Article Text

Abstract
The purpose of the Utah Project on Exfoliation Syndrome (UPEXS) is to identify associations between exfoliation syndrome (XFS) and other diseases that share the commonality of abnormalities in elastin and Lysyl Oxidase-Like 1 gene regulation. The UPEXS is unique because it uses the Utah Population Database, which is linked to the Utah genealogy, that contains a compilation of large pedigrees of most families in the state of Utah that go back multiple generations (3 to ≥11). The health and medical records of these family members are linked to vital records and can be used effectively in studies focused on genetic disorders like XFS, where familial clustering of a disorder is a trend. There is increasing evidence that patients with XFS have a higher risk of certain systemic disorders that reflect the systemic tissue abnormalities of XFS. Epidemiological studies focused on patients with XFS have shown that there is an increased risk of these individuals developing other pathologies that have abnormalities in extracellular matrix metabolism and repair. UPEXS has focused on suspected comorbidities that involve abnormalities in elastin maintenance, a protein that plays a role in the makeup of the extracellular matrix. In this paper, the results from the analysis of chronic obstructive pulmonary disease, inguinal hernias, pelvic organ prolapse, obstructive sleep apnoea and atrial fibrillation are summarised along with the utility of using such a large dataset.
- glaucoma
Data availability statement
Data are available in a public, open access repository. Data are available upon reasonable request. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Exfoliation syndrome (XFS), also known as pseudoexfoliation syndrome, is a systemic age-related disease diagnosed by the deposition of extracellular fibrillar tissue in the eye’s anterior chamber. XFS is the most common form of secondary open-angle glaucoma. This bears great significance considering glaucoma is the leading cause of blindness throughout the world.1 Given the systemic and historical genetic underpinning for XFS to Lysyl Oxidase-Like 1 (LOXL1) risk alleles, the Utah Population Database (UPDB) was used to investigate diseases that a patient diagnosed with XFS might be predisposed to give the belief of an association with elastin, produced by LOXL1.2 The key pathological and clinical finding of XFS is exfoliation material present on a dilated eye examination. Although systemic, ocular findings are pathognomonic and include fibrillar deposits in the anterior chamber, most commonly located on the anterior capsule, lens zonules, and in the iridocorneal angle viewed by gonioscopy. The pupillary margin is also a common location for XFS material. The development of exfoliation glaucoma, iris transillumination defects and cataracts with zonular dehiscence are associated with XFS. Other than ocular involvement, deposited fibrillar material in patients with XFS can also be found in the brain, lungs, heart and skin.3 4
Epidemiology of XFS
The prevalence of XFS varies widely across ethnic groups and geographic regions, highlighting the hypothesised contributing factors such as epigenetics, ultraviolet radiation exposure (UVR) and latitude.5–10 Increased odds of XFS have been shown in geographic regions with increased latitude, which has been hypothesised to be due to an interplay between temperature and greater UVR reflectivity into the eye. Overall, there is a range of XFS prevalence throughout the world.
LOXL1
The LOXL1 gene has been of key interest over the years in trying to understand and elicit the pathophysiology and the risk for XFS. Its enzymatic products act to cross-link and convert tropoelastin to elastin, stabilising and creating functional fibrillar collagens and elastin within the extracellular matrix (ECM).11 12 LOXL1 is a copper-dependent enzyme that has a role in oxidising primary amine substrates to reactive aldehydes.12 In LOXL1 knockout mice, the observation has been made of an ECM dysregulation, particularly the metabolism of collagen and elastin.13 Thorleifsson conducted a genome-wide search that showed multiple single-nucleotide polymorphism (SNPs) in a specific region that is associated with exfoliation glaucoma. Two non-synonymous SNPs in the LOXL1 gene explain this association.11
Elastin is a crucial component of the ECM, and abnormalities in this protein’s metabolism and production have been linked to the LOXL1 gene. Studies have shown that mice lacking the gene do not produce normal elastic fibres. Other studies focused on elastin abnormalities have shown that altered or enhanced elastin degradation can lead to an increased chance of developing emphysema, atherosclerosis and cancer.14 Furthermore, elastin degradation has also been shown to be an effective marker for COPD.15 Although the LOXL1 knockout mouse may not translate directly to the human clinical pathology, it has directed research towards possible associations between XFS and related systemic pathologies that also involves the ECM and collagen and elastin metabolism.
It is interesting to hypothesise that an epigenetic effect like DNA methylation, caused by one or more environmental triggers, could be leading to these changes of altered ECM as well as LOXL1 and elastin protein expression alterations, such that faulty elastin repair process ensues. Recent research has focused on such epigenetic changes as possibly playing a role in the XFS phenotype.16 One recent study found that LOXL1 expression is altered via DNA methylation in ocular tissues and blood samples from patients with XFS.5 Kang et al demonstrated that non-melanoma skin cancer (a marker for UVR) was associated with a higher risk of exfoliation glaucoma.6 Other studies have demonstrated that UV exposure does lead to changes of DNA methylation in epidermal cells derived from the skin.17 It is these genetic and epigenetic underpinnings of systemic disease that can be investigated in populations by assessing XFS and elastin dysregulation disorders using large data resources.
Utah Project on Exfoliation Syndrome
Large databases containing decades of medical history and records of individuals are extremely beneficial in conducting population-based studies as investigators can gather important information about specific clinical phenotypes, environmental influences and disease manifestations that are electronically available for thousands of patients and correlate a phenotype of interest with possible associated comorbidities across a population. The UPDB is a unique representation of such a database, where large amounts of information can be gathered and linked to individuals over their life span. The UPDB contains the medical histories and vital records of >11 million individuals who either currently reside in Utah or who formerly lived in the state, as well as their ancestors as far back as the 1700s (see: www.uofuhealth.utah.edu/huntsman/utah-population-database/data/). The UPDB contains over 40 million records that span decades and are linked to an extensive statewide genealogy in which most families in Utah are represented in pedigrees of 3 or more generations.18 This dataset has enabled identifying genetic phenotypes that have been life-changing in terms of early detection, such as the breast cancer genes BRCA1 and BRCA2.19 20
Utah Population Database
The UPDB, housed at the Huntsman Cancer Center at the University of Utah, is a globally unique database that, for nearly 40 years, has enabled epidemiological and outcomes research to be conducted at the Utah population level.21 Using this resource, pedigrees can be identified with excess clustering of XFS in the Utah population to study familial XFS pathologies and examine associated comorbidities in both individuals and high-risk XFS families.
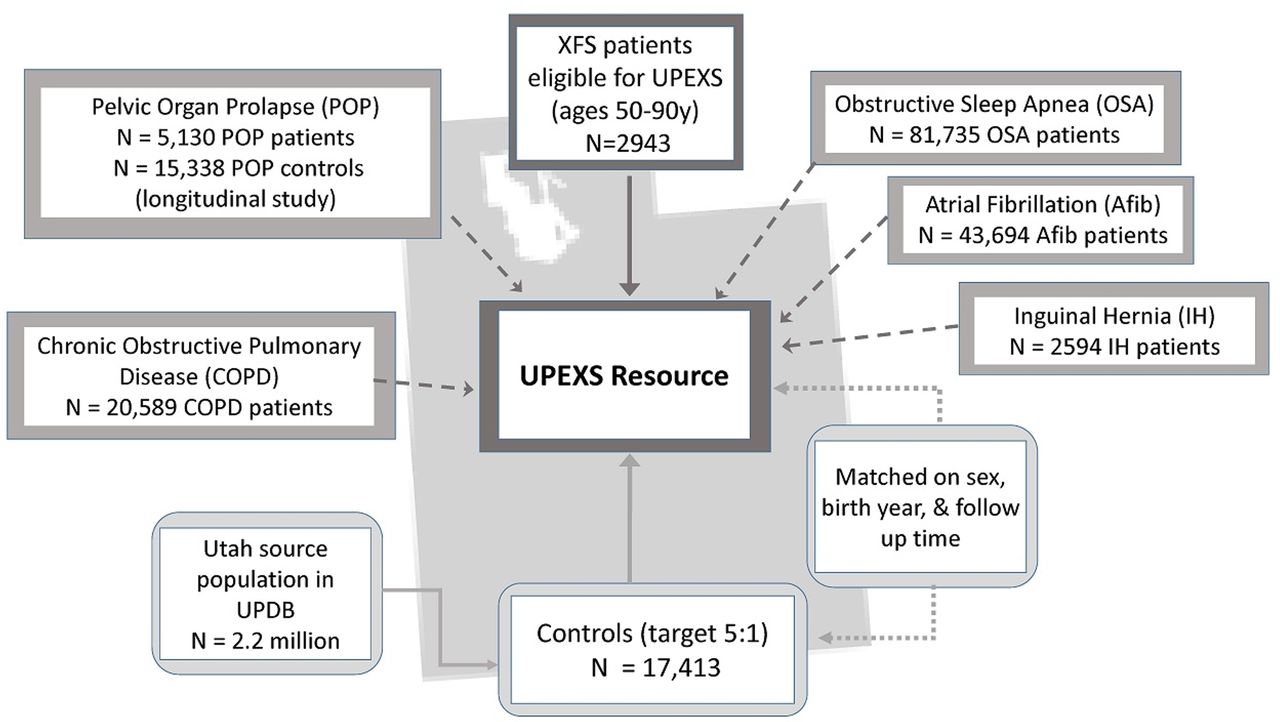
For UPEXS, participants’ historical data under an IRB-approved waiver of consent were obtained from the UPDB. We identified 2943 patients diagnosed in Utah with XFS between 1996 and 2015 for our studies and confirmed International Classification of Diseases (ICD) coding accuracy by randomised chart review. Sixty-eight per cent of our individuals with XFS were female, while 32% were male. Approximately 25% of this XFS case population was between 50 and 69, while 75% were between the age of 70 and 90. Over 95% of the population is white. The epidemiological characteristics of this XFS population closely mirror those of the Olmstead Study (Minnesota), which found that XFS incidence increased with age, with a mean age of diagnosis of 73 years, is derived from a population that was 95% white and 76% female.22 As a comparison cohort, population-based controls with no XFS history in UPDB were randomly selected and matched to XFS on sex, birth year, and follow-up time in Utah in a 5:1 ratio (N=17 413). A diagram of the UPEXS resource, including XFS patient and controls selection and XFS-associated comorbidity cohorts, is shown in figure 1.

{kind=link}
Utah Project on Exfoliation Syndrome (UPEXS) research resource overview. UPDB, Utah Population Database; XFS, exfoliation syndrome.
XFS and associated comorbidities
Through the utilisation of the UPDB and the establishment of the Utah Project on Exfoliation Syndrome (UPEXS), we have reported in several manuscripts data that supports the connection of XFS to various elastotic diseases in our Utah population, that is, chronic obstructive pulmonary disease (COPD), inguinal hernias (IHs), pelvic organ prolapse (POP), obstructive sleep apnoea (OSA), and atrial fibrillation (AFib) as associated comorbidities23–27 (table 1). We are currently investigating preliminary data of other potential associated comorbidities of XFS that follow a similar trend. These studies are based on the underpinning of the connection of XFS to a comorbid condition via abnormalities of the ECM pathway, deposition and elastin production and or repair. Furthermore, predispositions to XFS and its suspected comorbidities may share environmental mechanisms and or triggers leading to altered production of LOXL1, and changes in repair, and maintenance of the ECM, as well as the metabolism of elastin and collagen. One common factor that may play a role in the manifestation of these associated systemic comorbidities across our UPEXS patients is a triggering event; an insult and or injury (ie, UV exposure, surgery and or multiple vaginal births), traumatic and or inflammatory (ie, tobacco and inhaled smoke) that then requires the body to start an elastin/ECM repair process that in XFS malfunctions. Our continued UPEXS research shows that patients with XFS are predisposed to various systemic diseases that appear to be associated with elastin and ECM tissue abnormalities consistent with published data.1
Utah Project on Exfoliation Syndrome (UPEXS) comorbid phenotypes and XFS, summary of evidence
Chronic obstructive pulmonary disease
COPD is the third leading cause of death in the USA, and worldwide is one of the most prevalent chronic, life-threatening pulmonary emphysematous diseases.28 29 COPD occurs at higher rates in men, but in the past two decades, the rate of morbidity and mortality has risen in women.23 Rates of COPD diagnoses have been higher within the white European lineages.30 Changes in pathology consist of ciliary failure, bronchial fibrosis, hypertrophy of connective tissue and smooth muscle in airways, and an increase in deposition of ECM proteins: elastin, collagen and laminin.31–33 One study showed that elastin degradation could lead to an increased chance of developing emphysema.14 Pathological examination of lung tissue shows that samples with emphysematous changes have lower elastin LOXL1 expression and protein levels compared with those without emphysema. These decreased levels have been suggested to cause an altered repair process and an irregular elastic fibre system.34 Furthermore, inhaled smoke appears to be a trigger and or insult resulting in DNA methylation, which may play a role as an environmental trigger.35 36
UPEXS study design and results for COPD
Two patient cohorts were obtained from the UPDB for a 20-year period (1996–2015): an XFS cohort consisting of 2943 patients and a COPD cohort consisting of 20 589 patients. Both groups were between the age of 50 and 90 years at index diagnosis. ICD-9-CM codes were used to determine patients with XFS (365.52, exfoliation glaucoma, and 366.11, exfoliation of the lens capsule) and patients with COPD (COPD, 496.00). A control group of individuals was matched for age and sex to patients with XFS in a 5:1 ratio (N=14 713). A second control group with no history of COPD was randomly selected and matched for age and sex at a 5:1 ratio to patients with COPD (N=1 02 939). The control groups were necessary to have as long a follow-up period as their respective matched patient. In the XFS cohort, we examined the risk of having COPD compared with their matched control group with no history of XFS. Similarly, we examined the risk of having XFS in the COPD group compared with their matched control group with no COPD history.
The characteristics of XFS and patient with COPD cohorts and their matched control groups were examined and compared. In the XFS group, 68.0% were female, while in the COPD group, 43.6% were female. Variables including race, age at diagnosis and follow-up years did not differ greatly between men and women of either patient group. The mean age at the index of diagnosis was 75 years in the patients with XFS and 67 years in the patients with COPD. These ages are consistent with other published data.37 38
OR estimates showed that in the patients with XFS, risk of COPD diagnosis was higher when compared with the non-XFS controls (OR=1.41; 95% CI 1.17 to 1.70; p<0.0004), particularly in a subset of tobacco users (OR=2.17; 95% CI 1.15 to 4.09; p=0.02). Patients with COPD and their respective controls with no COPD did not differ in their risk of a diagnosis of XFS.
Inguinal hernia
Another degenerative disorder that appears to be caused by an abnormality in connective tissue regulation is indirect IH.39 Hernias are diagnosed when there is a protrusion of an organ or tissue through the fascia that normally contains it. A specific subtype of hernia known as inguinal is characterised by intra-abdominal contents protruding through the abdominal wall’s inguinal canal. IHs are either direct or indirect. A direct hernia is characterised by the protrusion going forward or in anterior direction when the individual stands up. An indirect hernia is characterised by the hernia going towards the scrotum or in an obliquely downward direction. Men are at a higher risk, with the rate being 27% and 3% for women.40 The risk factors for IHs include a prior hernia, increased age, trauma, white ethnicity, smoking and family history are all reported risk factors for IHs.41–45 XFS and IH share the common factor of connective tissue abnormalities, elastin connective tissue, specifically as an age-related process. Both disorders are associated with family history and possible epigenetic predisposition.46–48
UPEXS study design and results for IH
Using the UPDB, we were able to identify patients that underwent a surgical procedure to treat an IH from 1996 to 2015 based on the ICD-9 codes. We then examined its association with XFS (ICD-9 codes for XFS 365.52 and 366.1) in patients with an IH at the age of 40 or later compared with random control patients with the UPDB. Controls were sex and age-matched to cases in a 5:1 target ratio.
Overall, patients with IH had a 2.3-fold increased risk of an XFS diagnosis than control individuals (95% CI 1.4 to 3.5; p=0.03). Increased risk of XFS was not observed in patients with a direct IH (OR, 1.6; 95% CI 0.4 to 3.7; p=0.40). In contrast, patients with an indirect IH repair exhibited a 12-fold increased risk of an XFS diagnosis compared with matched control individuals; however, the estimate was imprecise (95% CI 4.0 to 38.7; p=0.002). These findings were based on a bootstrap resampling approach to provide more reliable estimates given relatively few XFS diagnoses. These were consistent with point estimates using an asymptotic (classic) conditional logistic regression model either adjusted for covariates or not. The model accounted for sex, age, body mass index (BMI) and smoking. The causes underlying the differential risk for direct and indirect IH with XFS observed in this study are unclear. However, direct and indirect IHs share abnormalities in connective tissue metabolism and genetic risk factors, but subtle variations in tissue histology, biomarkers and demographics suggest overlapping yet distinct pathogenic mechanisms.
Pelvic organ prolapse
POP, including pelvic floor disorders, affects the pelvic connective tissue of postpartum women. According to prevalence estimates, the reported range of symptomatic POP is 3%–11%.49 Surgical intervention is needed for approximately 11%–19% of women diagnosed with POP. Studies have shown that POP tends to run in families, correlates with elastin defects, and connective tissue repair abnormalities.50 51 Studies have also shown that there may be a genetic factor involved with POP.52 Both disorders may particularly share commonalities of the LOXL1 and elastin pathways.50 51 Emerging data regarding DNA methylation of LOX1 also reveals correlates between POP and XFS, as Zhang et al21 discovered a statistically significant and differential DNA methylation profile in a series of women with POP compared with controls.53
UPEXS study design and results for POP
The study focused on the relationship between POP and XFS and involved a 2-pronged approach using the UPDB. In substudy A, a cross-sectional analysis was done on 132 772 patient records of Utah women who were Medicare recipients for 3 or more years between 1992 and 2009. In substudy B, between 1 January 1995 and 31 December 2014, the longitudinal risk of an incident diagnosis of XFS was analysed of 5130 women between the ages of 30 and 65 years old at baseline, which all have been diagnosed with POP. This cohort was compared with 15 338 females controls that were age-matched and no history of POP. The results of these two studies were consistent with one another. In substudy A, the mean age of women was 82 years, and it was observed that POP was associated with a 56% increased risk of having a diagnosis of XFS (OR, 1.56; 95% CI 1.4 to 1.7). In the longitudinal analysis of substudy B, the incident risk of having XFS diagnosis was 48% greater in women aged 30–65 years with a diagnosis of POP compared with a control group of females that were age-matched without the diagnosis of POP over 20 years of follow-up (HR, 1.48; 95% CI 1.1 to 1.9). In both studies, the risk of being diagnosed with XFS was higher in women with a prior diagnosis of POP.
Obstructive sleep apnoea
OSA is a sleep disorder characterised by a partial or complete collapse of the upper airways while an individual is asleep, resulting in low airflow to the lungs and subsequent hypoxaemia and hypercapnia. OSA affects people of all ages, but the risk increases with age and obesity.54 Worldwide, this disorder affects 22% of men and 17% of women.55 However, some studies suggest the global prevalence of OSA is much higher.54 The severity of OSA is known to increase with a high BMI, age and male sex. Other risk factors that may play a role in incidence or severity include family history, smoking tobacco, alcohol abuse and menopause.56 Studies have shown an association between OSA and other systemic diseases such as AFib and hypertension.57 58
UPEXS study design and results for OSA
Using the UPDB, an OSA cohort was identified, consisting of individuals collected over an 18-year period (1999–2017). The OSA cohort consisted of 81 735 patients ages 50 through 90 years of age at the time of index diagnosis based on ICD-9 code 327.23 (OSA), or the ICD-10 code G47.33 beginning in October of 2015. A control group was randomly selected from the UPDB consisting of individuals without a diagnosis of any form of sleep apnoea. This group was individually matched based on age and sex in a 4:1 ratio to the OSA cohort. An XFS cohort of 2943 patients between ages 50 and 90 years diagnosed from 1996 to 2015 was previously identified with ICD-9 codes 365.52 (exfoliation glaucoma) or 366.11 (exfoliation of the lens capsule). A control group used for comparison was gathered with 14 713 subjects, each individually matched to the XFS group for sex and age in a 5:1 ratio. Each control subject was required to have a follow-up appointment in Utah at least as long as their respective matched study patient, based on the latest event recorded in the UPDB.
Conditional multivariable logistic regression models were used to calculate ORs to estimate the risk of XFS in OSA patients compared with their respective control groups. A model that included adjustment for covariables such as race, obesity, hypertension, tobacco use, AFib and COPD diagnosis history was also incorporated into the study. First-order interactions were examined between covariates potentially related to both XFS and OSA, including obesity, hypertension, tobacco use, AFib and COPD. The race was incorporated as a binary variable (non-white and white). Obesity was determined via the subjects’ BMI, categorised as non-obese (BMI<30), obese (BMI>30) or BMI not identified. Hypertension and tobacco use were both recorded as binary variables independent from one another. History of AFib and COPD was determined via ICD-9 codes in the subject’s medical records.
OR estimates for the covariate-adjusted model were done with a 95% CI and p values for the risk of having XFS on OSA patients overall, as well as in OSA patients with a history of hypertension compared with their respective matched control individuals. After accounting for matching variables of sex and age, and confounding variables such as race, obesity, AF, COPD, hypertension and tobacco use, we observed a slightly increased risk of XFS in patients with OSA overall (OR=1.27; 95% CI 1.02 to 1.59; p=0.03).
Atrial fibrillation
AFib is a common arrhythmia characterised by rapid and uncoordinated atrial depolarisation and myocardial contraction, leading to a higher risk of stroke and heart failure. AFib is the most frequent genetically influenced arrhythmia affecting approximately 9% of individuals over the age of 80% and 2% over 65.59 AFib is a complex disease process involving many structural changes at the atrial myocardium’s cellular level.60 Specific changes to the atrial myocardium have been observed, including fibrosis, dilation and hypertrophy. It has also been observed in other studies that abnormal levels of specific proteins that influence the ECM lead to disruption of the matrix’s homeostatic state. This disruption is believed to be caused by changes to the metabolic stability of elastin and collagen.
UPEXS study design and preliminary results for AFib
In a preliminary analysis, 2803 patients with XFS between 60 and 90 years old at the disease onset and a set of 43 694 patients diagnosed with AFib were examined. Conditional logistic regression was used to estimate the risk of AFib in patients diagnosed with XFS, compared with respective 5:1 sex-matched and age-matched non-XFS controls. Our pilot data indicate that patients with XFS appear to have a modest 20% increased risk of being diagnosed with AFib (p<0.01). In a preliminary Kaplan-Meier (KM) survival analysis, AFib patients with XFS appeared to survive longer than AFib patients with no history of XFS (p<0.0001). We plan to perform additional subgroup analyses and publish our final results.
UPEXS and survival patterns
In two separate studies, Slettedal et al and Svensson et al observed that individuals with XFS do not appear to have increased mortality and morbidity even when a possibly related life-threatening comorbidity is present.61 62 Given the size of this UPDB dataset, and the ability to determine morbidity and mortality in the UPEXS cohort, time to all-cause and disease-related mortality in the XFS was possible. Our UPEXS dataset included two patient cohorts, those with COPD and AFib, who had diseases known to increase morbidity and mortality. patients with COPD and age-matched control subjects with no history of COPD, stratified by XFS status, were analysed for time to death. KM survival curves were done separately for subjects between ages 50–69 years and subjects who were 70–90 years old at the time of diagnosis to reflect greater mortality risk inherent to the older group. In the age group 50–69 years, non-COPD controls with an XFS diagnosis had the highest survival rate over the 20-year study, with a 10-year survival of 91%. The control group with no XFS had lower survival rates overall, with a 10-year survival at 85%. In contrast, overall survival rates in the COPD group aged from 50 to 69 years were lower compared with their respective control group. However, patients with COPD with a history of XFS history had a notably higher survival rate than patients with COPD with no XFS (10-year survival of 76% and 43%, respectively). A similar trend was present in the 70–90 age group where the patients with XFS without COPD had the highest overall survival (59% at 10 years), followed by the patients without XFS nor COPD (10-year survival of 47%). Having COPD was associated with lower survival, generally, compared with controls. However, patients with COPD with XFS had higher survival rates than patients with COPD without XFS, with 10-year survival rates of 42% and 18%, respectively.
In a subanalysis of patients with COPD who were tobacco users, the survival rate was decreased compared with non-users. Having a medical history of XFS in tobacco-exposed COPD conferred a similar survival advantage. For example, for patients with COPD that use tobacco between the ages of 50–69, the 10-year survival rate of those with XFS was 70%, while the non-XFS subjects had a survival rate of 41%.
Discussion
This UPEXS work which used a very large dataset, the UPDB, has helped shed light on various systemic diseases that show an association with XFS. These data from the UPEXS help to support the hypothesis that shared pathogenesis and risk factors may exist as well as a triggering event, such as multiparity in the case of women with POP, tobacco use in COPD, and hypertension, and chronic mechanical stress in AFib patients. It is possible that tissue alterations containing elastin, which are regulated and repaired by enzymes such as LOXL1 are being affected by these triggering events and impacting disease pathogenesis. There are most likely other triggers and risk factors, perhaps epigenetic and environmental influences, that play a role in these relationships, as has been suggested by others in this field and may indeed involve LOXL1 as a risk gene.5 7 63 64 Ultimately the information gained from these UPEXS studies may help reshape our understanding of the role XFS plays in identifying other systemic disorders. Future efforts include an update to the UPEXS to include five additional years of historic data for carefully phenotyped XFS with comprehensive clinical values, comorbid conditions shown or hypothesised to be associated with XFS, as well as information on UV exposure. With this information, predictors of conversion of XFS to exfoliation glaucoma including mild and severe glaucoma outcomes maybe determined thus helping to identify those individuals at greatest risk for vision loss.
In conclusion, additional studies are needed to confirm these UPDB-based results and validate UPEXS results in other populations to continue to elucidate the role XFS plays in associated systemic conditions. Diagnostic coding via the ICD-9 codes can be inaccurate. To address this limitation, we randomly selected 540 medical records on 1901 patients with a diagnosis of XFS from 1996 to 2012 using ICD-9 which confirmed over 90% of our medical records. We are confident that the data presented here, and the current studies being performed using the UPDB population resource will improve our understanding of XFS, its clinical phenotype and associated comorbid diseases. This can help lead to referrals more accurate diagnosis, management, and improvement in earlier identification of diseases associated with XFS and better help identify common risk factors, environmental factors and demographics thus ultimately impacting patients’ outcomes.
Data availability statement
Data are available in a public, open access repository. Data are available upon reasonable request. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Approvals to conduct this study were obtained from the University of Utah Institutional Review Board (00081512) and the Utah Resource for Genetic and Epidemiologic Research, which governs research use of the UPDB, and study investigators adhered to the principles of the Declaration of Helsinki.
Acknowledgments
We gratefully acknowledge donors to the National Glaucoma Programme of the BrightFocus Foundation for their generous support (award G2020317). We thank the Pedigree and Population Resource of Huntsman Cancer Institute, the University of Utah (funded in part by the Huntsman Cancer Foundation) for its role in the ongoing collection, maintenance and support of the Utah Population Database (UPDB). We also acknowledge partial support for the UPDB through grant P30 CA2014 from the National Cancer Institute, University of Utah, and from the University of Utah’s programme in Personalised Health and Centre for Clinical and Translational Science (CCTS). We also thank the University of Utah CCTS (funded by NIH Clinical and Translational Science Awards), the Pedigree and Population Resource, University of Utah Information Technology Services, and Biomedical Informatics Core for establishing the Master Subject Index between the Utah Population Database, the University of Utah Health Sciences Centre. Research was supported by the NCRR grant, 'Sharing Statewide Health Data for Genetic Research' (R01 RR021746, G. Mineau, PI) with additional support from the Utah Department of Health and the University of Utah.
References
Footnotes
Contributors All authors had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: KC, BMW, CJP. Acquisition, analysis or interpretation of data: all authors. Drafting of the manuscript: KC, CShumway, CSwiston, MC, ST, CP, DJB, BMW, CJP. Critical revision of the manuscript for important intellectual content: BMW. Statistical analysis: KC. Obtained funding: BMW. Administrative, technical or material support: KC, BMW. Supervision: BS, RR, BMW.
Funding Funding for this study was provided by donors of National Glaucoma Research, a programme of the BrightFocus Foundation (Award G2020317) and an unrestricted institutional grant from Research to Prevent Blindness, Inc., New York, New York to the John A Moran Eye Center, University of Utah. Sam Taylor and Chase Paulson received grant support from RUUTE (Rural and Underserved Utah Training Experience), a programme to improve healthcare access and longitudinal socioeconomic benefit for underserved communities of Utah, Idaho, Montana and Wyoming. Support for the Utah Population Database was provided by Cancer Center Support Grant from the National Cancer Institute (P30 CA2014), an NCRR grant, 'Sharing Statewide Health Data for Genetic Research' (R01 RR021746, G. Mineau, PI) with additional support from the Utah Department of Health and the University of Utah.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.