Article Text

Abstract
Objective To assess the effects of lockdown and unlock phases mandated in view of COVID-19 on the incidence and characteristics of ocular trauma presenting to a tertiary care hospital.
Methods and Analysis The study was carried out as a hospital record based retrospective comparative analysis on patients presenting with ocular trauma in the lockdown period (March–July 2020) compared with the same time frame of the previous year considered as prelockdown period (March–July 2019) and during the unlock phases (August–December 2020).
Results Overall, the casualty department saw 464 patients of ocular trauma in the prelockdown period, 173 in the lockdown and 253 in unlock. The study showed a 44% reduction in patients visiting the casualty department for trauma during the lockdown compared with prelockdown, and a 62% reduction specifically in ocular trauma. The unlock phase showed a 21% reduction in ocular trauma compared with prelockdown and a 41% increase compared with the lockdown. In all three phases, the majority of people affected by ocular trauma were middle aged males from a rural background, sustained by assault. The lockdown saw a decrease in outdoor assaults (45%) and road traffic accidents (22%). Trauma sustained by females (18%) increased in the lockdown, as did home-based assaults (150%) and sexual assaults. The presentation of trauma, especially road traffic accidents and outdoor assaults saw a steady rise during the unlock.
Conclusion The lockdown mandated by the government in response to the COVID-19 pandemic had a significant impact on the trends of trauma presenting to healthcare facilities. There was a decrease in the overall number of patients approaching the casualty during the lockdown. However, during the lockdown, there was an increase in home-based trauma as opposed to outdoor assaults being the primary cause of trauma prior to the lockdown.
- COVID-19
- Trauma
- Epidemiology
- Eye (Globe)
- Public health
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic?
Previous similar studies have shown that the imposition of the lockdown has led to a decrease in patients visiting healthcare centres.
What this study adds?
The current study has shown the demographic distribution of the kinds of patients approaching the casualty for emergency care. Though the total cases of trauma were less, the increase in the fraction of trauma on females and home-based trauma is the significant finding of this study.
How this study might affect research, practice or policy?
The study has brought to light the lacunae in remote medical care. It is evident from the study that the difficulties posed to the public in the lockdown restricted access to medical care and emphasised the importance of strengthening local primary health centres, adequate training of first responders and improving telemedical services.
Introduction
The SARS-CoV-2 caused an outbreak of the COVID-19 pandemic. The virus, being highly contagious spread all over the world in a matter of a few months.1 2 The virus presented with symptoms like fever, cough, sore throat, myalgia, as well as ocular symptoms of viral conjunctivitis.3 The first case was reported in the Wuhan province of China in late 2019 and by March 2020, a global pandemic had been declared.4 India, China, France, Italy, New Zealand, Poland and the UK were the few countries to implement a strict lockdown, shutting down all workplaces, entertainment centres, educational institutes and any kind of travel. Only essential services, like basic food and water supply, healthcare institutes and medical stores, were kept open.
The lockdown in India was announced on 24 March 2020, initially for 21 days, then extended until 31 July (129 days), with a few relaxations.5 A phase-by-phase gradual unlock was brought into effect post August. Such a strict implementation of the lockdown had a significant impact in slowing the rate at which the number of cases were rising, also giving hospitals and the government time to build their infrastructure to handle such an unprecedented patient load.6 People we forced to remain indoors at their homes for an extended period of time. Hospitals had to be equipped to take in COVID-19-infected patients and routine medical care suffered a setback.7 There was a resistance to approach hospitals due to the fear of contracting the disease.5 Restrictions on travel and availability of transport curtailed medical access for majority of the population.
Ocular emergencies are comparatively rare, but they are associated with significant morbidity.8 They warrant immediate examination and management and are associated with poor prognosis if appropriate treatment is delayed.8 Emergency non COVID-19-related services remained open in most hospitals. Therefore, this study was done in the emergency department of a tertiary care hospital to assess the impact that the lockdown had on presenting patients.
Aim
The study aims to assess the effect that the lockdown and unlock had on the number of patients visiting the emergency department due to ocular trauma and to compare the characteristics of the trauma.
Methods
The study was carried out as a retrospective, hospital record based, comparative analysis. The patients included in the study were those who approached the emergency department of our tertiary care hospital with any form of ocular trauma in the lockdown period (March–July 2020) in a similar time frame of the previous year as the prelockdown period (March–July 2019) and during the unlock phase (August–December 2020). Study participants who sustained any ocular trauma and were given outpatient-based treatment, admitted under ophthalmology or admitted under any other specialty but requiring ophthalmological care were all included in the study. Patients with a history of trauma who came for follow-up visits or those with old ocular trauma were excluded from the study. Classification of the injuries and their management was based on the International guidelines lay down by the Birmingham Eye Trauma Terminology System.9 The data were depersonalised, excluding all patient identification information. Data were obtained from the hospital records using the casualty and operation theatre registers. Collected data included the age, sex, laterality, duration of hospital stay, mechanism of trauma, location of trauma, ophthalmological diagnosis and treatment given.
Tertiary care hospitals were handling COVID-19 patients as well as non-COVID emergencies. Routine outpatient department remained open with a small team of doctors, however, routine operative procedures were on hold. Patients presenting to the hospital emergency were attended to by the on-duty ophthalmologist, evaluated and treatment plan decided on. Superficial extra ocular injuries were treated with topical antibiotics, serratiopeptidase, analgesics and suturing was done under due aseptic conditions and local anaesthesia in the procedure room of casualty in the necessary cases. Patients who required surgical management or close observation were admitted under the ophthalmology ward or general surgery ward according the nature of trauma and other interventions required. Sufficient social distancing was followed with respect to admitted patient and patient attenders. The doctors wore prescribed personal protection equipment during the primary patient contact in the casualty as well as in the operation theatre.
Data were entered in Microsoft Excel. Statistical analysis was carried out using SPSS V.20 software. Tables and figures were generated using Microsoft Excel and Microsoft Word. Continuous data were represented as mean and SD and categorical data were represented as count (percentage). P value was calculated using Pearson χ2 or likelihood ratio as appropriate and p<0.05 was considered statistically significant.
Results
The number of patients visiting the casualty for trauma were 12615, 7054 and 9941 in the prelockdown, lockdown and unlock phases respectively. Out of this, 464 (3.6%), 173 (2.4%) and 253 (2.3%) suffered from ocular trauma. The lockdown saw a 44% drop in the incidence of patients visiting the casualty for trauma in general, and a 62% drop in patients with ocular trauma. The unlock phase had a drop of 21% in the numbers compared with the prelockdown and a 41% increase compared with the lockdown.
Demographic data
The age and laterality of the trauma was comparable over the prelockdown, lockdown and unlock phases (p>0.05). The mean age of the study participants was 34±14.2 years in the prelockdown phase, 33.1±13 years is the lockdown and 33±12.2 years in the unlock. Males were seen to be affected more by trauma in all three phases. Majority of the patients were from the rural background in all three time periods, but the numbers increased by 26% during the lockdown and returned to the prelockdown ratio during the unlock. The demographic distribution of data is summarised in the table below (table 1).
Demographic distribution of data
Details of trauma
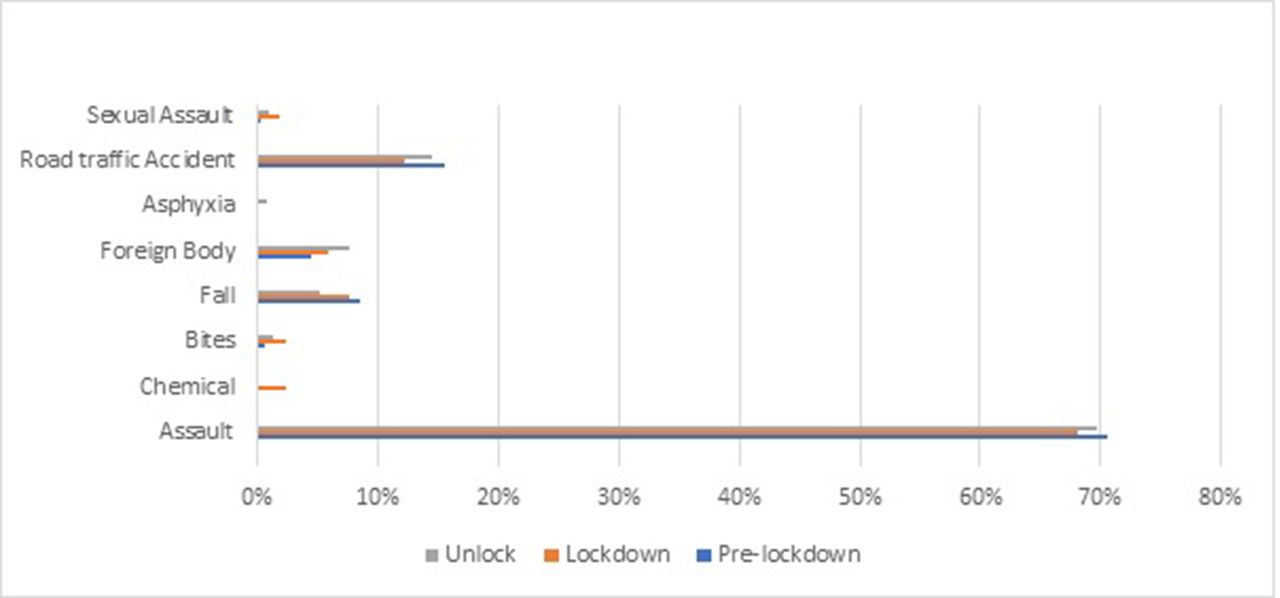
Assault was the most common mechanism of injury seen in all the three periods (70%, 68% and 69%—prelockdown, lockdown and unlock), followed by road traffic accidents (15.6%, 12.2% and 14.5%—prelockdown, lockdown and unlock). Sexual assaults with eye injuries were seen in all three periods, the maximum being in the lockdown (2%). Chemical injuries by irritants or materials available in the household was seen maximally during the lockdown (2.9%) (figure 1).

Mechanism of trauma.
Trauma occurred most commonly outdoor during the prelockdown phase (71.3%). This number reduced during the lockdown and home-based injuries (50%) were seen during the lockdown. The numbers of outdoor trauma increased during the unlock (figure 2). This variation was statistically significant (p<0.01).
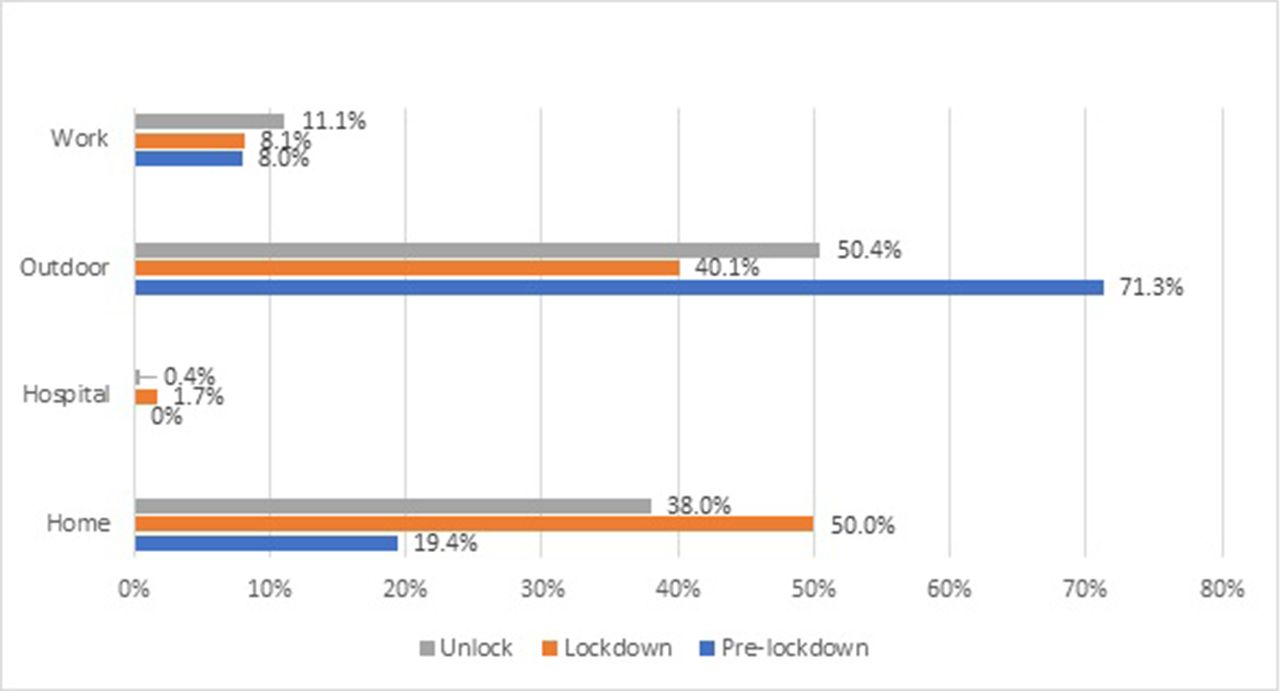
Location of trauma.
Seeing that assault was the most common cause of presenting trauma, a further analysis was done regarding the location of the assault. During the prelockdown phase, 20.7% of the assaults took place indoor at home. During the lockdown, 50.4% of the assaults occurred at home (p<0.01). This trend continued during the unlock phase, when 40.1% of the assaults happened within the house.
In the prelockdown period, 3.9% of the trauma that occurred were under the influence of alcohol. This number reduced to 1.7% during the lockdown and again rose to 3% during the unlock.
Ocular diagnosis
Management
Majority of the patients (89.8% in prelockdown, 91.9% in lockdown and 89.7% in unlock) were managed on out-patient basis, giving necessary treatment in the casualty and calling back for regular follow-up. The mean hospital stay among admitted patients was 5.7±3.7 days, 5.7±3.7 days, 6.1±3.4 days in the prelockdown, lockdown and unlock, respectively (table 2).
Diagnosis and management data
Conservative management was sufficient in maximum number of patients (67.8%, 64.5% and 64.5%—prelockdown, lockdown and unlock). Surgical management was necessary in the remaining. Primary lid tear suturing with antibiotic cover was done in patients with extraocular lid cut lacerated wounds. For intraocular tears, primary wound closure with necessary procedures like foreign body removal, anterior chamber reformation, cataractous lens extraction or vitrectomy was performed as the primary procedure. Failing this, destructive procedures like evisceration or enucleation was carried out. The distribution of treatment received by the patients was comparable (p>0.05) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Management.
Discussion
The COVID-19 pandemic had a massive effect on the world. There was a change in the number and distribution of trauma seen during the pandemic. Patients visiting the outpatient department for routine ophthalmic care at a tertiary care hospital reduced from 9316 in prelockdown to 853 postlockdown. The unlock phase from August to December 2020 showed a rise to 5476, but it was still less than the regular numbers. This may be due to decreased occupational exposure and decreased vehicular traffic, which were few consequences of the lockdown imposed. This hypothesis is supported by the decrease in outdoor ocular trauma during lockdown when compared with prelockdown. Other supporting reasons are peoples’ preference to visit a nearby healthcare facility as there were stricter travel restrictions and there were no public transport facilities. Also, immense fear in people’s minds towards COVID-19 dedicated healthcare facilities (study area was one among them) may be another supporting reason. An important point to note is that many hospitals and clinics remained shut due to the lockdown, reducing the accessibility of healthcare.
A large proportion of patients visiting a tertiary healthcare institute belong to the lower-middle socio-economic class and the class of migrant workers, who migrate to the cities from other states in search of livelihood. They stay away from their homes and families to earn money, and they constitute almost 90% of India’s workforce. The lockdown stranded lakhs of such workers in a place foreign to them and many lost their jobs. After the initial 58-day lockdown, large scale camps were conducted to help such workers return to their homes. This resulted in an egress of almost 43% of the population from urban back to the rural areas.10 This reduction in the urban population could be a factor for the decrease in incidence of ocular trauma during the lockdown period.
With reduction in outdoor activities and traffic on the roads, the trauma occurring outdoors saw a steep decline. When compared with prelockdown levels road traffic accidents decreased by 22% in the lockdown and outdoor assaults decreased by 45.1%. However, there was an increase in home-based assaults by 150% during the lockdown than the prelockdown levels. Suicidal ocular trauma, which was not seen in the prelockdown period was present in the lockdown and unlock phases. An increase in suicidal tendencies during the pandemic has been supported by many other studies,11 12 and the increase seen in the present study could be indicative of the same.
The trauma sustained under the influence of alcohol reduced by 56% during the lockdown and during the unlock, it was comparable to the prelockdown period which may be due to government’s complete ban on sale of alcohol during the lockdown. However, there was an increase in home-based trauma on females, amounting to domestic violence and sexual assaults.13 Sexual assaults increased from 0.2% in prelockdown to 1.7% during the lockdown. The percentage of females involved in trauma increased by 18% in the lockdown. The unlock phase saw a similar trend as seen above but number were higher as compared with lockdown. This may be due to persistent fear towards COVID-19 dedicated healthcare facilities or inadequate monetary resources as a consequence of the unemployment even during the unlock period. This may be due to reflection of mental stress of husbands/other household members onto household women because of unavailability of alcohol to chronic alcoholics, financial strain, the mandate to stay at home and absence of various types of entertainment people used to enjoy in the prelockdown period. This could be a representation of the deterioration of mental well-being in the population. The mental health situation in India was complicated by the high burden of pre-existing mental health issues, stigma associated with getting necessary psychological therapy, a large at-risk population and illiteracy and ignorance coupled with vast false information being portrayed in the media.14
The importance of adding hospital-based trauma in the study was to bring out the assaults against doctors that faced a historic high during the pandemic and lockdown. Violence against doctors is not a new occurrence. However, the increase in hospital-based trauma against doctors has been exemplified in the study. Three doctors who faced assaults in the hospital sustained ocular trauma during the lockdown, which was a small fragment of what was really happening in the world.15
The trends seen in the study are not localised to one area, but have been seen to corroborate with studies carried out in other parts of the country and the world. A thorough review of literature showed few similar studies done in India and other parts of the world. An Indian study carried out in Chhattisgarh, India, published results that corroborated the findings of the present study.16 68.6% of the presenting patients were from a rural background and home-based injuries (78.8%) were the predominant cases. A similar study carried out in the USA showed that the patients also had delayed presentation to the hospital owing to financial and transport difficulties.17 A study in Italy showed a decrease in child and adolescent trauma, which could be due to the closure of schools and a reduction in children playing outdoors.18
The above findings are in contrast with a study carried out in the UK showing that ocular trauma during the lockdown increased by almost three times compared with the prelockdown average. Injuries sustained due to falls and home improvement projects were a major cause for this increase.19
The drastic changes that were seen in the society due to the lockdown threw light on various lacunae in the healthcare service delivery that were required to be filled. The need to improve the literacy rate so that people can understand and opinionate themselves on the happenings in the world, is of utmost importance. The biggest challenges that were faced was the weakness of the peripheral healthcare system, lack of transport facilities, financial strain and stressors worsening the psychological well-being. Strengthening the healthcare system, both hospital-based, remote mobile vehicle based and telemedicine is an aspect that needs attention. Healthcare can be made more accessible to people by establishing more and strengthening the existing mobile units. This can help ensure a better distribution of essentials and basic drugs. Telecommunication has improved leaps and bounds in the last few years and advantage has to be taken to provide medical and psychological support to remote areas, seeing that the majority of patients of trauma were from rural backgrounds.
The limitation to the study was that it was conducted based on the hospital records. Also, the study was based in a single tertiary care hospital which could have caused sampling bias.
Conclusion
The COVID-19-induced pandemic resulted in a decrease in the ocular trauma presenting to hospitals. The incidence of domestic violence, sexual assaults and violence against females increased during the lockdown. Measures need to be taken to improve the accessibility of healthcare services, especially during testing times like lockdowns and other restrictions. Such studies are important and will help us in treatment protocols in future emergencies.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Institutional ethical clearance was obtained before commencement of the study.
Acknowledgments
I would like to acknowledge the immense support extended by the Head of Department, Dr Sanjeevani Ambekar, without which taking up this project would not have been possible. I would also like to thank the Medical Superintendent Dr Ajay Tawre and the forensic medicine department for their help. I would also like to recognise the cooperation of Mr Shailesh Chavan from the medico-legal record department for his support in accessing patient records.
Footnotes
Contributors The manuscript has been read and approved by all the authors. The requirements for authorship as stated earlier in this document have been met and each author believes that the manuscript represents honest work. The guarantor (R.P) accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views expressed in the submitted article are my own and not an official position of the institution or funder.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.