Article Text

Abstract
Objective To compare the two surgical techniques in terms of efficacy, safety, and postoperative management over 36 months of follow-up.
Methods This retrospective clinical cohort study compared the outcome of trabeculectomy surgery and Xen gel implant in patients having uncontrolled glaucoma. Patients were recruited using the following inclusion criteria: uncontrolled intraocular pressure (IOP) on maximally tolerated medical therapy, healthy conjunctiva freely mobile in the superior sector, open-angle, glaucomatous visual field damage, full follow upfollow-up of at least 36 months. Thirty-four patients were submitted to trabeculectomy and 34 to Xen gel implant. We set the lower limit at 6mmHg mm Hg and the upper limit ≤12 mm Hg for criteria A, upper limit to ≤15 mm Hg for criteria B and upper limit ≤18 mm Hg for criteria C. Criteria for success have been characterizedcharacterised according to whether or not this has been achieved without (complete success) or with IOP -lowering medications (qualified success).
Results For all survival curves, trabeculectomy was superior to Xen gel implant. When considering complete success, the log-rank test for criteria A was statistically significant (pp=0.006), marginally significant for criteria B (pp=0.065) and not significant for criteria C (pp=0.23). When qualified success was considered, trabeculectomy was superior to Xen gel for criteria A, B, and C (pp=0.012, pp=0.033 and pp=0.025, respectively). Higher number of post-operative flat chamber and bleb leakage was observed in the trabeculectomy group.
Conclusion Xen gel implant techniques offer a better safety profile but a lower IOP reduction compared to compared with the gold -standard technique.
- glaucoma
- treatment surgery
- intraocular pressure
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Trabeculectomy is the most widely performed surgical treatment of glaucoma with evidence of high long-term success. Previous retrospective studies have compared the efficacy and the safety profile of Xen gel implant with trabeculectomy but over a median follow-up between 6 months and 15 months.
What are the new findings?
Xen gel implant offers a better safety profile, it is surgically faster, but it has a lower IOP reduction compared with the trabeculectomy.
How might these results change the focus of research or clinical practice?
Ophthalmologists have to know that both surgeries can reduce significantly IOP, but if the target IOP is lower teens, trabeculectomy is better, on the other hand, if a faster and safetier surgery is looked for, Xen gel implant is the choice.
INTRODUCTION
Glaucoma is an optic neuropathy that leads to the progressive loss of ganglion cells, defects in the visual field and ultimately to blindness if not adequately managed.1 The prevalence of glaucoma for the population aged 40–80 years is 3.5%, and the burden of glaucoma has been estimated to grow progressively, reaching 111.8 million people affected in 2040 worldwide.2
Elevated intraocular pressure (IOP) is the major risk factor for glaucoma progression, and IOP prevents visual field deterioration.3 The treatment goal for glaucoma is lowering IOP to slow down the damage progression rate to maintain vision-related quality of life according to the patient’s life expectancy.4 Filtering surgery is generally offered to patients in which the target IOP cannot be achieved with medications or laser.5
Currently, trabeculectomy is the most widely performed surgical treatment of glaucoma with evidence of high long-term success.6 Unfortunately, trabeculectomy is associated with severe perioperative complications such as anterior chamber bleeding, conjunctival buttonhole, flat anterior chamber, hypotony, choroidal detachment, hyphaema, cataract, bleb leaking and encapsulated bleb.7–9 To overcome these limitations, minimally invasive and less invasive glaucoma have been developed, aiming at better safety and more predictable results.10
Among them, the gel stent has been designed to be implanted by a clear corneal incision permitting subconjunctival filtration and minimising operating time, avoiding conjunctival incisions and reducing the risk of hypotony.11 Previous retrospective studies have compared the efficacy and the safety profile of gel stent with trabeculectomy over a median follow-up between 6-month and 15-month follow-up.12–16 Our study aimed to compare the two surgical techniques in terms of efficacy, safety and postoperative management over a 36-month follow-up.
Methods
Study design
This retrospective clinical study compared the outcome of trabeculectomy surgery and gel stent implant in patients having uncontrolled glaucoma. The study was carried out at the Clinica Oculistica, DiNOGMI, Ospedale Policlinico San Martino, University of Genoa, Italy, between March 2016 and September 2020. All patients provided written informed consent. Eyes that underwent gel stent implantation were included in the analysis according to the following criteria. The trabeculectomy group was formed to match the ocular and demographic characteristic of the gel stent group.
Inclusion criteria and exclusion criteria
Patients older than 45 years of age with uncontrolled IOP and affected by primary open-angle glaucoma or pseudoexfoliative glaucoma with a complete follow-up of at least 36 months were included. Patients who underwent previous ocular surgeries were excluded except for laser trabeculoplasty or phacoemulsification with IOL implantation performed more than 6 months before the filtration surgery. One eye per patient was included in the analysis.
Study population
According to the inclusion and exclusion criteria, data of 34 patients that underwent gel stent implantation were analysed. A similar group of patients who underwent trabeculectomy matched for ocular and demographic characteristics was formed.
Success and failure criteria
According to the World Glaucoma Association guidelines on design and reporting surgical trials, we considered three complete success criteria according to IOP. We set the lower limit at 6 mm Hg and the upper limit 12 mm Hg for criterion A (6 mm Hg ≤IOP ≤ 12 mm Hg), between 6 mm Hg and 15 mm Hg for criterion B and between 6 mm Hg and 18 mm Hg for criterion C. Criteria for success have been characterised according to whether or not this has been achieved without (complete success) or with IOP-lowering medications (qualified success).
We defined failure as an IOP level measured above the upper limit or below the lower limit on two consecutive study visits. Reintroduction of IOP-lowering medications or additional glaucoma procedures were judged failures. We considered a complete failure in the presence of loss of light perception attributable to glaucoma, or the necessity for further glaucoma surgical intervention, ocular hypotensive medications. Postoperative surgical manouvers, such as flap suture lysis, or Nd:YAG laser procedures, bleb needling and subconjunctival mitomycin-C (MMC) injections, were recorded but not been considered as failure.
We reported the number of IOP-lowering medications before and after surgery according to the number of active compounds (ie, fixed combinations were considered as two medications in the analysis).
Surgical technique
Two experienced surgeons (CET and MI) performed surgeries achieved the same proportion of both surgeries included in the analysis.
Gel sten implant
Topical or peribulbar anaesthesia was achieved before surgery. The nasal upper quadrant of the conjunctiva was marked with 3 mm from the limbus. Subconjunctival injection of 0.12 mL of MMC (0.2 mg/mL) was done by a 30G hypodermic needle in the targeted area. Two self-sealing incisions were fashioned through inferotemporal clear cornea opposite to the preferred position of the implant and nasally. Miochol-E 0.2 mL (1% acetylcholine chloride intraocular solution) was injected into the anterior chamber to obtain miosis. Then, the anterior chamber was filled with cohesive viscoelastic (Viscotek). The preloaded injector needle was inserted in the anterior chamber and then in the nasal upper quadrant of the conjunctiva through the iridocorneal angle, and the gel stent implant was implanted. Injection of a balanced saline solution in an anterior chamber is performed to wash out the viscoelastic and achieve bleb expansion. If needed, the implant is carefully manipulated ab externo to ensure that the implant is freely mobile under the conjunctiva and is not blocked by tenon capsule.
Trabeculectomy
Trabeculectomy surgery was conducted under peribulbar anaesthesia. Conjunctiva and tenon tissue were carefully dissected to create a fornix-based flap. Diathermy on the exposed sclera was applied. Then, a 3×4 mm half-thickness rectangular scleral flap was fashioned. MMC 0.2 mg/mL was applied for 2 min below and over the scleral flap and then washed carefully. An inferotemporal paracentesis was performed before the sclerectomy and the peripheral iridectomy. The scleral flap was then repositioned and sutured with nylon 10–0 sutures. Before closing the conjunctive to the limbus with vycril 8-o sutures, the filtration through the scleral flap was verified. BSS was injected to check the expansion of the filtering bleb.
Postoperative management
IOP-lowering medications were stopped the day of surgery, and tobramycin/dexamethasone was prescribed five times/day for 2 weeks. Then, the topical steroid was tapered down slowly over 6 months.
Bleb management, such as needling procedure or MMC injection, was performed in the outpatient clinic at the slit lamp under topical anaesthesia and iodopovidone administration.
The needling procedure was performed with a 30 G hypodermic needle to dissect subconjunctival scarring, while MMC (0.2 mg/mL) injection was performed approximately 2–3 mm superiorly to the bleb with 30G hypodermic needle.
According to IOP values and the bleb status, both needling and MMC injection were performed at the surgeon’s discretion.
After the baseline visit, follow-up visits were generally scheduled at day 1, day 3, weeks 1 and 2, months 1 and 3 and every 3 months up to the last follow-up visit. According to the clinical evidence, additional visits were conducted at any time at the treating physician’s discretion.
At each follow-up visits, IOP, best-corrected visual acuity, filtering bleb status, anterior chamber status, number of IOP-lowering drug molecules, surgical procedures or laser needed were recorded.
Statistical analysis
In the descriptive statistics, all the variables were reported as mean and SD. The absolute value and frequency were used for the categorical variables. The difference between the two groups was tested by using the Wilcoxon test for continuous data and the chi-squared (χ2) test for the categorical variables. The Kaplan-Meier curves have been used to compare the survival analysis defined by the criteria A, B, C for the two surgical techniques. P-value <0.05 has been considered statistically significant. Statistical analysis was performed with Stata V.15.1 (StataCorp LLC, College Station, Texas).
Results
Our study population consisted of 68 patients of whom 34 eyes underwent trabeculectomy and 34 eyes underwent gel stent implant. The demographical and ocular characteristics of the two groups are summarised in table 1. The study population resulted to be homogeneous regarding the mean age, gender, baseline IOP, number of IOP-lowering medications at the baseline, glaucoma type, mean defect expressed as visual field mean deviation. A marginally significant difference existed regarding the lens status. Eyes that underwent trabeculectomy had more frequently a phakic status of the lens compared with eyes submitted to gel stent implantation (p=0.051).
Baseline characteristics
We summarised in table 2 the surgical anaesthesia, the surgical time and the hospitalisation days for both procedures (p<0.001). All the trabeculectomies were performed under peribulbar anaesthesia, while for 53% of gel stent implants, topical anaesthesia was preferred. As expected, surgical time for trabeculectomies was more that two times the surgical time for gel stent. Also the number of hospitalisation days after surgery resulted higher for trabeculectomy.
Anaesthesia, surgical time, hospitalisation days
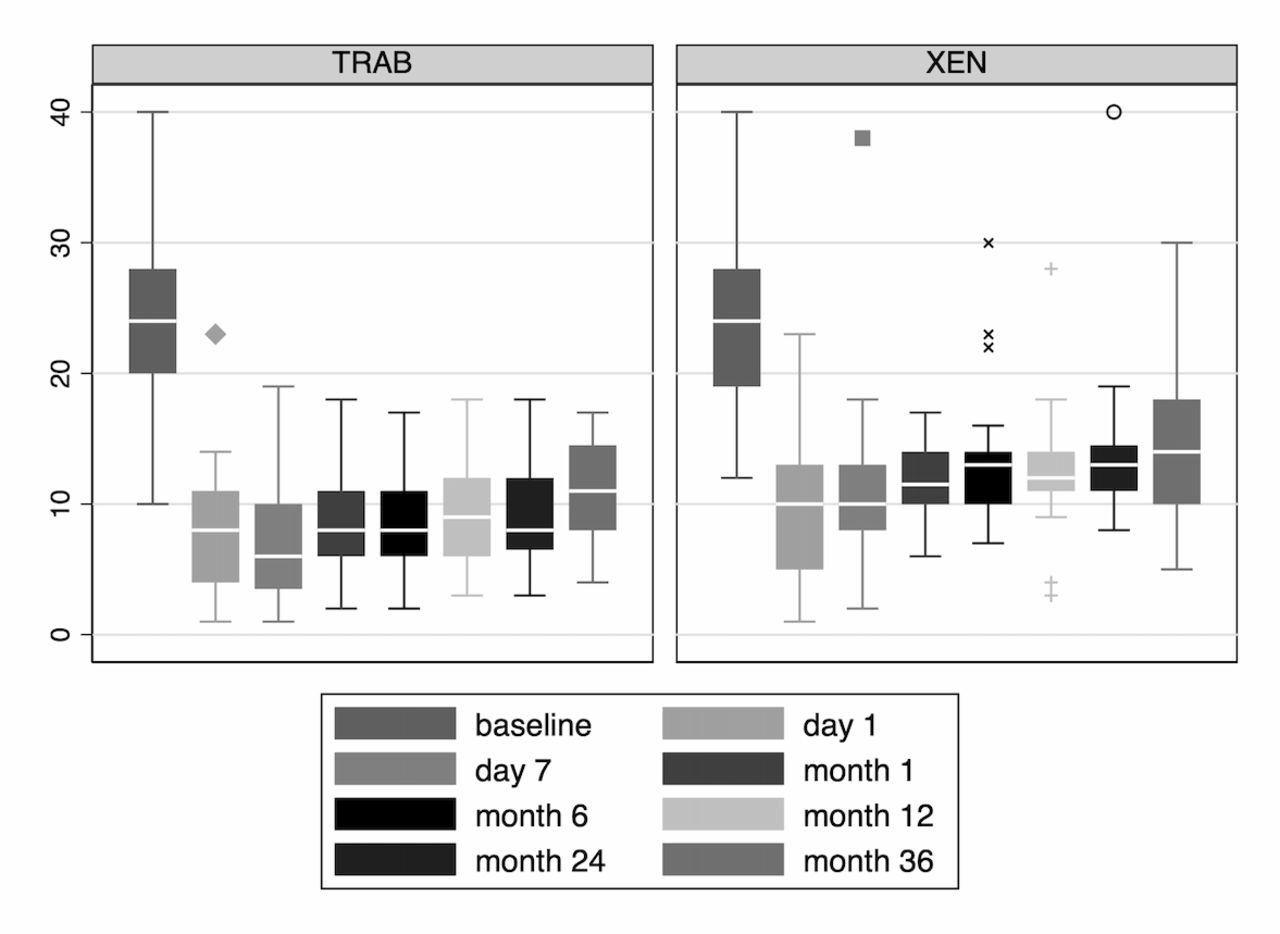
Regarding the postoperative management of the two groups, we analysed the number of postoperative visits, and we found an slightly higher number of visits performed to patients who undergone gel stent at 24 months (p=0.055). Figure 1 represents the IOP analysis performed at 36 months after surgery. The IOP of patients who underwent trabeculectomy showed lower values and a better IOP profile compared with the gel stent group.

{kind=link}
IOP distribution over 36 months for TRAB group and Xen group. IOP, intraocular pressure; TRAB, trabeculectomy.
Concerning the safety profile, all complications were recorded and are summarised in table 3. Table 4 reports the number of visits in our centre’s follow-up period, the number of surgical adjustments such as needling, MMC injections, suture lysis and Nd-YAG laser procedures needed, and additional surgery such as bleb revision and trabeculectomy for each group.
Complications in the gel stent group and trabeculectomy group
Postoperative management* possibility of multiple procedure for each patient
Only the trabeculectomy group underwent suture lysis because of the trabeculectomy surgery’s intrinsic features that require sutures, whereas Nd-Yag laser aimed to restore patency of the implant that was performed only in case of the gel stent. The number of needling and MMC are reported in table 4, and there is no difference between the two groups. Additional surgeries such as bleb revision or trabeculectomy were 2.9% and 20% in the gel stent group; 5.88% of the trabeculectomy group underwent bleb revision. In table 3, complications are reported. The statistical analysis of Kaplan Meier curves was tested with the log-rank test for criteria A, resulted in statistically different (p=0.006), marginally significant for criteria B (p=0.065) and not significant for criteria C (p=0.23) (online supplemental figures 1–3). When qualified success was considered, trabeculectomy was statistically superior to Xen gel for all criteria (A, p=0.012; B, p=0.033 and C, p=0.025) (online supplemental figures 4–6).
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Discussion
Our analysis conducted clinical comparisons of results over a 3-year follow-up for eyes that underwent gel stent implantation or trabeculectomy. The demographical characteristics and baseline ocular characteristics were similar for the two groups, permitting reasonable analysis of the surgical procedure itself. Previously, other retrospective comparisons between gel stent and trabeculectomy have been reported,12–16 but with a shorter follow-up.
During the follow-up, we found a significant better survival curve for trabeculectomy when an IOP criterion between 6 mm Hg and 12 mm Hg without any IOP-lowering medication, additional surgical procedure or sight-threatening complication was set.
Schlenker et al performed a retrospective study involving four centres that followed a total of 185 eyes submitted to gel stent and 169 eyes that underwent trabeculectomy for a median follow-up period of 15.0 and 17.8, respectively.12 The study failed to detect a significant difference in the HR of failure for these two procedures. Compared with our study, Schlenker primary outcome was aimed to an IOP lower than 17 mm Hg without any glaucoma medication, reoperation or serious complication. When we considered a similar IOP criterion (criterion C), we obtained similar results and no difference between groups.
Marcos Parra et al also found no difference between gel stent and trabeculectomy when the success criterian was an IOP ≥6 and ≤16 mm without treatment at 12 months.13 In a real-world analysis of 171 eyes, Wagner et al found similar success at 12 months between gel stent and trabeculectomy. In the latter study, success was defined as IOP ≤18 mm Hg, an IOP reduction of >20% and in no need of revision surgery or topical medication. Even if success was similar, Wagner et al found an higher IOP reduction in the trabeculectomy group (10.5 mm Hg) compared with the Xen group (7.2 mm Hg; p=0.003).14 Another comparison between the two procedure was recently reported. In their analysis, Sharpe et al found a better IOP profile for trabeculectomy at 6 months with a lower number of needling procedures 30% in Xen versus 7.9% in the trab group (p<0.001).15
The observation of significantly longer surgical time for trabeculectomy is due to the higher number of surgical steps involved in the trabeculectomy procedure compared with the gel stent implantation. Longer hospitalisation for the trabeculectomy group might be due to the higher rate of early complications, as reported in table 3. Mathus et al, when comparing the two procedures, found a higher number of complications after trabeculectomy (p = 0.005) and a higher number of needling procedures after gel stent implantation (p = 0.021).16
In our study, whereas bleb leaking and flat anterior chamber were more frequently observed in the trabeculectomy group, choroidal detachment was observed with higher frequency in the gel stent group. The assessment of factors associated with the occurrence of this complication was reported in a previous study.17
In the postoperative management analysis (table 4), the number of postoperative visits showed a marginally significant difference between the two groups. The trabeculectomy group showed fewer postoperative visits over 24 months period, while the difference between the two groups lost significance at 12 months. This evidence can be explained by the higher IOP stability guaranteed by the trabeculectomy technique and the following need for fewer check-up visits on the long-term follow-up. This hypothesis can be supported by the IOP profile over 36 months and shown in figure 1, which shows lower IOP values and less fluctuation in the trabeculectomy group compared with the gel stent group. Suture lysis, a postoperative manouver peculiar of trabeculectomy, was done in 44.1% of patients, and our finding was similar in frequency to the values reported by the Schlenker study.12 Our study is mainly limited by the retrospective design of the study. Even if trabeculectomy and Xen have similar selection criteria, surgeons may choice the procedure based on the patient’s characteristics or target IOP. For this reason, our study is potentially limited by a selection bias. However, this study has the most extended follow-up among the published reports between gel stent and trabeculectomy in a real clinical practice.
In conclusion, the survival analysis study curves highlight that the trabeculectomy offers a higher probability of maintaining lower IOP values at 3 years than the Xen gel implant and should be the surgery of choice when the individual target IOP is low.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This was a clinical retrospective study and it was approved by the regional ethics committee (CER Liguria: 145/2021). All methods used were carried out according to the criteria set by the declaration of Helsinki and by EGS guidelines for the clinical practice useful for following up patients with glaucoma.
Acknowledgments
This work was developed within the framework of the DINOGMI Department of Excellence of MIUR 2018-2022 (Law 232 of 2016). This work was supported by grant from Italian Ministry of Health—ACC.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors FC and MI conceived the study; CET and MI performed the surgery; FC, CAC, SO, VT, DS, CP and SC collected the data and patients; CAC analysed the data; FC, CAC, DS and MI wrote the manuscript; all the authors revised and approved the final version of the manuscript. MI planned the review, is responsible for the overall content and submitted the review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.