Article Text

Abstract
Objective The purpose of this study is to investigate the amount of oral flora dispersion towards the ocular surface in relation to various face mask scenarios.
Methods and analysis Thirty participants were recruited for this prospective cross-sectional study. Each participant was seated and instructed to hold a blood agar plate perpendicular to the bridge of their nose and facing downward. Participants then partook in three unique face mask scenarios: no face mask, surgical face mask and surgical face mask with tape securing the superior edge. During each scenario, participants were instructed to forcefully exhale for 5 s three times. The primary outcome measure was the number of colony-forming units (CFUs) grown on each face mask scenario-specific plate.
Results Thirty participants were recruited for the study, and a total of 90 chocolate agar plates were successfully incubated. The proportion of detecting any CFU was 6.67% (95% CI: 0.818% to 22.1%) for no mask scenario, 0% (95% CI: 0% to 11.6%) for mask scenario and 3.33% (95% CI: 0.0844% to 17.2%) for mask-taped scenario. The mean differences in proportion of detecting any CFU were 3.33% (95% CI: 0% to 10%, p=0.309) for no mask versus mask taped, 3.35% (95% CI: 0% to 10%, p=0.307) for mask taped versus mask and 6.68% (95% CI: 0% to 16.7%, p=0.142) for no mask versus mask.
Conclusion This study showed no difference in bacterial dispersion towards the ocular surface when comparing no face mask, a surgical face mask without tape or a surgical face mask with tape.
- ocular surface
- microbiology
Data availability statement
Data are available upon reasonable request. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Face masks redirect airflow towards the ocular surface. The impact of this redirected airflow on the dispersion of oral flora is unknown.
What are the new findings?
No difference in bacterial dispersion towards the ocular surface was found when comparing no face mask, a surgical face mask without tape or a surgical face mask with tape.
How might these results change the focus of research or clinical practice?
The results may help direct future studies regarding other benefits of taping one’s mask, such as decreased mask-associated dry eyes or spectacle/eye protection fogging.
Introduction
As a result of the COVID-19 pandemic, patients are using face masks more frequently. It has been well described that face masks decrease the forward spread of oral flora from an individual’s mouth and nose.1 2 However, the use of face masks redirects airflow towards the ocular surface. The impact of this redirected airflow is not well understood. Prior studies have demonstrated that the dispersion of oral flora may be reduced through face mask use by physicians and implementing a no-talking policy during intravitreal injections.3 4 However, the effect of face mask use on the dispersion of oral flora is still unknown. Thus, face masks that allow expiration to be redirected superiorly instead of forward may increase the risk of ocular contamination by oral flora when worn by patients during or immediately after eye procedures.
Endophthalmitis is a potentially devastating complication of eye surgeries and intraocular procedures. In the USA, the incidence of postoperative endophthalmitis following cataract surgery has been reported at 0.04%.5 Recent studies compared the bacterial isolates in endophthalmitis following intraocular surgery and found 8.2%–9.0% of isolates were Streptococcal species.6–8 Additionally, the reported incidence of post injection endophthalmitis in the literature ranges between 0.019% and 0.09%.9 10 A recent meta-analysis revealed that 30.8% of bacterial isolates in post injection endophthalmitis were Streptococcal species.11 The source of infection in oral flora-associated endophthalmitis is thought to be driven by contamination of the operative or procedural field through droplet spread or aerosolisation.11–15 Therefore, any potential for increasing and channelling the nasal and oral flora directly to the eye is a risk for infection that needs to be understood so that proper interventions can be implemented. The purpose of this study is to investigate the amount of oral flora dispersion towards the ocular surface in relation to various face mask scenarios.
Methods
Overview and patient involvement
This is a prospective, cross-sectional study on healthy adult volunteers, ≥18 years of age, who provided written informed consent. The study was conducted in accordance with the tenants of the Helsinki declaration. Patients were not involved in setting the research question, the outcome measures or the design and implementation of the intervention.
Study participants
Thirty participants were recruited for this study. Inclusion criteria included participants ≥18 years of age who answered no to COVID-19 screening questions, who could comfortably wear a mask and self-identified as able to forcefully exhale for 5 s three times in three scenarios. Exclusion criteria included any participant with a pending COVID-19 nasal swab test, who could not comfortably wear a mask, who could not forcefully exhale while wearing a mask, who could not have surgical tape placed near their skin, who was using any form of antibiotics within 14 days of their participation, who self-reported a history of asthma or chronic obstructive lung disease or who had a history of cough, chills, fever, upper respiratory infection or gastrointestinal symptoms within 14 days of their participation. All participants were screened for COVID-19 symptoms on entrance to the facility.
Study design
Each participant was seated behind a plexiglass shield and provided gloves and an iPad to review the standardised instructions. Participants were then randomised into one of four possible sequences. Each sequence had a unique order of three possible face mask scenarios: (1) no face mask; (2) a surgical face mask (HUAFU HF8111 Particulate Respirator Disposable Face Masks); (3) a surgical face mask (HUAFU HF8111 Particulate Respirator Disposable Face Masks) and tape spanning from lateral canthi to secure the superior edge of the face mask. Each participant was allocated four standardised 100 mm circular chocolate agar plates which were labelled with a study ID # and a letter representing the face mask scenario. One plate was placed approximately 10 feet from the participant and served as a Room Control plate. Chocolate agar plates were used in lieu of blood agar plates to maximise sensitivity of detection, including recovery of fastidious flora (eg, Haemophilus spp). Participants were then provided the face mask scenario-specific plate and were instructed to place the plate at the bridge of their nose, facing downward and parallel to the floor (figure 1). Participants were then instructed to forcefully exhale for 5 s three times, rotating the agar approximately 120° clockwise in-between each exhale. Participants waited approximately 5 min in-between each face mask scenario, before being provided a new face mask scenario-specific plate and repeating the process.
Subjects held the face mask scenario-specific plate to the bridge of their nose, facing downward and parallel to the floor.
All chocolate agar plates were sealed and transported to the microbiology lab. The plates were incubated for 48 hours at 37°C in a 5% carbon dioxide-rich environment. The number of bacterial colonies per plate was counted by microbiologists who were masked to the plate collection sequence. Bacterial species-level ID was not performed, and no organisms were excluded as the premise of this study was to be strictly quantitative in terms of CFU counts.
Statistical analysis
Sample size was modelled off prior studies that were able to detect a valid difference between various scenarios with 15 participants.3 16 The proportion of detecting any CFUs and 95% CIs were reported for all three face mask scenarios. The 95% CIs for the mean proportion difference between any two face mask scenarios and their associated two-sided p values were constructed using a non-parametric bootstrap method with 100 000 bootstrap samples stratifying on participant. Statistical significance was considered to be a two-sided p value <0.05. All data were analysed using R V.3.6.1.
Results
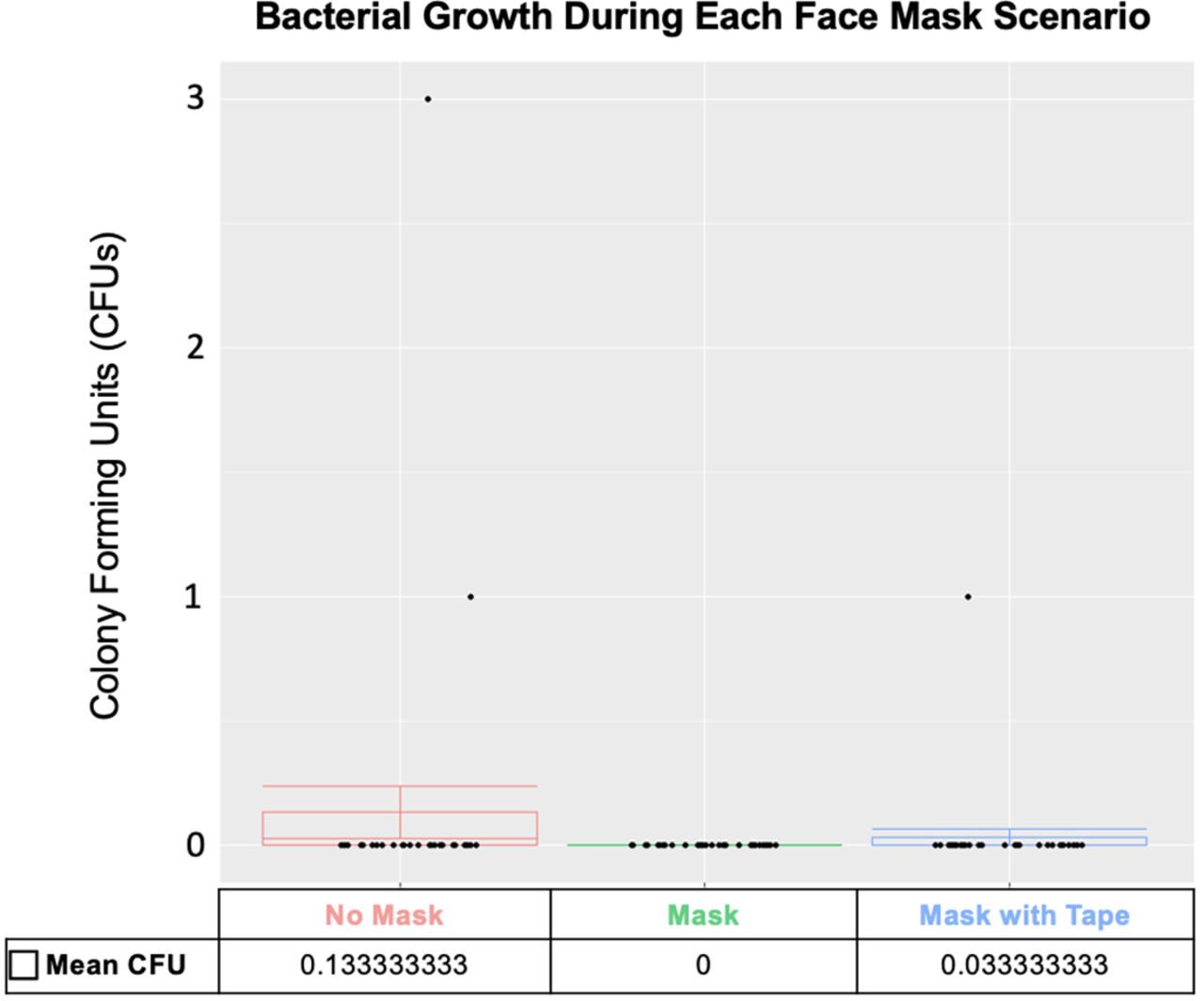
Thirty participants were recruited for the study, and a total of 90 chocolate agar plates were successfully incubated. The proportion of detecting any CFU was 6.67% (95% CI: 0.818% to 22.1%) for no mask scenario, 0% (95% CI: 0% to 11.6%) for mask scenario and 3.33% (95% CI: 0.0844% to 17.2%) for mask-taped scenario. The mean differences in proportion of detecting any CFU were 3.33% (95% CI: 0% to 10%, p=0.309) for no mask versus mask taped, 3.35% (95% CI: 0% to 10%, p=0.307) for mask taped versus mask and 6.68% (95% CI: 0% to 16.7%, p=0.142) for no mask versus mask.
Figure 2 shows the mean CFUs among the different face mask scenarios. The no mask scenario grew the most colonies with a total of four CFUs or a mean±SD of 0.13±0.57 per participant. In contrast, the mask scenario grew the fewest number of colonies with a total of 0 CFUs. The sequence effect of face mask scenarios could not be evaluated due to an insufficient sample size.

{kind=link}
{kind=link}
Distribution of face mask scenario-specific plates and the mean bacterial growth based on colony-forming units (CFUs) under various face mask scenarios.
Out of the 30 Room Control plates, only six grew CFUs at 48 hours. One Room Control plate was excluded after being deemed to be contaminated by physical touch. The other five Room Control plates came from sets where all associated face mask scenario-specific plates grew no CFUs.
Discussion
As a result of the COVID-19 pandemic, patients are using face masks more frequently. Face masks redirect airflow towards the ocular surface. The impact of this redirected airflow on the dispersion of oral flora is unknown. Prior studies have shown wearing a face mask or remaining silent significantly decreases bacterial dispersion from the perspective of the physician during intravitreal injections.3 However, it is unclear if the bacteria linked with oral flora-associated endophthalmitis is emanating from the physician, patient or both. We hypothesise face masks that allow expiration to be redirected superiorly instead of forward may increase the risk of ocular contamination by oral flora when worn by patients during or immediately after eye procedures. However, this investigation of bacterial dispersion during forced exhalation with three different face mask scenarios found that using a taped face mask resulted in no statistically significant difference in bacterial dispersion when compared with using an appropriately worn face mask.
Our analysis showed no significant difference in bacterial dispersion when comparing any of the three face mask scenarios. However, the comparison of no mask versus mask demonstrated the greatest mean difference in proportion of detecting any CFUs. Participants wearing a surgical face mask without tape covering the superior edge grew an equivalent amount of CFUs when compared with the same face mask with tape securing the superior edge. Based on these results, a larger sample size is needed to confirm the null hypothesis. However, a similar study showed a significant difference in CFU growth between mask versus mask taped with half the number of participants and agar plates.16 In this context, we believe it is reasonable to conclude there is not a large increased risk of oral bacteria being directed toward the eyes with mask wear perioperative or periprocedural while upright.
The aforementioned study examined the relationship between patient face mask use and bacterial dispersion during a simulated intravitreal injection. They concluded that taping the superior edge of a patient’s mask can reduce bacterial dispersion during simulated intravitreal injections.16 A similar study using comparable conditions found no significant difference in taping the superior edge of a mask to decrease bacterial dispersal towards the ocular surface when compared with an appropriately worn mask.17 Both studies used 2 min of talking to simulate the potential dispersion of bacteria, and both had participants in a reclined position to simulate intravitreal injections. A ‘no-talking’ policy during intravitreal injections is widely accepted practice and is supported by the 2018 European Society of Retina Specialists expert consensus recommendations.18 However, the studies above chose to have the participants speak for 2 min as this improved their culture yields.17 The current study evaluated bacterial growth under simulated exhalation scenarios where participants were instructed to exhale forcefully for 5 s while wearing various face masks. Participants in this study were seated in the upright position to simulate postoperative face mask use. Despite finding taped masks to be equal to appropriately worn masks regarding bacterial dispersion, prior studies have demonstrated qualitatively that taping the superior edge of a face mask can effectively block airflow directed to the ocular surface to undetectable levels.19 Thus, taping one’s mask could provide other benefits, such as decreased mask-associated dry eyes (MADE) or spectacle/eye protection fogging. Additionally, taped masks can act as a deterrent to patients lowering or removing their mask during a visit.
Endophthalmitis is a rare but devastating complication of eye surgeries and intraocular procedures. In the USA, the incidence of postoperative endophthalmitis following cataract surgery has been reported at 0.04%.5 Recent studies compared the bacterial isolates in endophthalmitis following intraocular surgery and found 8.2%–9.0% of isolates were Streptococcal species.6–8 Additionally, the reported incidence of post injection endophthalmitis in the literature ranges between 0.019% and 0.09%.9 10 A recent meta-analysis revealed that 30.8% of bacterial isolates in post injection endophthalmitis were Streptococcal species.11 Although the risk of infection is relatively low, the prognosis of oral flora-associated endophthalmitis is poor.20–22 For this reason, great efforts have been taken to reduce the risk of postprocedural and postoperative endophthalmitis. Common methods of oral flora-associated endophthalmitis prevention include physician face mask use or a no-talking policy during intravitreal injections. These methods are widely accepted and are supported by the 2018 European Society of Retina Specialists expert consensus recommendations.18 However, it is unclear if the bacteria linked with oral flora-associated endophthalmitis is emanating from the physician, patient or both. This question is of particular importance during the COVID-19 pandemic where patients are required to wear masks throughout the procedure.3 23 24 In our study, there were no statistically significant difference in the mean difference in proportion of detecting any CFUs between any of the three face mask scenarios. However, during the no mask scenario, there was a greater absolute growth of CFUs.
Our study has several limitations. Due to our study’s limited sample size, we were unable to detect if a valid difference exists between the various face mask scenarios. The decision to recruit 30 participants was based off prior study results. These studies were able to detect a valid difference between various scenarios with 15 participants.3 16 The chocolate agar plates used in this study do not accurately represent the ocular surface. Additionally, we did not identify what species of bacteria grew on these plates. Another limitation involves not controlling for facial shape or hair. However, we standardised the placement of agar plates, the degree of exhalation and the orientation of face masks to reduce any differences between participants. Finally, it has not been shown that additional CFUs on the ocular surface can be directly related to an increased risk of oral flora-associated endophthalmitis. Additionally, the authors are not aware of any current literature showing an increase or decrease in endophthalmitis rates following intraocular procedures or intravitreal injections during the pandemic. However, due to the exceedingly poor visual prognosis of oral flora-associated endophthalmitis, it is crucial we eliminate any potential risks.
Overall, this study showed no difference in bacterial dispersion towards the ocular surface when comparing no face mask, a surgical face mask without tape or a surgical face mask with tape. However, during the no mask scenario, there was a greater absolute growth of CFUs. Future studies with a larger sample sizes may be able to detect if a valid difference exists. Additionally, data from this study could help direct future studies regarding other benefits of taping one’s mask, such as decreased MADE or spectacle/eye protection fogging.
Data availability statement
Data are available upon reasonable request. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Vanderbilt Eye Institute institutional review board (IRB# 201796), and all participants provided written informed consent.
Acknowledgments
This paper and the research behind it would not have been possible without the exceptional support of the Vanderbilt Eye Institute.
References
Footnotes
Contributors AC, JCL contributed to conception and design. AC, JCL, SA contributed to data collection. ASM, JES, QC, YL contributed to analysis and interpretation. SA contributed to first manuscript draft. SA contributed to critical revisions of the manuscript. AC, JCL contributed to obtained funding.
Funding Vanderbilt Eye Institute-Discovery Grant, Research to Prevent Blindness
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.