Article Text

Abstract
Objective To estimate prevalence and causes of blindness and vision impairment and assess cataract surgical coverage and quality of cataract surgery in Kabul.
Methods and analysis A total of 3751 adults aged 50 years and above were recruited from 77 randomly selected clusters. Each participant underwent presenting and pinhole visual acuity assessment and lens examination. Those with pinhole visual acuity <6/12 in either eye had a dilated fundus examination to determine the cause of reduced vision. Those with apparent lens opacity were interviewed on barriers to cataract surgery.
Results The age-adjusted and sex-adjusted prevalence of blindness was 2.4% (95% CI: 1.8% to 3.0%). Prevalence of severe, moderate and mild vision impairment was 2.2% (95% CI: 1.7% to 2.7%), 6.9% (95% CI: 6.0% to 7.9%) and 8.7% (95% CI: 7.5% to 9.8%), respectively. Cataract was the main cause of blindness (36.8%), severe (54.4%) and moderate (46.1%) vision impairment. Uncorrected refractive error was the leading cause of mild vision impairment (20.3%). Age-related macular degeneration was the second leading cause of blindness (23.0%). In people with a presenting visual acuity of <3/60, cataract surgical coverage was 89.7%, and effective cataract surgical coverage was 67.8%. The major barriers to uptake of the available cataract surgical services were the need for surgery was not felt (23.7%) and cost (22.0%).
Conclusion Kabul province has a high prevalence of blindness, largely due to cataract and age-related macular generation. The quality of cataract surgery is also lagging in terms of good visual outcomes. This calls for immediate efforts to improving the reach and quality of existing eye services and readiness to respond to the increasing burden of posterior eye disease.
- epidemiology
- vision
- public health
Data availability statement
Data are available upon reasonable request. data are stored in RAAB repository, available in reasonable request. https://raabdata.info/repository.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key message
What is already known about this subject?
Rapid Assessment of Avoidable Blindness (RAAB) was conducted in three provinces, Herat, Badakhshan and Laghman, outside of Kabul.
What are the new findings?
The current study is the first RAAB in Kabul province. It showed blindness rate as over 2%; the leading causes were cataract and age-related macular degeneration.
How might these results change the focus of research or clinical practice?
These finding would help the policy makers to formulate adequate eye health policy and resource allocation.
Introduction
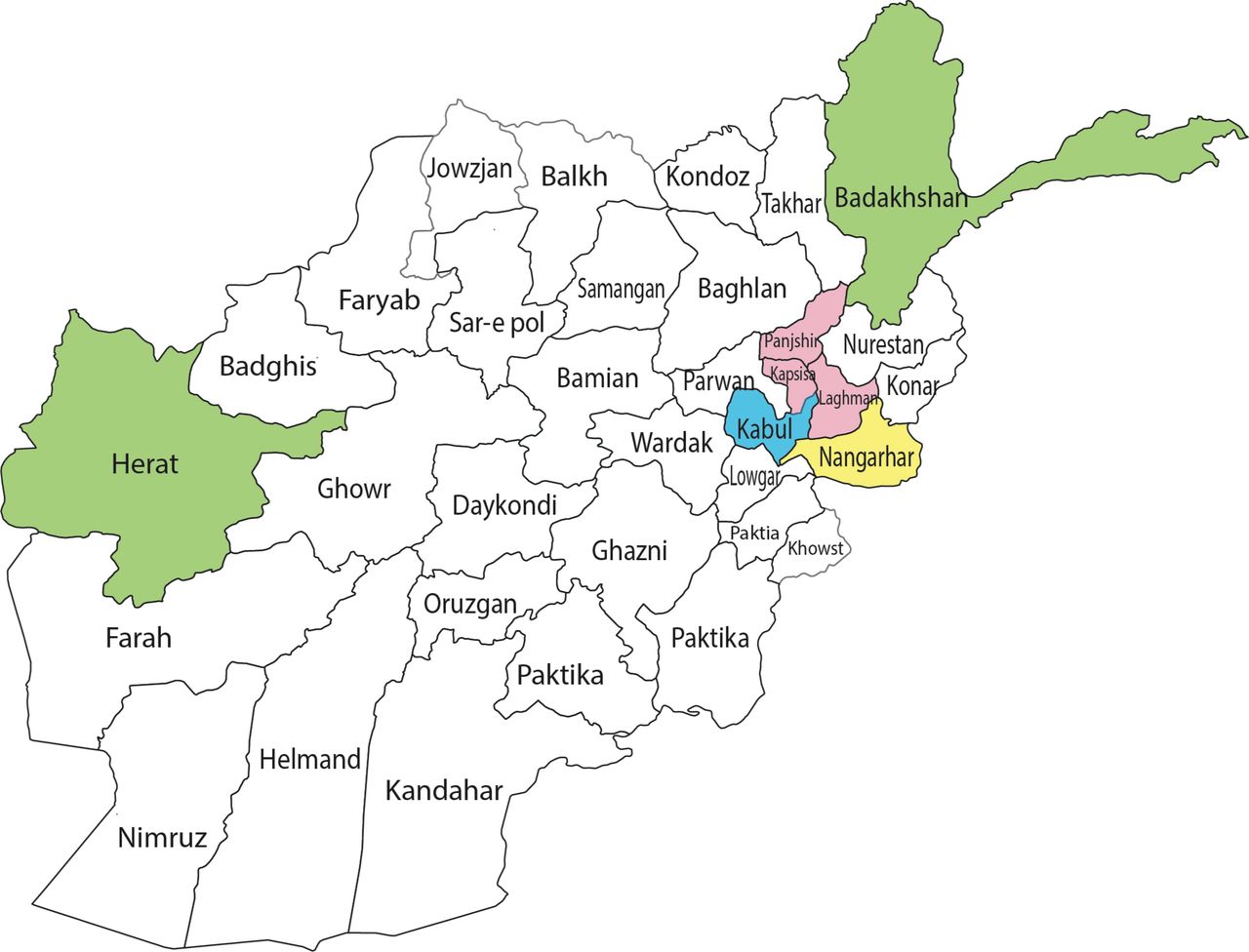
The 66th World Health Assembly endorsed the Universal eye health: A global action plan 2014–2019, which set a target to reduce the prevalence of blindness and vision impairment by 25% between the years 2010 and 2019.1 The first mandate of the global action plan (GAP) is to generate evidence on the magnitude and causes of blindness and vision impairment in signatory countries; this evidence can monitor progress towards achieving the GAP targets and advocate for greater political and financial commitment in eye health. The GAP strongly recommends implementing population-based surveys that estimate the prevalence of blindness and vision impairment in the vulnerable elderly population.2 Rapid Assessment of Avoidable Blindness (RAAB) surveys have been conducted in Afghanistan in the past. Three provinces were surveyed in 2010 (Badakhshan, Heart and Laghman), while Jalalabad city and four surrounding districts in Nangarhar province were surveyed in 20153–5 (figure 1). However, a RAAB survey has not yet been conducted in Kabul, the capital city of Afghanistan, nor in Kabul Province.

{kind=link}
Map of Afghanistan where provincial RAAB surveys were conducted in 2010–2015 and 2018.
In Afghanistan, primary eye care services are available at district and province capital hospitals, and a resident ophthalmologist provides eye care services at secondary-level hospitals. Dedicated eye care units are located at seven regional hospitals; public tertiary-level eye hospital services exist in Kabul (capital city) only.
The primary aim of the current study was to estimate the prevalence and main causes of blindness and vision impairment in people aged 50 years or older in Kabul province, Afghanistan. The study also determined the proportion of people with impaired vision due to cataract receiving the required cataract surgery and visual outcome after such surgery.
Methodology
This was a cross-sectional population-based survey. The survey methodology followed the standard RAAB survey protocol.6
Definitions
Blindness and vision impairment were classified as per the WHO standards.7 Mild vision impairment was defined as a presenting visual acuity (PVA) of <6/12–6/18, moderate vision impairment (MVI) as a PVA of <6/18–6/60, severe vision impairment (SVI) as a PVA of <6/60–3/60 and blindness as a PVA of <3/60. Cataract surgical rate, the measure of the quantity of cataract services, was defined as the number of cataract operations performed in 1 year per million population.8 Cataract surgical coverage (CSC) was defined as the proportion of patients or eyes with operable cataract who had already received surgery; it measures the impact of existing cataract services.9 Effective cataract surgical coverage (eCSC), which combines CSC with postoperative vision outcomes, was defined as the number of people who had undergone cataract surgery and achieved a good outcome (PVA ≥6/18) as a proportion of those having operable plus operated cataract.10
Sample size and selection
According to the Central Statistical Organization (CSO), the total population of Kabul province is 4 679 648 (CSO 2017); of these, 3 984 343 (1 949 852 females and 2 034 491 males) live in urban areas and 695 305 (338 194 females and 357 111 males) live in rural areas. Kabul city has a population of 3 961 487 people. The previous RAAB survey report (unpublished) in other provinces shows that the prevalence of blindness is 3%–8%. The required sample for the current survey was estimated to be 3820 people aged 50 years or older; this was based on an estimated prevalence of blindness of approximately 4%, at 95% CI with a relative precision of 20%, design effect of 1.5 for cluster sampling and assuming 10% dropout rate. RAAB V.6 software (London School of Hygiene & Tropical Medicine, UK) was used to calculate the sample size. Based on CSO 2017 population data,11 approximately 12% of the population in Afghanistan is aged 50 years or older. Therefore, a population unit of 450 people was needed to obtain 50 people aged 50 years or older in each population unit. Kabul province was therefore divided into 5006 population units (clusters), with each comprising at least 450 people. We enrolled 3850 people in 77 randomly selected clusters in Kabul province to achieve the required sample size.
Survey teams
Three RAAB teams, each consisting of one ophthalmologist and one ophthalmic technician, received the standard 5-day RAAB training from a certified RAAB trainer. The training included measuring VA using a tumbling E chart, performing an external examination of the eye and crystalline lens using a flashlight and slitlamp, and determining the leading cause of vision impairment. At the end of the training, the interobserver variation (IOV) was determined among the three teams. Data collection was also piloted under the supervision of the trainer in a non-study cluster; this provided an opportunity for the survey team to practice all aspects of data collection, including quality assurance steps.
The enrolment of eligible survey participants and data collection were carried out door-to-door in the selected study clusters. PVA was assessed in each eye using a tumbling E chart. Pinhole visual acuity, or best-corrected visual acuity (BCVA), was checked if PVA was <6/12. Clinical examination of the anterior segment was performed using a flashlight, and assessment of media clarity and fundus examination were performed by direct ophthalmoscopy. If BCVA was <6/12 in either eye and could not be explained by lens opacity, the participant’s pupils were dilated with 1% tropicamide, and direct ophthalmoscopy was performed indoors or in a shaded area to determine the cause of reduced vision. If a participant needed cataract surgery, reasons for not having had surgery were elicited. If a participant had received cataract surgery, surgery details and outcomes were recorded.
Data collection
The data were recorded on smartphones using the mRAAB application (V.1.30, Peek Vision, UK). The data entered using a smartphone were transferred to a computer server via email at the end of a cluster visit or when the internet connection for the field team was available. The data collection was paperless, and the mRAAB software was designed to notify the survey team of any data inconsistency or incomplete data. The study coordinator also performed an additional consistency check, and inconsistencies were corrected on the same day, if any.
Informed consent was obtained from all participants at the time of enrolment and before the examination. An appropriate referral was made when the teams came across participants who needed follow-up at a healthcare facility.
Statistical analysis
The RAAB V.6 software was used to generate study reports once all cluster data collection was completed.
Patient and public involvement
Before the enrolment and examination, all eligible participants were explained the study procedures including the benefits to each participant in their local dialect by the enumeration team. Written informed consent with signature or inked fingerprint was obtained stating their acceptance to voluntarily participate in the study and permit use of the data for publication. No financial incentives were provided for participation in the study.
Results
The IOV κ (Kappa) for the team was 0.72 for VA measurement, 0.82 for lens examination and 0.78 for assigning cause for vision impairments; all κ values were greater than the RAAB recommendation of 0.6. Data collection took place from June to September 2018.
In this survey, a total of 3751 people received vision assessment and eye examination out of 3850 enrolled, the overall response rate was 97.4%. Forty people were not examined, 19 people (12 males and 7 females) refused to participate, and 21 people (11 males and 10 females) did not provide informed consent.
Prevalence of blindness and vision impairment
The age-adjusted and sex-adjusted prevalence of blindness was 2.4% (95% CI: 1.8% to 3.0%). Prevalence of blindness was higher in females at 2.9% (95% CI: 2.1% to 3.6%) than males at 1.9% (95% CI: 1.2% to 2.6%), but this difference was not statistically significant (OR: 1.0, 95% CI: 0.7 to 1.6, p=0.8). The age-adjusted and sex-adjusted prevalence of SVI, MVI and early vision impairment was 2.2% (95% CI: 1.7% to 2.7%), 6.9% (95% CI: 6.0% to 7.9%) and 8.7% (95% CI: 7.5% to 9.8%), respectively and was higher in females in all categories of vision impairment (table 1).
Age-adjusted and sex-adjusted prevalence of blindness, SVI, MVI and EVI in Kabul province and estimated number of cases
Extrapolating the blindness prevalence to the total population aged 50 years and older in Kabul province suggests that 82 847 people had some degree of vision impairment, and 9847 were blind in the province (table 1).
Blindness increased significantly with advancing age, from 0.7% in the 50–59 age group to 14.8% in 80 years and older age group (p<0.01), and it was higher in females than males in each age group (online supplemental table 1).
Supplemental material
Causes of blindness and vision impairment
Cataract was the most common cause of blindness, SVI and MVI; the uncorrected refractive error was the most common cause of mild visual impairment. Age-related macular degeneration (ARMD) was the second leading cause of blindness (23.0%), as well as of SVI (11.4%), and the third leading cause of MVI (13.0%) (table 2).
Causes of blindness and VI
Prevalence of cataract and CSC
The age-adjusted and sex-adjusted prevalence bilateral cataract among people with blindness and SVI, was 0.7% (95% CI: 0.4% to 1.0%), and 1.5% (95% CI: 1.0% to 2.0%), respectively. Using these prevalence figures, we estimated the number of people affected by cataract at different levels of vision impairment in Kabul province. We estimated that 2778 people who are blind (VA <3/60) and 6148 people with SVI (VA <6/60) had bilateral cataract (table 3).
Age-adjusted and sex-adjusted cataract prevalence and extrapolated numbers
CSC among people with blindness, SVI, and MVI, was 89.7%, 67.3%, and 63.4%; eCSC was lower, at 67.8%, 54.1%, and 47.6%, respectively (table 4).
Cataract surgical coverage and eCSC
Vision outcome of and barriers to cataract surgery
Ten of 469 (2.1%) eyes that had undergone cataract surgery did not receive an intraocular lens (IOL); it was planned extracapsular cataract extraction. Among those who received IOL, good postoperative PVA (≥6/18) was achieved in 69.0% of eyes, and good postoperative BCVA was achieved in 75.9% of eyes (online supplemental table 2).
Cataract surgery was performed in four types of facilities: private (45.6%), government (33.7%), charitable (19.8%) and eye camp (0.9%). Good outcome was found as 71%, 67.1%, 64.5%, 75% operated in private, government, charitable and eye camp, respectively. The major causes of poor outcome following cataract surgery were ocular comorbidities (43.2%) (mainly posterior segment problem such as age-related macular degeneration), long-term postoperative complications (38.5%) (eg, posterior capsular opacity and retinal detachment) and immediate surgical complications (12.2%) (eg, peaked pupil and endothelial decompensation). One would expect better visual outcome after cataract surgery with technical and technological advances in the recent years. But it was not the case in this study (online supplemental table 3).
Fifty-nine people stated their barriers to obtaining cataract surgery. The most commonly reported barriers were that a need for surgery was not felt (23.7%), cost (22.0%), fear (17.0%), ignorance about cataract surgery (17.0 %) and treatment deferred by providers (15.2%) (table 5). The most commonly reported barriers to receiving cataract surgery appeared to differ between males and females, with a greater proportion of females reporting that cost and deferral of treatment by providers were a barrier, compared with men (34.7% cf. 12.1% and 23.1% cf. 9.1%, respectively).
Barriers to cataract surgery among bilateral cataract blind (BCVA <6/60 due to cataract)
Refractive error and low vision
The prevalence of refractive error for distance in the study population was 12.7%. More than half (57.3%) of participants with the refractive error were not wearing spectacles. In this survey, we assumed all people age 50 years and over need reading glasses: only 7.8% of people were wearing near vision (presbyopia) correction at the time of examination.
Discussion
The study presented here is the first population-based survey of blindness and vision impairment in Kabul province of Afghanistan. There were two principal challenges in the planning and execution of this survey. These included: (1) women were reluctant to get examined by male eye health personnel, which could be overcome by consultations that involved the entire community; (2) the security risk related to ongoing strife in the country, with the government making provisions for adequate safety and security of all people involved in the survey to mitigate this risk. Female medical health workers, including a female ophthalmologist, should be included in future population-based studies to increase more female participation.
Despite these challenges, the first RAAB survey in Kabul region had a good response of 97.4%. We preferred the RAAB survey methodology to an all-age population survey because RAAB is relatively fast and inexpensive.12 The information obtained from the RAAB survey, such as the prevalence and causes of blindness, CSC and visual outcome following cataract surgery, indicates the state of existing eye care services and is important for decision-makers to coordinate, promote and deliver high-quality, sustainable eye care services.2 This information is also important to assess the need for eye care infrastructure, human resources development, and quality assurance in eye care.
In this survey, we found an age-adjusted and sex-adjusted prevalence of blindness of 2.4%. The survey also suggested that the prevalence of blindness in the capital city, where 85% of the population live, was comparable to that in rural. This finding is surprising, given that health services in Afghanistan tend to be of higher quality in urban areas than rural areas. This is also in contrast to evidence from many other comparable economy countries, where healthcare is usually better in the urban areas than rural areas because of easy availability and accessibility of care and eye health personnel.13 Primary eye care services are only available at district and province capital hospitals in Afghanistan, and resident ophthalmologists provide eye care services in isolation at secondary-level hospitals. Dedicated eye care units are only available in seven regional hospitals, and public, tertiary-level eye hospitals only exist in Kabul. Primary-level services are better in other provinces than Kabul; the secondary and tertiary eye care services are considerably better in Kabul than in other regions and provinces.
The prevalence of blindness in Kabul is comparable to the prevalence in the other three provinces where RAAB surveys have been conducted in the past (Herat, Badakhshan and Laghman); however, the prevalence of SVI and MVI was higher in the other three provinces. We compared the results of the current RAAB with the earlier three RAABs and the publications by the Global Burden of Disease study group (online supplemental table 4). Uncorrected refractive error was the most common cause of MVI in all provinces except in Badakhasan province (2010 RAAB); untreated cataract was the leading cause of blindness and SVI in all four provinces; trachoma was mostly detected in Badakhshan province, and ARMD was mostly detected in Kabul province.
Geographically, Afghanistan is located in the Eastern Mediterranean (South-Central Asia). This region has 22 countries with a total population of 679 million14 and an age-standardised prevalence of blindness of 1.5% (2015 estimate).15 These countries are not uniform in terms of lifestyle, gross domestic product and socioeconomic status—more so at times of uncertainty of war and internal conflicts.16 17 Afghanistan is a low-income country with a low human development index (0.498) and is ranked 168th in the world.18 In this economic situation, it is expected that the healthcare system would not be robust. This could also vary from one province to another, and indeed it is reflected in the differences in the blindness prevalence and vision impairment between the four RAABs in the last decade. Data from the present study are comparable to data from the Vision Loss Expert Group report from central Asia.15
The current RAAB clearly shows that CSC, eCSC and post cataract surgery outcome do not measure up to the WHO targets. These indicators have also not improved in the past decade, despite recent advances in the techniques and technology for cataract surgery. While fear of surgery and low health literacy are the traditional barriers to cataract surgery, affordability in 22% of people is a matter of concern.
The study also found a large burden of ARMD. Unlike cataract surgery or refractive error correction, treatment of macular degeneration needs a very large resource investment in diagnostic equipment, trained personnel and cost of treatment. The Afghanistan eye health system should gear up to this need. These investments would also be essential for other posterior segment care, most importantly, diabetic retinopathy. Incidentally, the current RAAB did not detect a large number of people with diabetic retinopathy, but the current study was not specifically designed to detect diabetes mellitus and/or diabetic retinopathy.
The prevalence of uncorrected refractive error and uncorrected presbyopia was high. Only 43% of people with distance vision impairment due to refractive error were wearing spectacles. Only 7.8% of people aged 50 and above were using presbyopic correction.
So, where should Afghanistan focus efforts when it comes to eye care? Since the cost–benefit is higher in cataract surgery and refractive error correction compared with other eye health conditions, the health system in the country could be directed to improve the quantity and quality of cataract surgery and support the provision of affordable spectacles as a first step. A strategy to develop eye health personnel and resources for other eye conditions such as glaucoma, diabetic retinopathy and ARMD should also be put in place. The current RAAB results will help inform these country-specific responses to eye care needs.
Data availability statement
Data are available upon reasonable request. data are stored in RAAB repository, available in reasonable request. https://raabdata.info/repository.
Ethics statements
Patient consent for publication
Ethics approval
The study confirmed to the tenets of the Declaration of Helsinki. The protocol was reviewed, and the Institutional Review Board (IRB), Ministry of Public Health, Islamic Republic of Afghanistan (Ref. No. 444504, dated 4 April 2018) approved to carry out in Kabul province of Afghanistan.
Acknowledgments
We are grateful to Health Net TPO Afghanistan team for logistics and financial management to support this survey work. Thanks also goes to survey supervisor Dr Sayed Jalal Pashtoon, study ophthalmologists Dr Qais Nasimee, Dr Shabir Muez and Dr Abeebullahh Asadi for challenging field work for data collection of this survey. We are also grateful to all people of Kabul for their cooperation and participation in this survey.
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All author contributed on manuscript preparation and research design. NN, AMS, MN, ASS, AuR, YS further contributed to data acquisition and analysis. FD'E, TD and YS contributed to data interpretation.
Funding This research was funded by Fred Hollows Foundation, Australia.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.