Article Text

Abstract
Objective To evaluate the long-term visual outcome and safety after bilateral cataract surgery with primary intraocular lens (IOL) implantation in infants with visually significant cataract at birth operated before 12 weeks of age.
Methods and analysis Medical records of infants with congenital cataract who had bilateral surgery with primary IOL implantation before 12 weeks of age at Oslo University Hospital between 2007 and 2016 were retrospectively reviewed. Fifteen infants (30 eyes) were enrolled for a prospective study examination in 2017. Corrected distance visual acuity (CDVA) and intraocular pressure (IOP) were assessed. Visual axis opacification (VAO) was defined as opacification on the anterior or posterior surface of the IOL, capsular phimosis or fibrinous membrane. Secondary glaucoma was evaluated according to international guidelines.
Results Median age at the time of primary surgery was 35 days (range, 15 to 70 days). There were no serious intraoperative complications, and all eyes had the IOL implanted in the capsular bag. After a median follow-up of 6.1 years (range, 1.5 to 10.2 years), the CDVA was 0.5 logMAR (range, 1.2 to 0.04). All eyes had surgery for VAO and the median number of surgical procedures was 2.0 (range, 1 to 5). The cumulative incidence of secondary glaucoma was 10% after 5 years of follow-up.
Conclusion Primary IOL implantation before 12 weeks of age gave a satisfactory visual outcome, and the incidence of secondary glaucoma was similar to that reported after primary IOL implantation in older infants. However, the risk of VAO was high.
- child health (paediatrics)
- lens and zonules
- vision
- anterior chamber
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Primary intraocular lens (IOL) implantation in children with bilateral cataract up to 2 years of age shows favourable results in terms of visual outcome and safety.
What are the new findings?
Primary IOL implantation before 12 weeks of age gives a satisfactory visual outcome.
The incidence of secondary glaucoma is similar to that reported after primary IOL implantation in older infants.
Primary IOL implantation before 12 weeks of age is associated with a high risk of developing visual axis opacifications.
How might these results change the focus of research or clinical practice?
Primary IOL implantation in this young patient group still poses some challenges. Future research with a larger sample size and preferably randomised, clinical trials that focus exclusively on the youngest patients with visually significant cataract at birth are required.
Introduction
Congenital cataract is one of the most common causes of treatable childhood blindness worldwide.1 The prevalence is estimated from one to four per 10 000 live births.1 2 Globally, approximately 200 000 children are blind from bilateral cataract.2
The timing of cataract extraction is critical to prevent deprivation amblyopia. Most clinicians would recommend surgical intervention before 6 or 8 weeks of age in unilateral and bilateral cataracts, respectively.3 4 Traditionally, it has been controversial to perform primary implantation with an intraocular lens (IOL) before 2 years of age, mainly due to the risk of visual axis opacification (VAO) and secondary glaucoma.5 Furthermore, the unpredictable myopic shift in infants leads to variability in the refractive outcomes.6 Over the last few years, however, primary IOL implantation has become an established treatment modality in some centres even among the youngest children.7 Other leading paediatric surgeons and centres still question this practice, especially in bilateral cataract surgery, where the risk of aniseikonia is lower, and visual outcome sometimes is considered better when both eyes are left aphakic.5 8
Currently, there are several studies addressing the role of primary IOL implantation in paediatric cataract surgery.5 7 9 However, these studies have included patients with age at surgery up to 6–24 months,5 7 9 10 hence, the included cases have probably been a mixture of infants having visually significant cataract and infants with a mild degree of cataract at birth, which later progressed to require surgery. To our knowledge, there are no studies evaluating the outcome of bilateral primary IOL implantation in infants exclusively operated within the first 12 weeks of age, in which all had visually significant cataract at birth. Therefore, the main aim of this study was to evaluate the visual outcome and safety in terms of glaucoma and VAO after bilateral cataract surgery with implantation of an IOL in infants with visually significant cataract at birth, operated before 12 weeks of age.
Materials and methods
Patient material
About 3/4 of all children with congenital cataract in Norway are treated at the Department of Ophthalmology, Oslo University Hospital. In the present study, consecutive infants with bilateral congenital cataract referred to our hospital were considered for inclusion. Eligible for the study were infants who underwent bilateral cataract surgery with primary IOL implantation before 12 weeks of age in the period January 2007 to December 2016. In this 10-year period, 23 infants underwent bilateral cataract surgery. Four infants (eight eyes) were not suitable for IOL implantation due to microphthalmos (axial length (AL) less than 16 mm) and/or small corneal size (horizontal diameter less than 10 mm) and were left aphakic. Two of these infants (four eyes) also had a moderate to severe persistent fetal vasculature (PFV). These four infants (eight eyes) were excluded from the study. In addition, four infants were not included due to lack of informed consent. Informed consent was obtained from 15 parents of the 19 infants who had cataract surgery with primary IOL implantation. The included 15 patients had a thorough study follow-up examination in 2017. In addition, the medical records were reviewed for all information concerning the surgery and all scheduled visits.
Patient and public involvement
The Norwegian Association of the Blind and Partially Sighted (patient organisation) was involved in the planning, and the results of the study have been disseminated to them. Patients were not directly involved in the design of this study.
Surgical procedure
All surgeries were carried out under general anaesthesia by three experienced surgeons. Prior to surgery, biometric measurements were performed, including AL (Immersion A-scan ultrasound Echoscan US- 500, Nidek) and corneal curvature (Righton-Retinomax K-plus 3, Opto Medica Oftalmologia Srl.). The corneal diameter was measured with a calliper.
The main incision was made by means of a corneoscleral tunnel of 2.75 mm at the 12 o’clock position, together with two stab side ports. Intracameral phenylephrine and lidocaine were installed. The anterior continuous curvilinear capsulorhexis (CCC) was aimed with a diameter of approximately 5 mm. In cases of poor visibility, trypan blue (VisionBlue, Dutch Ophthalmic Research Center) was used to stain the anterior capsule. Lens material was aspirated by bimanual infusion-aspiration using Alcon Infinity Phacoemulsifier (Alcon Laboratories). In all eyes, a posterior CCC followed by a dry anterior vitrectomy was performed. The IOL was fixated in the capsular bag in all cases. The IOL type used was AcrySof SN60WF (30%, n=10) or SA30 (60%, n=18) (Alcon Laboratories) or Hoya AF-1-Model NY-60 (7%, n=2) (HOYA Surgical Optics). The surgeons calculated the IOL power by using the SRK/T formula, however, they mostly implanted IOL with a power of 28–30 diopters (D), aiming for postoperative hyperopia (about +8 D to +10 D) due to the expected myopic shift. The incisions were closed with a 10–0 Vicryl suture (Ethicon). At the end of surgery, cefuroxime 0.1 mL was injected intracamerally together with an injection of betamethasone 0.3 mL subconjunctivally adjacent to the main incision.
Surgical procedure for posterior VAO was the removal of the opacities with a one port pars plana vitrectomy. In cases of VAO anterior to the IOL, secondary cataract material was aspirated, whereas membranes were removed with forceps and microscissors.
Postoperative treatment and examination
All patients received either dexamethasone (1 mg/mL) or a combination of topical dexamethasone (1 mg/mL) and chloramphenicol (5 mg/mL), 6 to 12 times a day for 1 week. After 1 week, only dexamethasone was used and tapered off over approximately 2 months. In addition, cyclopentolate 0.5% was given three times a day for the first 3 weeks. The treatment was adjusted when required.
All patients were routinely examined by an orthoptist, an optometrist and an ophthalmologist after 1 day, 1 week, 1 month and then at intervals of 3 to 4 months. Examinations under anaesthesia were performed when required, for example, when clinical suspicion of secondary glaucoma. Refraction was assessed by retinoscopy the first postoperative day, or as soon as possible. The residual refractive error, with additional +3.00 diopters (D) to provide near-point correction, was prescribed by means of contact lenses to all patients (Hydrolens, Cantor & Nissel or Aphakic SiH, Ultravision CLPL). Bifocal glasses (instead of contact lenses) were initiated in all patients when the child was approximately 2.5 years old. However, in cases where the parents were unable to manage contact lenses, or the children for other reasons had problems wearing contact lenses, the children were prescribed spectacles.
Follow-up examinations
The patients were enrolled for a prospective follow-up examination in 2017, which included a detailed medical history and a thorough ophthalmological examination. All data were collected using a standardised case report form, and the examinations were performed by an experienced paediatric cataract surgeon (SC), an orthoptist and an optometrist. Corrected distance visual acuity (CDVA) was measured with age-appropriate visual acuity testing charts (eg, Cardiff cards, Teller Acuity cards, Lea grating acuity or Snellen chart). Twelve (80 %) of the 15 children were tested with optotypes. In two infants with Down syndrome (three eyes, 10%), CDVA was not achievable at the follow-up examination due to poor cooperation in one infant and anisometropic amblyopia and poor cooperation in the other infant. The CDVA values were converted to logMAR equivalents for analysis. In addition, objective and subjective refraction was performed, if possible. Examination of the eyes’ red reflex, indirect ophthalmoscopy, slit lamp examination (ordinary, if possible, otherwise handheld) were conducted. A rebound tonometry (iCare PRO, Icare) or Goldmann applanation tonometry was used for intraocular pressure (IOP) measurements. Perkin handheld applanation tonometer (Haag-Streit) was applied when the patients were examined in general anaesthesia. For cooperating children, the eye’s AL and corneal curvature were assessed (AL-Scan optical biometer Nidek).
The diagnosis of glaucoma was made in accordance with a classification system for paediatric glaucoma.11 The diagnosis was given if the eyes had two of the following criteria: IOP >21 mm Hg, optic nerve cupping, Haab striae or increased corneal diameter, visual field defects, increased AL or myopic shift that outpaced normal growth. VAO were registered when surgery was required and were defined as opacification either on the anterior and/or posterior surface of the IOL, anterior and posterior capsular phimosis or fibrinous membrane in the pupillary field.
Statistical methods
Since the patients were examined at different ages, and some of the eyes had not reached their visual potential during the research period, we adjusted for age in our statistical analysis. We used a non-linear mixed-effect regression model to account for the correlation of multiple measurements on each eye and measurements on both eyes of each patient. The models were fit using restricted maximum likelihood. By extending the model in Wang et al12 to include random effects, the CDVA (logMAR) was modelled by:

where i refers to the ith patient, j refers to the jth eye on the patient, k refers to the kth examination, α1ij is the initial CDVA parameter, α2ij is the final CDVA parameter and α3ij represents the exponential rate of change in CDVA with respect to time. The parameters α1ij, α2ij, α3ij were each decomposed into a fixed effect parameter part, a patient-specific random effect part and an eye-specific random effect:

where  . The measurements error εijk and random effects a1ipat, a2ipat, a3ipat, a1ijeye, a2ijeye, a3ijeye were assumed to be independent and normally distributed. We added main effects to the model to test whether certain baseline characteristics could explain initial CDVA, final CDVA and the exponential rate of change. Multiple regression analysis was performed using the backward elimination method.
. The measurements error εijk and random effects a1ipat, a2ipat, a3ipat, a1ijeye, a2ijeye, a3ijeye were assumed to be independent and normally distributed. We added main effects to the model to test whether certain baseline characteristics could explain initial CDVA, final CDVA and the exponential rate of change. Multiple regression analysis was performed using the backward elimination method.
The secondary glaucoma data were presented with descriptive statistics and Kaplan-Meier plot. Due to the correlation between the eyes, the left eye was selected for the Kaplan-Meier analysis. For comparison between follow-up of patients with secondary glaucoma and the rest of the study patients, we used a Wilcoxon signed-rank test. To avoid correlation between eyes in the same patient, we used the average value for each patient.
Summary of observations is presented as median (range, minimum to maximum). Regression results are presented as mean (95% CI). A p value <0.05 was considered statistically significant. All analyses were conducted in R packages.13 Residual plots were inspected for possible violations of model assumptions of independence, normality and homogeneity of variance for error terms.
Results
Preoperative parameters (baseline characteristics) are presented in table 1.
Baseline characteristics in patients undergoing bilateral cataract surgery before 12 weeks of age (n=15 patients, 30 eyes)
Median age of the patients was 35 days (range, 15 to 70 days) at the time of primary cataract surgery. The intraoperative complications were few and minor: one eye (3%) had an iris injury with some pigment loss, one eye (3%) had an irisprolapse and one eye (3%) had a tear in the posterior CCC. The median age at follow-up was 6.1 years (range, 1.5 to 10.2 years). Ocular biometry measures at follow-up are presented in table 2.
Characteristics at the study follow-up examination in patients undergoing bilateral cataract surgery before 12 weeks of age (n=15 patients, 30 eyes)
Visual acuity
The median CDVA at the follow-up examination was 0.5 logMAR (range, 1.2 to 0.04 logMAR; n=27) before age correction. In the better-seeing eye, the median CDVA was 0.44 logMAR (range, 1.10 to 0.04 logMAR; n=14). When children with Down syndrome were excluded, the median CDVA of the better-seeing eye was 0.34 logMAR (range, 1.10 to 0.04 logMAR; n=10). The CDVA development during the study period is illustrated in figure 1. Even though three eyes were not measured at the follow-up examination, CDVA was tested at previous examinations. Thus, all 30 eyes were included in the regression analysis (193 measurements). A trend from the model in equation 1 is presented with predicted CDVA up to 10 years. The CDVA was improved with age (p<0.001), and age-adjusted CDVA at 5 years of age was 0.45 logMAR (range, 0.98 to 0.14).

Corrected distance visual acuity (CDVA), logMAR versus age (years) with estimated trend line (solid grey line) for the 30 eyes: logMAR = (2.09–0.48) exp(−0.94 age)+0.48. The grey dots represent the CDVA measured at the follow-up examination, other dots represent other examinations, and the connected lines represent the CDVA development. The grey line represents the estimated mean CDVA as a function of age. The dashed lines represent the normative paediatric CDVA as shown by Salamoa and Ventura27and Pan et al.28
Out of the variables examined (lens morphology, age at surgery, number of surgeries for VAO, secondary glaucoma, PFV and preexisting posterior capsule defect, Down syndrome and prematurity), only Down syndrome (estimate=0.354; 95% CI 0.61 to 0.095; p=0.008) and prematurity (estimate=0.41; 95% CI 0.77 to 0.058; p=0.024) showed a statistically significant association with worse final CDVA. None of the variables significantly improved the model for the exponential rate of change. With a multivariate model using the same variables with p<0.15 from the previous tests, only Down syndrome was found as a predictor of worse visual acuity.
Visual axis opacification
All eyes required surgery for VAO within the first year after cataract surgery. The first operation for VAO was performed 3.5 months (range, 1.2 to 5.8 months) after cataract surgery, and the median number of surgical procedures for VAO was 2.0 (range, 1 to 5). Eleven eyes (37%) required only one surgical procedure. The latest surgery for VAO was performed after 2.7 years.
Secondary glaucoma
Three patients (five eyes; 17%) developed secondary glaucoma. Their characteristics are presented in table 3.
Descriptive statistics, eyes with secondary glaucoma
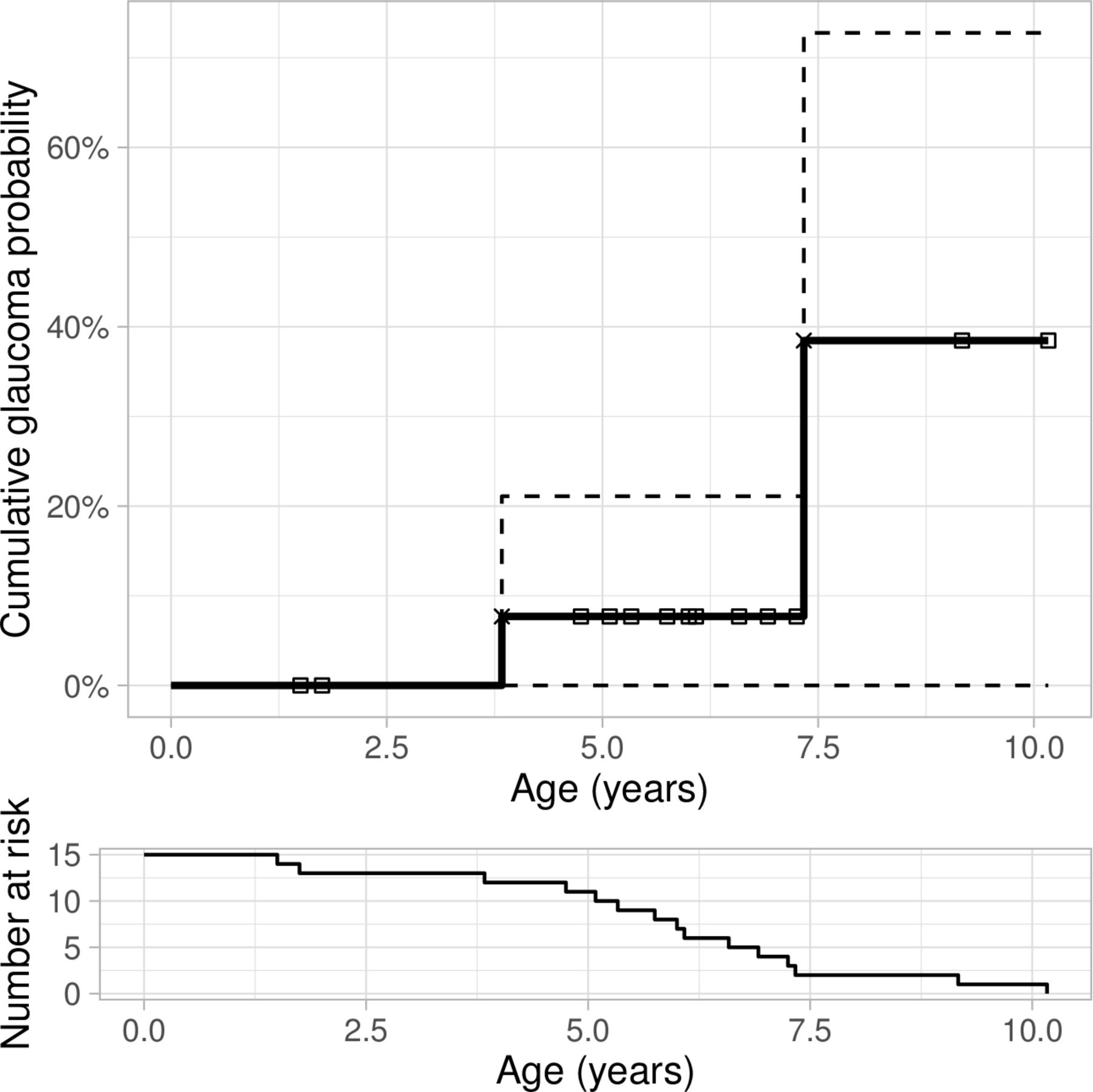
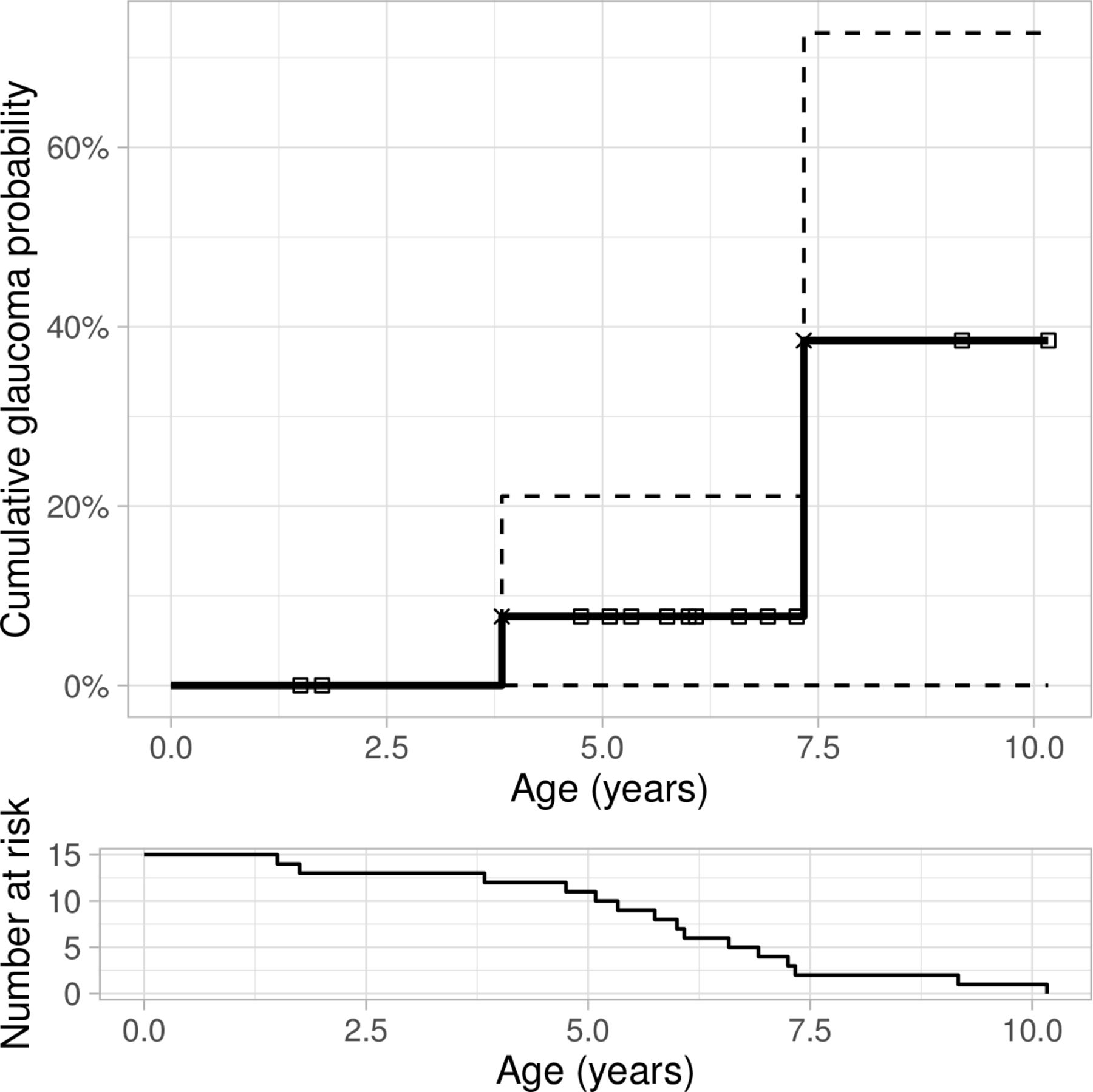
The median time for detection of glaucoma was 3.9 years (range, 3.8 to 7.3 years) after cataract surgery. These three patients with glaucoma had a median follow-up of 7.6 years (range, 7.3 to 9.9 years) compared with 6 years (range, 1.5 to 10.2 years) for the rest of the study patients (p=0.070). The cumulative incidence of secondary glaucoma was 10% after 5 years (Kaplan Meier analysis), and increasing with a longer follow-up (figure 2).
{kind=link}
{kind=link}
Kaplan-Meier estimator displayed as a solid line, showing the cumulative probability of developing secondary glaucoma versus time after cataract surgery. Small squares (upper part of figure) represent patients having last follow-up examination without having developed secondary glaucoma (censored). The 95% CIs are shown as dashed lines. The risk table at the bottom shows the number of patients at risk at certain time points.
Other postoperative complications
Four patients (five eyes; 17%) had transient steroid-induced IOP elevation; one eye after primary cataract surgery and the others after removal of VAO, however, none of these eyes developed secondary glaucoma during the follow-up time. Otherwise, no serious postoperative complications occurred.
Discussion
In this observational study, we found a satisfactory visual outcome after primary IOL implantation in infants with congenital bilateral cataract who were operated on before 12 weeks of age. With such a young age at surgery (median 35 days, and the oldest one 10 weeks of age) as well as the long follow-up time of median 6.1 years, we believe that this study provides important new knowledge about primary IOL implantation in this young patient group.
In the last decade, improvements in surgical technique, technology and better understanding of the growth of the eye have led to a more positive attitude among paediatric cataract surgeons to implant an IOL even in the youngest infants. Still, there exist controversies and challenging aspects, especially in those below 6 months of age, and there is to date no consensus regarding the minimum age for primary IOL implantation. The controversies are due both to the higher risk of VAO requiring additional surgery, to the risk of developing secondary glaucoma and to the unpredictable myopic shift that leads to variability in refractive outcomes.5 6 8 On the other hand, primary IOL implantation has the advantage of providing a partial optical correction at all times and may allow for a more optimal visual development and thereby preventing amblyopia. Vasavada et al7 found that visual rehabilitation was faster in pseudophakic compared with aphakic eyes. This is assumed to have a positive impact on the activity of the child and likely also the overall functional development. Primary IOL implantation in children also has the advantage of better visual stimulation than aphakia in patients who refuse to use glasses or contact lenses even if prescribed.
In the present study, the median CDVA at the follow-up examination was 0.5 logMAR without age correction. Since visual acuity improves as a result of visual stimulation during the first few years,12 we also accounted for different ages at follow-up using a regression model with an age trend (figure 1). This gave a predicted age-corrected mean CDVA of 0.45 logMAR at 5 years of age. This was somewhat inferior to the visual outcome of the Toddler Aphakia and Pseudophakia study (TAPS).9 However, they excluded most children with chromosomal and neurodevelopmental anomalies from the visual acuity summaries, and the age at surgery was 1 to 7 months. After removing the children with Down syndrome and the one with Lowe syndrome from our study, the median CDVA of the better-seeing eye was comparable to the TAPS study. Our results are also in accordance with previous reports of primary IOL implantation in an older age group.5 7 However, in these studies, the infants who were operated as early as in our study were left aphakic, and these aphakic children did not achieve a similarly good visual outcome.5 7 Furthermore, age at onset of cataract is an important factor of the visual outcome in these patients, and contrary to other studies on paediatric cataracts, we only included infants with visually significant cataract at birth. The visual outcome in the present study was in accordance to the other studies,5 7 9 that also included patients who were more likely not having visually significant cataract at birth with, therefore, a potentially more favourable visual prognosis.
Studies have shown that younger age at surgery increases the risk of VAO.5 14 In the present study, all patients were operated within 12 weeks of age, and all eyes required treatment for VAO. Vasavada et al, Bothun et al and Solebo et al reported lower incidences of VAO (10% to 39%) in studies with a higher age at surgery.5 7 9 The different incidences of VAO in the literature may also be explained to an extent by different surgical techniques and also classification; for example, in our study, we had a rather inclusive definition of VAO as all surgeries necessary to obtain a clear visual axis. Our high incidence of VAO may be explained by the close follow-up, and an aggressive approach to treat VAO in order to reduce the risk of amblyopia, but probably first of all the low age at cataract surgery. As primary IOL implantation causes more reoperations due to VAO,5 9 it has been questioned whether such repeated exposure to general anaesthetics during this key period of neurodevelopment may be dangerous for these small children. However, a recently published randomised trial did not find an increased risk of neurocognitive or behavioural deficits after multiple general anaesthesia in infancy.15 Nevertheless, newer approaches as the bag-in-the-lens can be considered in some selected cases to reduce VAO,16 however, this technique can be challenging in this young patient group.
Secondary glaucoma remains the most serious sight-threatening complication after cataract surgery in infants.17 Previous studies have discussed various potential risk factors, such as early surgery, especially in the first month of life.18 We found a cumulative glaucoma risk of 10%, which is in accordance with previously reported 5-year incidences of 5%–13.8% for bilateral paediatric cataract.5 7 Furthermore, the role of primary IOL implantation following congenital cataract surgery has been reviewed in previous reports. Several studies have not found any significant difference in the incidence of secondary glaucoma between aphakic eyes and eyes with primary IOL implantation.7 19 Others have found that the risk is higher in aphakic eyes,20 and that the presence of an IOL is protective for the development of secondary glaucoma.18 However, these reports may suffer from selection bias, as the surgeons may choose IOL implantation in eyes that are less likely to have complications.19 Still, a recently published systematic review and meta-analysis by Zhang et al17 concluded that there is a significantly lower risk of secondary glaucoma after primary IOL implantation in patients under 2 years of age with bilateral congenital cataract in comparison with aphakia.
In the present study, we found a high variation in refraction at the follow-up examination and mostly with a large myopic shift. Selection of an IOL with appropriate power for implantation in paediatric eyes is complex, as IOL power calculation formulas give a large prediction error in these young children.21–23 The high myopic shift and unpredictable refraction are disadvantages of primary IOL implantation in infants.6
Implanting the IOL in the capsular bag is preferable, as sulcus fixation increases the risk of IOL malposition, postoperative inflammation and secondary glaucoma.24 The alternative to primary IOL implantation is aphakia, with or without secondary IOL implantation later in childhood, when IOL power predictions may be more reliable.25 With secondary implantation, however, it may be difficult to dissect the anterior and posterior capsule apart; one study found that the IOL had to be implanted in the ciliary sulcus in as many as 72% of the cases.26 In our study, all eyes had the IOL placed in the capsular bag.
The clinical implication of the present study is that cataract surgery in infants younger than 12 weeks of age is safe in terms of visual outcome. The incidence of secondary glaucoma is similar to that reported after primary IOL implantation in older infants. However, the risk of VAO is high, and the parents must be informed that frequent follow-up examinations and additional surgery for VAO in general anaesthesia are necessary. Another disadvantage is that the high myopic shift in young children gives a rather unpredictable final refraction. The advantage of an implanted IOL, however, is that it provides a permanent continuous correction of aphakia, which may be favourable especially during early childhood to prevent amblyopia and to enhance visual development.
The strength of the present study is that it includes an unselected and nationally representative group of the youngest infants with bilateral cataract in Norway. Other advantages are few surgeons, a long and close follow-up, and that all infants had a comprehensive prospective study examination. Limitations of the study are the non-comparative design and that some data were obtained by retrospective review of medical records. Another limitation is the small sample size. However, the study participants included most of the patients with visually significant bilateral cataract at birth operated on in a 10-year period in a university hospital clinic. In conclusion, our study shows that primary IOL implantation before 12 weeks of age gives a favourable visual outcome and that it can be considered as a primary modality of treatment, with the appropriate surgical and anaesthesia experience, and close follow-up.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Oslo University Hospital’s Data Protection Office and the Regional Committee for Medical and Health Research Ethics (South-East Norway, reference number 2016/165). The research was performed in accordance with the Helsinki declaration.
Acknowledgments
We want to thank Anna-Katarina Litzen Jørstad and Katinka Jeber (Department of Ophthalmology, Oslo University Hospital), who respectively contributed with the orthoptic and optometrist examination of the children in the comprehensive follow-up examination and contributed to data acquisition. We also want to thank Lotte-Guri Bogfjellmo Sten (Department of Optometry, Radiography and Lighting Design, University of South-Eastern Norway, Campus Kongsberg) who contributed to the design of the study and in the plotting of data. We also want to thank the Norwegian Association of the Blind and Partially Sighted (NABP) for the involvement in the planning of the study.
References
Footnotes
Contributors Patient examination and data acquisition: SC, EDK, MKS. Data analysis and interpretation: KR, MKS, SC, OK, LD. Article writing and critical revision: MKS, SC, KR, EDK, OK, LD. Supervision: OK, LD.
Funding This work has been funded by the South-Eastern Norway Regional Health Authority, Norway (grant number:2018034) and the Norwegian Association of the Blind and Partially Sighted (NABP), and the project has also received small grants from Inger Holms Memorial Fund and Arthur and Odd Clausons Foundation.
Disclaimer The funding organisations had no role in the design or conduct of this research and have no related commercial interests.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.