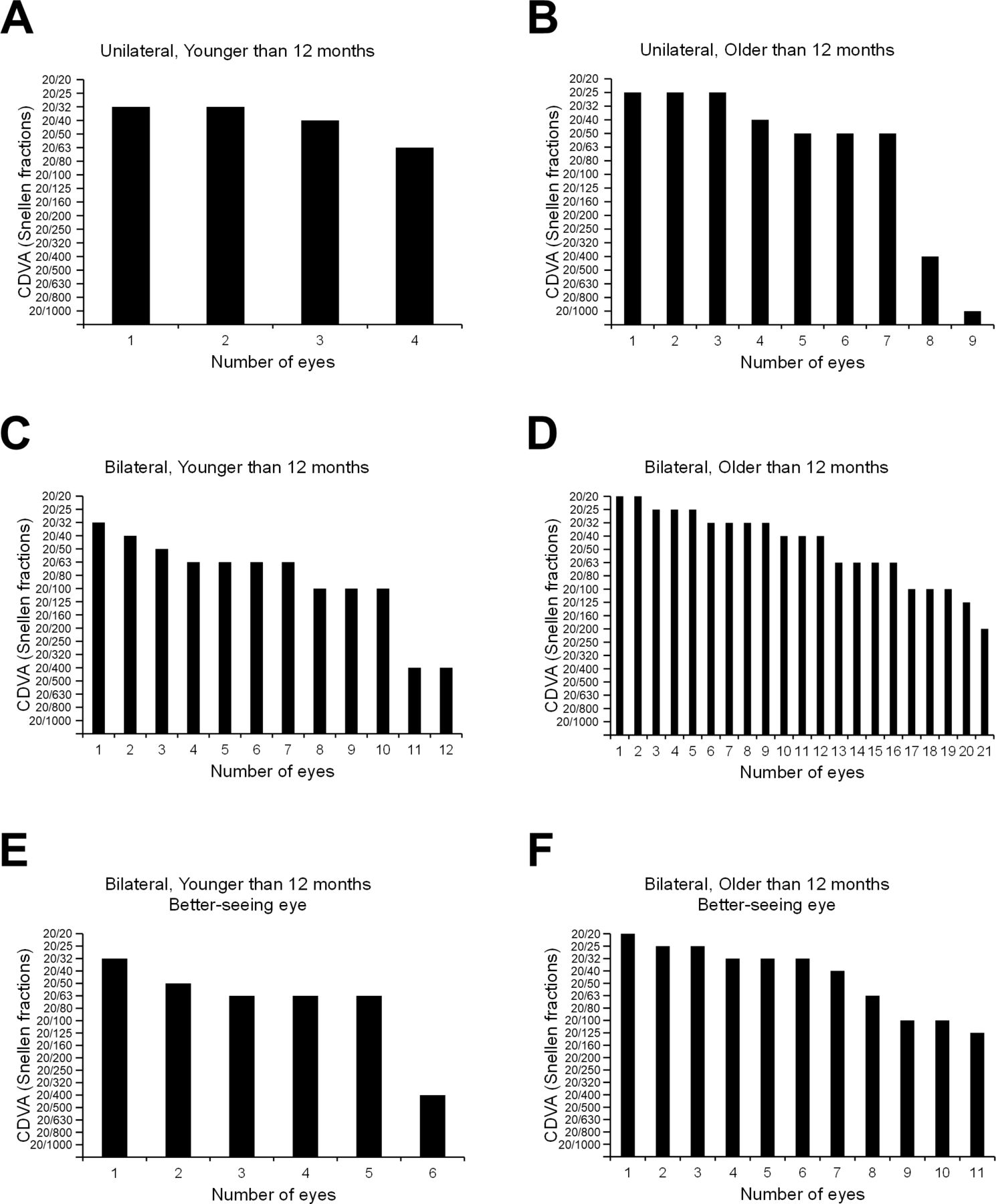
Corrected distance visual acuity (CDVA) results at last patient visit in children who underwent cataract surgery with femtosecond laser-assisted anterior capsulotomy. (A) Unilateral cases younger than 12 months at time of primary surgery (4 out of 46 eyes). (B) Unilateral cases older than 12 months at time of primary surgery (9 out of 46 eyes). (C) Bilateral cases younger than 12 months at time of primary surgery (12 out of 46 eyes). (D) Bilateral cases older than 12 months at time of primary surgery (21 out of 46 eyes). (E) Better-seeing eye of bilateral cases younger than 12 months at time of primary surgery. (F) Better-seeing eye of bilateral cases older than 12 months at time of primary surgery.
In patients younger than 12 months of age at time of surgery, a CDVA equal to or better than 20/40 was achieved in 75.00% (three out of four cases) of unilateral cases and in 16.67% (2 out of 12 cases) of bilateral cases. In patients older than 12 months of age a CDVA equal to or better than 20/40 was achieved in 44.44% (4 out of 9 cases) of unilateral cases and in 57.14% (12 out of 21 cases) of bilateral cases. When analysing the better-seeing eye in bilateral cases, a CDVA equal to or better than 20/40 was observed in 16.67% (one out of six cases) of patients younger than 12 months of age and in 63.64% (7 out of 11 cases) of patients older than 12 months of age.
Table 2 reports mean postoperative CDVA attained by the patients at their final follow-up visit.
Mean postoperative corrected distance visual acuity (CDVA) at last patient visit
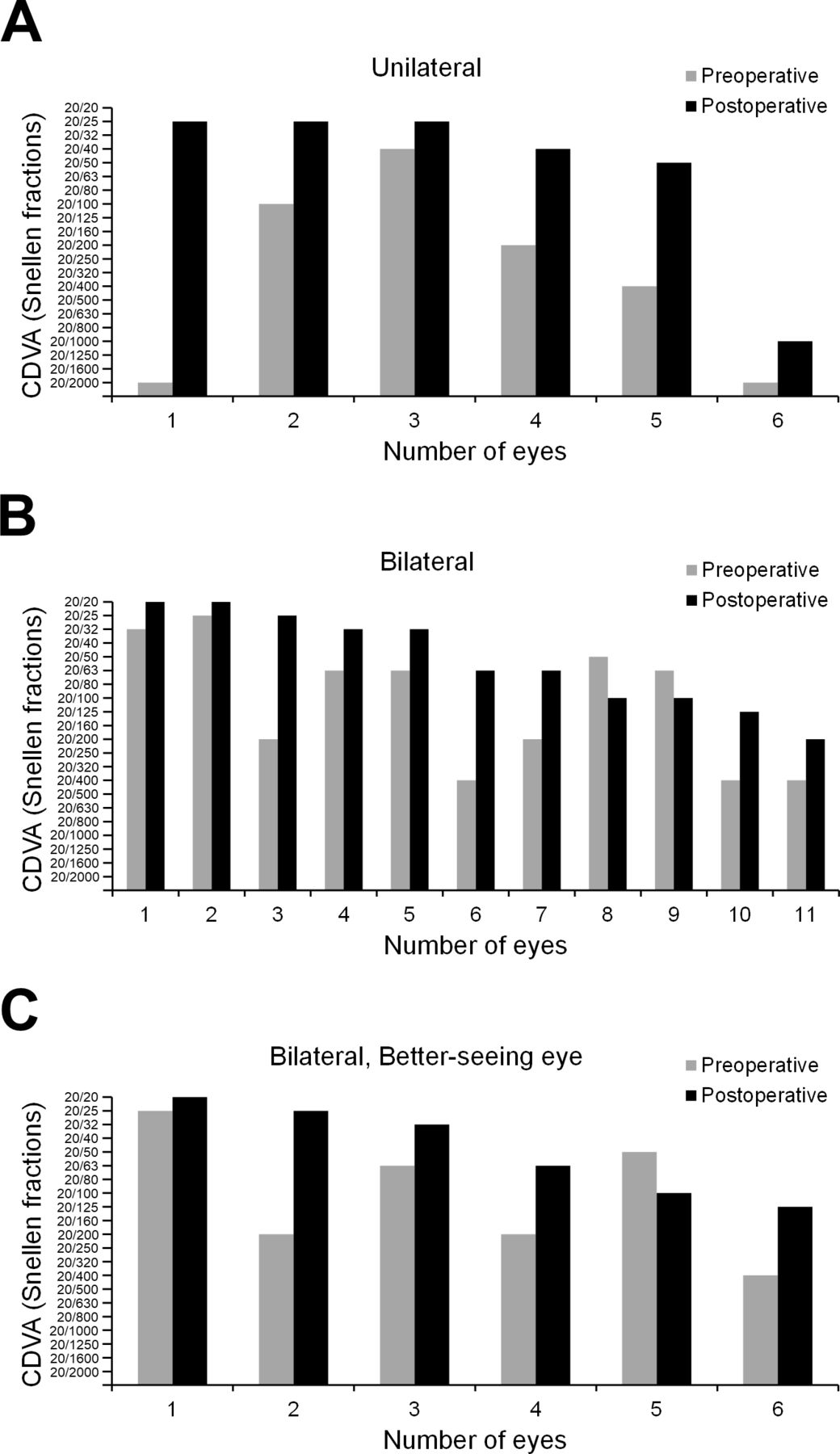
Change in CDVA relative to the preoperative measurement for the 17 eyes, in which it was possible to determine preoperative visual acuity, are presented in figure 3. In six unilateral cases, the mean CDVA improved from 20/200 preoperatively (range: 20/2000 to 20/40) to 20/33 postoperatively (range: 20/1000 to 20/25). In 11 bilateral cases, the mean CDVA improved from 20/66 preoperatively (range: 20/400 to 20/25) to 20/40 postoperatively (range: 20/200 to 20/20). In the six better-seeing eye of the bilateral cases, the mean CDVA improved from 20/66 preoperatively (range: 20/400 to 20/25) to 20/38 postoperatively (range: 20/125 to 20/20). One patient (man, 5 years old) who had bilateral surgery had worse postoperative visual acuity than preoperative one. The CDVA in OD decreased from 20/63 preoperatively to 20/100 postoperatively and in OS from 20/50 preoperatively to 20/100 postoperatively. Prior to surgery, the patient was diagnosed with multiple degenerative eye conditions, including partial optic nerve atrophy in both eyes, chorioretinitis by unknown cause in both eyes, chorioretinal scars in both eyes and macular hypoplasia in OD. Progression of the diseases caused the decrease in patient visual acuity.
{kind=link}
{kind=link}
{kind=link}
Preoperative and postoperative corrected distance visual acuity (CDVA) results at last patient visit in children who underwent cataract surgery with femtosecond laser-assisted anterior capsulotomy and in which it was possible to determine preoperative visual acuity (A) 6 patients who underwent unilateral surgery (B) 11 eyes of 12 patients who underwent bilateral surgery (C) six better-seeing eye of 12 patients who underwent bilateral surgery.
Discussion
One of the most marked differences between adult and paediatric cataract surgery is the behaviour of the lens capsule during the procedure. Paediatric patients have a highly elastic lens capsule and surgeons often find it challenging to perform the capsulorhexis.7 Femtosecond laser can contribute to the achievement of predictable, reproducible, centred and perfectly round-shaped capsulotomy while decreasing the manual surgical steps and manipulations and consequently potentially decrease the risk of surgical complications.6 8 11 The objective of the present study was to analyse safety and efficacy of FLA anterior capsulotomy in a large patient cohort. Visual outcomes following paediatric cataract surgery are strongly correlated with the period of visual deprivation. The decision regarding timing of the surgery is based on the patient’s clinical condition and the presence of visually pronounced cataract. The use of IOLs for the management of infantile cataract remains questionable. This is due to the limited accuracy of IOL power calculation, along with the higher rate of visual axis opacification and increased risks of postoperative complications.13–16 Multiple studies report benefits for visual acuity, if the surgery with IOL implantation is performed at very early age.16–20 In our practice, the surgery is preferably performed in young infants with a significant visual depravation, starting from 8 weeks of age, as in subjects younger than 4 weeks higher risk of postoperative complications have been reported.21–24
The use of low-energy FEMTO LDV Z8 femtosecond laser for the purpose of laser-assisted anterior capsulotomy was investigated in 51 eyes of 33 paediatric patients aged from 2 months to 13 years. Currently, there are only few studies focusing on the use of the femtosecond lasers in children with a limited number of cases performed as off-label procedure and without reports on visual outcomes.8 9 11 25
Intraoperative outcomes
In our study, the incidence rate of capsular tear was 5.88%. Similar incidence rates in paediatric population were reported with common manual anterior capsulotomy techniques. Wilson et al reported an incidence rate of 6.2% with the manual continuous circular curvilinear anterior capsulorhexis and a 5.3% incidence rate with the vitrectorhexis technique.26 In all our cases, the capsule tears occurred during manual completion of the FLA capsulotomy. A large case series study with 1500 FLACS procedures in adult patients reported the intracapsular manipulation in cases with tissue bridges or microtags as the primary cause for anterior capsular tears.27 The laser power parameters have an important role in obtaining a free-floating capsulotomy.8 In this case series, laser power between 75% and 90% was optimal in obtaining an anterior capsulotomy with no residual tissue bridges and very limited amount of cavitation bubbles. Despite the high likelihood of a continuous capsulotomy with a free capsule cap, it is still advisable to make sure that no residual tags exist using adequate detection method, for example, using high magnification when inspecting capsule edge with the microscope, and if necessary, taking proper manual surgical adjustments to ensure completion.
The anterior capsulotomy diameter programmed at the laser platform was calculated using the Bochum formula, which adjusts for age-dependent enlargements of the laser-assisted capsulotomy.10 Recently, a new formula was validated in 2–6-year-old patients with congenital cataract.28 In contrast to Bochum formula, the new one does not take into account patient’s age at time of surgery. Although physical measurements on the achieved capsulotomy diameters were not performed, in all cases, satisfiable results were achieved. Since, for paediatric cataract surgeons, it is vital to be able to use a formula that applies to children of all ages, we are currently performing a study, where laser-assisted anterior and posterior capsulotomies are being assessed in a large cohort of paediatric patients.
It is important to note that in all our cases, no lateral canthotomy was necessary to instal the laser patient interface onto patient’s eye. This avoided all potential long-term sequelae associated with such a procedure in infants.29 In only a limited number of cases (approximately 1 case out of 10 patients based on our routine medical practice), difficulties in the vacuum application of the sterile patient interface due to a very narrow palpebral fissure or a small orbit were observed, and such patients were not included in this study. In such instances, we immediately opted for the manual cataract procedure and, thus, avoided any eyelid lacerations or eyelid bruising. At the time of writing of the manuscript, the manufacturer announced release of a new liquid patient interface specially designed to comply with small orbit and small interpalpebral apertures, which should comply even better with the eyes of infants.
FEMTO LDV Z8 is a compact and mobile femtosecond laser platform. It does not require any major adaption of the surgical room environment, or surgical flow, as there is no need to move the patient to another operating room to perform the laser-assisted step. Despite the fact that we did not measure the overall surgical time of laser-assisted surgeries, we did not perceive any significant difference in total surgery time or general anaesthesia duration if compared with the manual procedure. A prior report on the comparison between FLACS performed with FEMTO LDV Z8 and conventional phacoemulsification cataract surgery (CPCS) in adult patients showed that the mean overall surgical time of FLACS was 5.2 min longer than CPCS.30
In adult patients, low-energy femtosecond lasers have shown better FLACS outcomes (better capsulotomy quality, lower incidence of miosis, lower rate of subconjunctival haemorrhage) than high pulse energy femtosecond lasers did.31 To support this, no cases of intraoperative pupil miosis or subconjunctival haemorrhage were observed in all our paediatric patients.
Postoperative outcomes
In accordance with our outcomes, very similar unilateral and bilateral percentages of postoperative PCO development were reported in studies with similar follow-up periods.32 33
PCO was most frequent in infants younger than 12 months of age, where 65.00% of all cases developed PCO. Multiple studies report same or higher rates of PCO development in very young children after cataract surgery in which the posterior capsules are left intact.34–36 Intraoperative posterior capsulorhexis and anterior vitrectomy are considered standard surgical steps in young children, because they reduce the rate of PCO.37 However, a partial or complete closure of the posterior capsule still occurs in up to 40%–80% of paediatric cases, thereby leading to a decrease in visual axis clarity as well as to decreased visual functions.14 23 38
PCO occurrence may be mitigated by performing of posterior capsulotomies, but due to current lack of clinical evidence on the associated risks of paediatric FLACS with laser-assisted posterior capsulotomy, in this large cohort study, a conservative approach was followed. In fact, FLACS with posterior capsulotomy is a more demanding procedure involving supplementary surgical steps and an additional vacuum-docking of the laser patient interface on the patient’s eye.8 Nevertheless, we believe that in children, FLA posterior capsulotomy may facilitate the surgical step of obtaining a perfectly sized and circular posterior capsulotomy, centric to the anterior capsulotomy. In fact, performing paediatric posterior capsulorhexis manually is challenging as the posterior capsule is very thin, fragile and often hardly visible.39–42 Based on the long-term safety observed in this study, currently we are performing a new study where we perform laser-assisted anterior and posterior capsulotomies during cataract surgery in a large cohort of paediatric patients. This will allow investigating the potential impact of posterior laser-assisted capsulotomy on the development of PCO and the need for subsequent Nd:YAG laser treatment.
Visual outcomes
The present study is the first one to report long-term visual outcomes after paediatric cataract with FLA anterior capsulotomy. So far, all the existing studies pertained to the assessment of feasibility of the surgical procedure.
Overall, our results correlate with the previously reported data on unilateral and bilateral paediatric manual cataract surgery. Nyström et al published their results on phacoemulsification and primary implantation of ‘bag-in-the-lens’ IOL in a series of 109 eyes of 84 children with a median age of 2.5 years (range: 2 weeks to 14.1 years) and reported that 37.5% of unilateral cases and 55.6% of bilateral cases attained a postoperative long-term CDVA of 20/40 or better.43 To better understand the correlation between the preoperative age-specific condition of the eye and postoperative visual outcomes, the results in our study were stratified into two groups, that is, corresponding to patients from 0 to 12 months of age, and those older than 12 months. In general, the visual outcomes of the present study for both age groups are in line with previous findings. In a study by Lesueur et al in 165 eyes of 107 children, a mean CDVA of 0.925 LogMAR (20/168) for unilateral cases in patients younger than 7 months of age and 0.322 LogMAR (20/42) for unilateral cases in patients older than 7 months of age were reported. For bilateral cases in patients younger than 7 months, the mean CDVA was 0.425 LogMAR (20/53) and it was 0.206 LogMAR (20/32) for bilateral cases in patients older than 7 months.17 Lu et al presented the visual results of primary IOL implantation in 16 infants (26 consecutive eyes) aged 6–12 months. At last follow-up the mean CDVA for the unilateral cases was 0.98±0.18 LogMAR (20/191) and 0.50±0.14 LogMAR (20/63) for the bilateral ones.44
In a study by Ram et al, mean CDVA in 10 unilateral cases (range: 8–14 years) was 0.49 LogMAR (20/62) 1 year after non-toric IOL implantation.45
In our study, the mean CDVA in unilateral cases younger than 12 months of age was 20/40. This visual acuity result is generally better than previous literature reports on final unilateral cataract visual outcomes in infants. It is to be noted that we only report on four cases and all the four infants were actually younger than 6 months of age at time of surgery. Looveren et al reported in five children (eight eyes, two unilateral cases, three bilateral cases) younger than 6 months of age a mean CDVA at the end of follow-up of 0.32 decimal (20/63).46
One of the study limitations was that no comparison group (standard manual surgery) was included in the analysis. For this reason, the rates of intraoperative and postoperative complications could not be compared between the two methods performed by the same surgeon. In addition, because of the very young age of the majority of our patients, we encountered difficulty in testing and interpreting children’s visual function. The visual acuity results may be affected, among others, by patients’ attention and time of examination. An additional challenge was the examination of the child’s eye, especially during the assessment of a postoperative complication. In young children and in uncooperative children, all ophthalmologic examinations including anterior segment and Fundus examination were performed under inhalation anaesthesia.
In conclusion, the paediatric cataract surgery with laser-assisted anterior capsulotomy using a mobile and compact low-pulse energy femtosecond laser is safe and reliable. In this paediatric case series, the low-energy femtosecond laser offered the benefits of achieving a safe anterior capsulotomy, low number of intraoperative complications as well as significant improvement in CDVA. Although the data presented in this study were collected prior to the European CE approval, the FEMTO LDV Z8 is today the only femtosecond laser on the market indicated for use in paediatric cataract surgery.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The retrospective study was approved by S. Fyodorov Eye Microsurgery Federal State Institution ethics committee (Number 105.4, 08.04.2021).
Acknowledgments
We would like to express our sincere thanks to the medical team of the Kaluga branch of the S. Fyodorov Eye Microsurgery Federal State Institution, Russia for their remarks, support and encouragement during the study.
References
Footnotes
Contributors IGT made substantial contributions to conception and design, acquisition of data and analysis and interpretation of data, and as such is to be considered as a guarantor for all applicable purposes; AVT, SVI made substantial contributions to acquisition of data, and analysis and interpretation of data. All authors, in addition, were involved in drafting the article and revising it critically for important intellectual content and final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and public were not involved in the sudy.
Provenance and peer review Not commissioned; externally peer reviewed.