Article Text

ABSTRACTPurpose
To describe the ocular features and characteristics of young children presenting with advanced, untreated retinopathy of prematurity and to determine appropriate screening guidelines for retinopathy of prematurity (ROP) in Pakistan.
Material and methods A retrospective case series of young children with stage5A or 5B or cicatricial changes (4B or 4A ROP) was undertaken in the Department of Ophthalmology, Lahore General Hospital, Lahore, Pakistan, from August 2017 to July 2019. Information was obtained from interviewing parents and from neonatal care discharge summaries, if available. An assessment of visual function and a dilated fundus examination were performed.
Results 51 children presented at mean age of 9.7 (1.5–36) months. Their mean gestational age (GA) was 28.84 (26–38) weeks, and mean birth weight (BW) was 1229 (800–2100) g. Four children (7.8%) had a GA of >31 weeks plus a BW of >1501 g. 40 (76.4%) children were blind and 11 (23.6%) had impaired vision. Sixty-five eyes (63.7%) had stage 5B; 13 (12.7%) eyes had stage 5A; 18 (17.6%) had falciform macular folds (4B ROP) and 6 eyes (5.9%) had macular dragging (4A ROP). 39 (76.5%) children had bilateral stage 5A/5B. Half (47%) of the children lived outside the capital city of Lahore, and 15 came from small cities (population <1 million).
Conclusion The third epidemic of blindness due to ROP has arrived in Pakistan, and premature babies are going blind even in smaller cities. Initial screening guidelines of a GA of ≤35 weeks and BW of ≤2000 g seem reasonable. There is an urgent need to improve the quality of neonatal care and to increase the coverage of ROP screening and treatment services across the country.
- retina
- vision
- child health (paediatrics)
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Retinopathy of prematurity (ROP), a vasoproliferative disease of the retina of premature babies, is an avoidable cause of blindness. Evidence-based screening criteria are available for many countries, but not for Pakistan.
WHAT THIS STUDY ADDS
ROP is causing blindness in Pakistan, and is affecting children who were born with a wide range of birth weights and gestational ages. The findings reflect poor quality neonatal care and a lack of effective ROP screening and treatment services.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE, OR POLICY
Our findings provide some support for wider screening criteria for ROP in Pakistan, but more studies are needed. Improvements in the quality of neonatal care and expansion of ROP services are urgently needed.
Introduction
Retinopathy of prematurity (ROP) is a significant cause of avoidable blindness in young children,1 despite the effectiveness of screening and treatment. The third epidemic of ROP blindness, which started in the 1990s in East Europe and Latin America,2 3 has extended into other countries in Asia4 and, more recently, into sub-Saharan Africa.5 The third epidemic is a result of increasing survival of preterm infants due to the expansion of neonatal care services, coupled with inadequate ROP services to detect and treat vision-threatening ROP (VT-ROP). Infant mortality rates (IMR) have been shown to be associated with the proportion of blindness in children due to ROP, and countries with an IMR of 10–60/1000 live births are those most at risk of ROP blindness.2 In 2018, the IMR in Pakistan was 57.2/1000 live births, suggesting that blindness due to ROP is likely to become a problem.6
Preventing blindness from ROP requires high-quality neonatal care starting immediately after birth.7 Screening for vision threatening ROP (VT-ROP, Type1 ROP) is required, starting a few weeks after birth. Treatment, if needed, must be delivered within 48–72 hours to prevent progression to retinal detachment.8 A multidisciplinary approach is essential for successful screening programmes, with excellent collaboration between the ophthalmologist and neonatal teams.9 However, neonatologists are often not aware of the impact of untreated ROP, as blind children with end stage ROP tend to present to ophthalmologists.
Screening guidelines need to take account of the local context, as preterm infants at risk of ROP vary depending on the level of neonatal care they have received.10 In settings with suboptimal neonatal care, more mature, heavier infants are also at risk of VT-ROP than in units where there is less exposure to risk factors such as hyperoxia, sepsis and failure to gain weight. The majority of countries use a combination of gestational age (GA) and birth weight (BW) to identify infants eligible for screening, and some use additional sickness criteria. For example, the USA and UK use the guidelines of GA of less than 30 and 31 weeks, respectively, and a BW of less than 1500 g.11 However, these narrow criteria would miss many infants with VT-ROP in low-income and middle-income countries; hence, the criteria used in India, China and Mexico include older premature babies with higher BWs.12
However, there are few data from Pakistan on which to base recommendations for ROP screening criteria. In two studies, undertaken in state-of-the-art private neonatal intensive care units (NICU), severe ROP developed in infants with a GA of ≤32 weeks and a BW ≤1500 g.13 14 In three other studies, the characteristics of infants developing VT-ROP are not clearly described,15–17 but one study, which used wider criteria, stated that none of the infants who developed VT-ROP fell outside UK screening criteria.18
One way to develop relevant screening guidelines would be to evaluate the GA and BW of infants who become blind from ROP without being screened or treated. This study describes the ocular morbidity and characteristics of children presenting with advanced, untreated ROP in order to provide preliminary information on GA and BW screening criteria in Pakistan.
Material and methods
A retrospective study of all consecutive infants and young children who presented to the ROP clinic at the outpatient department of Lahore General Hospital, over a 24-month period between August 2017 and July 2019 were included. Prematurity was confirmed by neonatal discharge summaries and from information given by parents or care givers. Children who had not undergone ROP screening or treatment for ROP were included.
Children underwent dilated fundus examination by indirect ophthalmoscopy and 20D lens with a sterilised speculum for eye opening under topical anaesthesia with proparacaine. Children having clear media also underwent an EUA (examination under general anaesthesia) to capture retinal photographs using a neonatal retinal camera (Forus, India) and to confirm the extent of retinal detachment with more accuracy. Children with dense retrolental fibroplasia and no view of the fundus did not have EUA or retinal images. However, all children had B-scan ultrasonography (Quantel, Compact Touch, France) to classify stage 5 ROP into 5A and 5B. All findings were confirmed by two vitreoretinal specialists experienced in ROP, and were described in accordance with the International Classification of Retinopathy of Prematurity.19
Visual function was described depending on the ability to show fixation and following.20 Two targets were used, a light target and a toy where the wisest diameter was 10 cm. Children able to fixate on and follow the 10 cm toy target were categorised as having good vision. Children who could fixate on and follow the light were categorised as visually impaired, those who could not respond to the torch light were categorised as blind.
Children with features of advanced ROP on dilated retinal examination, including total retinal detachment, falciform macular folds or macular dragging (ie, stages 4B 5A or B or cicatricial disease)11 were included in the study. Children with retinal detachment not related to ROP for example, from persistent hyperplastic primary vitreous or trauma, were excluded.
The following information was recorded: GA (in completed weeks), BW, place of neonatal care, length of stay, administration of supplemental oxygen and surfactant, blood transfusions and a history of sepsis. Oxygen supplementation was considered positive if given for more than 72 hours. Information regarding whether the parents received any education about ROP or were told about the need for screening in the neonatal unit was collected. How the child was referred (self-referral, referred by an ophthalmologist or a neonatologist) was also recorded.
SPSS Statistics for Windows package, V.25.0 (IBM, USA), was used for data entry and analysis. Variables were characterised as either categorical, such as level of vision, or continuous. Age at presentation, BW and GA were expressed as means with SD. Association between means of continuous variables, such as BW, GA, age at presentation and type of ROP, was analysed using analysis of variance (ANOVA).
Results
Fifty-one young children met the inclusion criteria, 51% of whom were female. The mean chronological age at presentation was 9.7±8.1 (range 1.5–36) months. The mean GA was 28.8±2.2 (range 26–38) weeks and the mean BW was 1200±300 (range 800–2100) g (online supplemental file 1).
Supplemental material
Seven of the 51 children weighed more than 1500 g (13.7%) at birth and 6/51 (11.8%) had a GA of more than 32 completed weeks. A plot of BW against GA shows that one patient (<2%) and four patients (7.8%) would have missed screening if guidelines recommended by the Ophthalmic Society of Pakistan (OSP)21 and the UK11 had been used, respectively (figure 1).
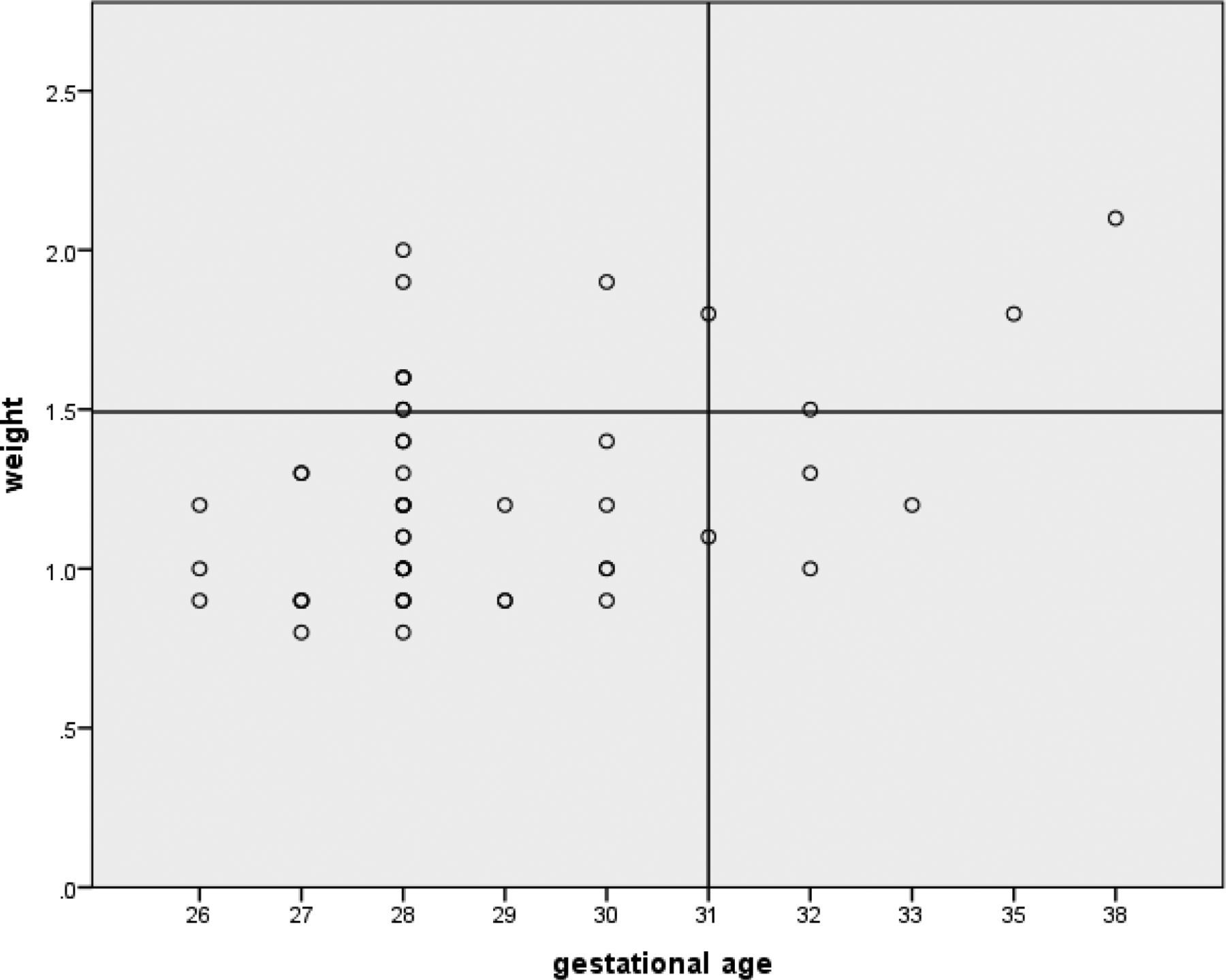
{kind=link}
Birth weight and gestational age of 51 children with advanced ROP. Reference lines show UK ROP screening criteria, 2022.11 Four babies would be missed using UK screening criteria. ROP, retinopathy of prematurity.
Over half (29/51) of the children had been referred by an ophthalmologist, 18 (35.3%) were self-referred and 4 (7.8%) were referred by a neonatologist. Children referred by a neonatologist were significantly younger at presentation (mean 2.5±1.0, range 1.4–5 months) than those referred by an ophthalmologist (9.0±7.0, range 1.5–36 months) or those whose parents self-referred as they had noticed leukocoria or abnormal visual behaviour (mean 12.7±9.4, range 3–30 months)(ANOVA, p=0.05).
Visual function was very poor; 78 eyes (76.5%) were blind and 24 eyes (23.6%) were visually impaired and none had good visual function. The oldest child was 36 months old but as the best visual function was only F&F to light, no other test could be used to assess visual function.The majority of children, 39/51 (76.5%), were blind in both eyes, 9/51 (17.6%) had one blind and one visually impaired eye, and 3 children (5.9%) had visual impairment in both eyes.
Almost two thirds of eyes (65/102) had stage 5B retinal detachment and 13 eyes (12.7%) had stage 5A. Cicatricial ROP, that is, falciform macular folds (4B) or temporal cicatrisation with macular dragging (4A), occurred in 18 (17.6%) and 6 (5.9%) eyes, respectively. Thirty-nine children (76.5%) had a retinal detachment in their better eye: 27/51 (52.9%) had stage 5B and 12/51 (23.5%) had stage 5A (table 1). Nine children (17.6%) had a falciform macular fold in their better eye (the eye with less advanced ROP) and 3/51 (5.9%) had macular dragging. Children with bilateral stage 5A or 5B ROP (Group A) presented at a significantly earlier age than those with cicatricial ROP in the better eye (Group B), at 7.7±6.5 and 16.1±9.7 months, respectively (ANOVA, p=0.001) (table 1). Children with stage 5 (Group A) ROP also had a lower mean BW than those with cicatricial disease (Group B) (ANOVA, p=0.003), but there was no difference in the mean GA by severity of ROP (ANOVA, p=0.27).
Clinical features of ROP in the better eye (the eye with less advanced ROP) and characteristics of affected children
Risk factors
All parents/caregivers confirmed that their infant had received supplemental oxygen for more than 72 hours during their inpatient stay. Other risk factors occurred in a smaller number of children: seven (13.7%) had received blood transfusions, and sepsis was documented in the discharge summary of two (3.9%) children.
Place of neonatal care and information given to parents
Approximately half (52%) of the children had received care in neonatal units in Lahore, the capital of Punjab Province, and all the other children, apart from four, had received care in other cities in Punjab (table 2). Three children came from Karachi, the capital city of Sindh Province, Pakistan and one from Afghanistan.
Population and distance of referring cities
Only 7/51 (13.7%) parents reported that they had been told that prematurity may affect the eyes, but the possibility of blindness was not mentioned. Four parents were told to take their infant to an ophthalmologist for ROP screening, but the level of urgency was not explained. These seven children presented at an earlier age (2.1±0.9 months) than those whose parents did not recall being told anything about ROP (10.9±8.1 months) (ANOVA, p=0.007).
Over 40% of the children came from small cities with a population of less than 10 million, nearly 1/3 (6/21) of whom came from even smaller cities with a population of less than 0.5 million (table 2). There were no significant differences in retinal clinical features by city size or distance from Lahore.
Discussion
Untreated VT-ROP led to very poor outcomes in children in this study, which heralds the arrival of the third epidemic of ROP blindness in Pakistan. In our series, over three quarters of the children were blind in both eyes. It has been estimated that PKR 100 000 (US$625) will be lost every year by each family of an ROP blind child over the child’s lifetime (personal communication, Dr Izhar Hashmi, Director, Punjab Welfare Trust for the Disabled). This is nearly 40% of the average yearly household income in Pakistan. The total life-time losses for our 51 cases would be approximately PKR 306 million (US$1.9 million), a very large amount for a lower-middle income country like Pakistan.
In our study, children with bilateral stage 5A or 5B presented at a younger age than those with cicatricial signs, which is likely to reflect the greater impact on visual functioning of bilateral retinal detachments. Children referred by a neonatologist also presented at a younger age than those referred by an ophthalmologist. Parent’s health seeking behaviour and reasons for delayed presentation were not explored in this study, but late presentation is likely to reflect several factors, such as fear of having their suspicions confirmed, not knowing where to take their child, and the distance and cost of obtaining expert advice in Lahore.
In our study, none of the children had been screened for ROP during infancy. Lack of screening has been reported in several other studies of ROP blind children, such as in India, where the majority (109/115, 94.8%) of children presenting with bilateral stage 5 ROP to one centre over a 1-year period had not been screened (table 3).22 Other studies describing ROP blind children from West India,23 North India24 and Mexico25 also report that the majority of children (65%–100%) had not been screened (table 3). In a study from Pakistan, which included three ROP blind children, none had been screened.26
Characteristics of infants who presented blind from retinopathy of prematurity in low-income and middle-income countries over the last decade
There are three broad reasons why preterm infants might not be screened for ROP. First, the neonatal unit where they received care does not provide ROP services and infants are not referred elsewhere for screening. Second, ROP services are available but the infant falls outside local screening criteria. Last, ROP services are available and the babies fulfil the screening criteria but are not screened or have incomplete screening for a variety of reasons. The first and second reasons are more likely in low-income and middle-income countries such as Pakistan, where coverage of services can be low, and larger more mature infants can develop severe disease. The third reason is more likely in high-income countries, where failure of neonatologists to refer was a contributing factor in 8/13 (61.5%) malpractice law suits in the USA.27 In our study, several parents said they were not informed by the neonatologist of the urgency of a retinal examination, or the urgency was not conveyed or understood. Those counselling the parents of infants who are eligible for screening must emphasise that the examinations must be done in a timely manner, that is, 3–4 weeks after birth for all premature infants, and earlier, at 2–3 weeks, for babies at a high risk of aggressive ROP.24 28
A lack of awareness about ROP was identified among 62 paediatricians and neonatologists surveyed at a national conference in Pakistan in 2014. Only 24% knew that screening was required and most of their institutions (77.4%) did not provide ROP screening.29 Lack of awareness among neonatologists has been reported in other low-income and middle-income countries such as Palestine,30 the Philippines31 and Nigeria.32 This confirms the need to increase awareness about the importance of ROP screening among neonatologists as well as the steps they can take to reduce the risk of VT-ROP by improving the quality of neonatal care.
A large number of studies demonstrate that more mature infants with higher GAs and BWs also develop VT-ROP and become ROP blind in low-income and middle-income settings10 33 34 (table 3). For example, the GA and BWs of 66 ROP blind children in west India ranged from 26 to 36 weeks and from 700 to 2300 g, respectively.23 In a small study in Pakistan, the ROP blind children presented at 6 months of age and had a mean GA of 32 weeks, and their BWs ranged from 1400 to 2000 g (mean 1722)g.26 This is occurring because neonatal care can be suboptimal, and infants are exposed to modifiable risk factors, such as unmonitored supplemental oxygen, sepsis and failure to gain weight. As a consequence, many middle-income countries have wider screening criteria than high-income countries.12 For example, in north India, 15.1% of ROP blind children fell outside the UK screening criteria, that is, they had a GA of more than 32 weeks and a BW of more than 1500 g (table 3).24 In Mexico, the national ROP screening criteria are a BW of ≤1750 g or GA of ≤34 weeks, considerably higher than UK guidelines. In a study of 69 ROP blind Mexican children, 8 infants fell outside these wider criteria.25
Our series shows that applying screening criteria from high-income countries (ie, GA <31 weeks or BW ≤1500 g) would have missed four children (7.8%), while the recent recommendations of the Ophthalmological Society of Pakistan (OSP, December 2019) of ≤35 weeks or ≤2000 g) would have missed only one child (2%). The OSP guidelines seem to be an appropriate starting point for most NICUs in Pakistan, which would need to be confirmed by prospective studies. Consideration could also be given to including sickness criteria for more mature infants, rather than extending the criteria which would greatly increase the screening load.
Lahore is a big city with a several NICUs with neonatologists as well as eye departments with paediatric ophthalmologists. Yet, despite this, nearly half of the ROP blind children came from Lahore. Similar findings were reported from a study in Delhi, the capital city of India, where over 50% of children with advanced ROP, none of whom had been screened, came from within the city.24 In our study, another important finding is that nearly a third of children came from cities with a population of less than half a million. There is an urgent need to improve the quality of neonatal care and to establish ROP screening and treatment services across the country to reduce the anticipated increase in blindness from ROP.
There are many challenges in setting up ROP programmes, including lack of awareness of ROP,32 poor parental compliance with follow-up after discharge from the neonatal unit,35 lack of trained professionals6 36 and the need for a national commitment with financial support for ROP, to name a few.37 The Pakistan ROP Educational and Research Alliance has been successful in setting up screening and treatment services in three government hospitals in Pakistan. Factors associated with success include leadership by neonatologists and paediatricians who work in collaboration with ophthalmologists and neonatal nurses to form a responsible team. Trained ROP coordinators, whose role is to educate parents and to monitor and ensure good compliance with screening in the unit as well as after discharge, are also essential.6
A limitation of our study was that it was based at one centre which is a centre of excellence for ROP. Multicentre studies are needed to study the situation across the country. Another limitation is that the third version of the international classification of ROP (published in 2021) mentions stage 5C ROP, but anterior segment findings could not be retrieved due to the retrospective design of the study.38 Care is also required when interpreting what parents reported because of recall bias.
The hurdles of poor awareness among paediatricians, nurses, administrators, healthcare policy makers and parents need to be overcome, in particular in relation to the narrow window of opportunity for treatment, and that without treated ROP can lead to irreversible blindness. To increase awareness, we plan to send follow-up information to all the NICUs who cared for children in this study to explain the need for setting up ROP screening programmes in their units, as was done in Lima, Peru.39 National guidelines are also needed for the prevention, detection, management and follow-up of ROP, with protocols for screening and treatment.40 Our data support the validity of the initial screening guidelines recommended by OSP (December 2019).21 There is compelling evidence that high-quality ROP services, which require ministry of health support, can reduce the societal burden and lifelong impact of early onset blindness.41
Conclusion
Pakistan is facing the third epidemic of blindness due to ROP, even among infants receiving neonatal care in smaller cities. Initial screening criteria of a GA of ≤35 weeks and a BW of ≤2000 g seem appropriate. There is an urgent need for policies which comply with recent UNICEF and WHO recommendations42 and to establish ROP screening and treatment across the country. Screening in the neonatal unit must become the standard of care because referral to eye departments leads to very high drop-out rates and late presentation.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the institutional review board of Lahore General Hospital and Post-Graduate Medical Institution, Lahore.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MM: planning, conception, design and critical review. LSM: conduct, reporting, acquisition of data, analysis, interpretation of data, manuscript writing. AI: literature review, initial manuscript writing and data acquisition. CG: data interpretation and critical review. UKM: data interpretation and critical review. Guarantor, LSM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.