Article Text

Abstract
Objective To describe a cluster of symptomatic intravitreal silicone oil (SiO) droplets following intravitreal injections (IVIs) and assess the effect of switching to a SiO-free syringe.
Methods and analysis Observational quality registry study of patients receiving IVI at a large Norwegian ophthalmology centre between April 2018 (start of cluster) and November 2019 (1 year after switching to SiO-free syringes). At onset, anti-vascular endothelial growth factor drugs were administered using SiO-containing insulin syringes. From November 2018, SiO-free syringes were implemented. Spontaneously reported symptomatic SiO cases were confirmed by slit-lamp examination. A follow-up interview was performed after 1 year, assessing visual complaints. The prevalence of non-symptomatic cases was assessed in a sample of 50 eyes from 50 consecutive IVI patients.
Results Among 13 429 IVIs, 50 eyes of 46 patients (29 women) with symptomatic intravitreal SiO droplets were identified. Forty-one patients reported floaters at regular appointments, whereas five patients contacted the department regarding symptoms between scheduled appointments. After 1 year, 34 patients (79%) still experienced floaters, 21 (49%) reported reduced symptoms and 3 (7%) reported worsened symptoms. Eighteen patients (42%) reported being bothered, and eight (18.6%) reported that their lives were negatively affected by the floaters. Among 50 non-symptomatic eyes that had received IVI during the same period, intravitreal SiO was found in 34 (68%). No cases of symptomatic intravitreal SiO droplets were identified after switching to SiO-free syringes.
Conclusion Symptomatic intravitreal SiO following IVI can cause significant and prolonged distress for affected patients. It can be avoided by using SiO-free syringes.
- macula
- neovascularisation
- retina
- vitreous
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Floaters due to intravitreal silicone droplets are a potential complication of intravitreal injections and have been recognised since the beginning of the anti-vascular endothelial growth factor era.
What are the new findings?
We here report on a large cluster of cases that appeared during a half-year span.
Follow-up interviews after 1 year revealed continued symptoms and distress.
A change to silicone oil-free syringes eliminated the problem: no new cases appeared during 1 year of monitoring.
How might these results change the focus of research or clinical practice?
We strongly recommend the use of silicone oil-free syringes for intravitreal injections.
Introduction
In the era of anti-vascular endothelial growth factor (anti-VEGF) inhibitors, intravitreal injections (IVIs) have become one of the most commonly performed ophthalmic procedures.1 Deposition of intravitreal silicone oil (SiO) has been observed since the beginning of anti-VEGF therapy but received limited attention in the early literature.2 3 More case series have been published in recent years.4–7 This adverse effect seems to occur in clusters, possibly attributable to specific syringe production batches or injection techniques.4 8 Despite the evident risk of depositing intravitreal SiO, syringes containing SiO lubricant remain popular, and neither guidelines nor drug label recommendations advise against their use.9 10
In mid-2018, IVI patients in our clinic started reporting persisting floaters after their last IVI. Slit-lamp examination revealed SiO droplets in the vitreous body, presumably derived from the syringes. These syringes had been used for several years prior without similar incidents. Changing the syringe batch failed to solve the problem, and ultimately a switch was made to SiO-free syringes.11
The aims of this study were to determine the extent of the cluster, assess patient-reported outcomes after 1 year, determine the prevalence of non-symptomatic SiO and evaluate the effect of shifting to SiO-free syringes for IVI.
Materials and methods
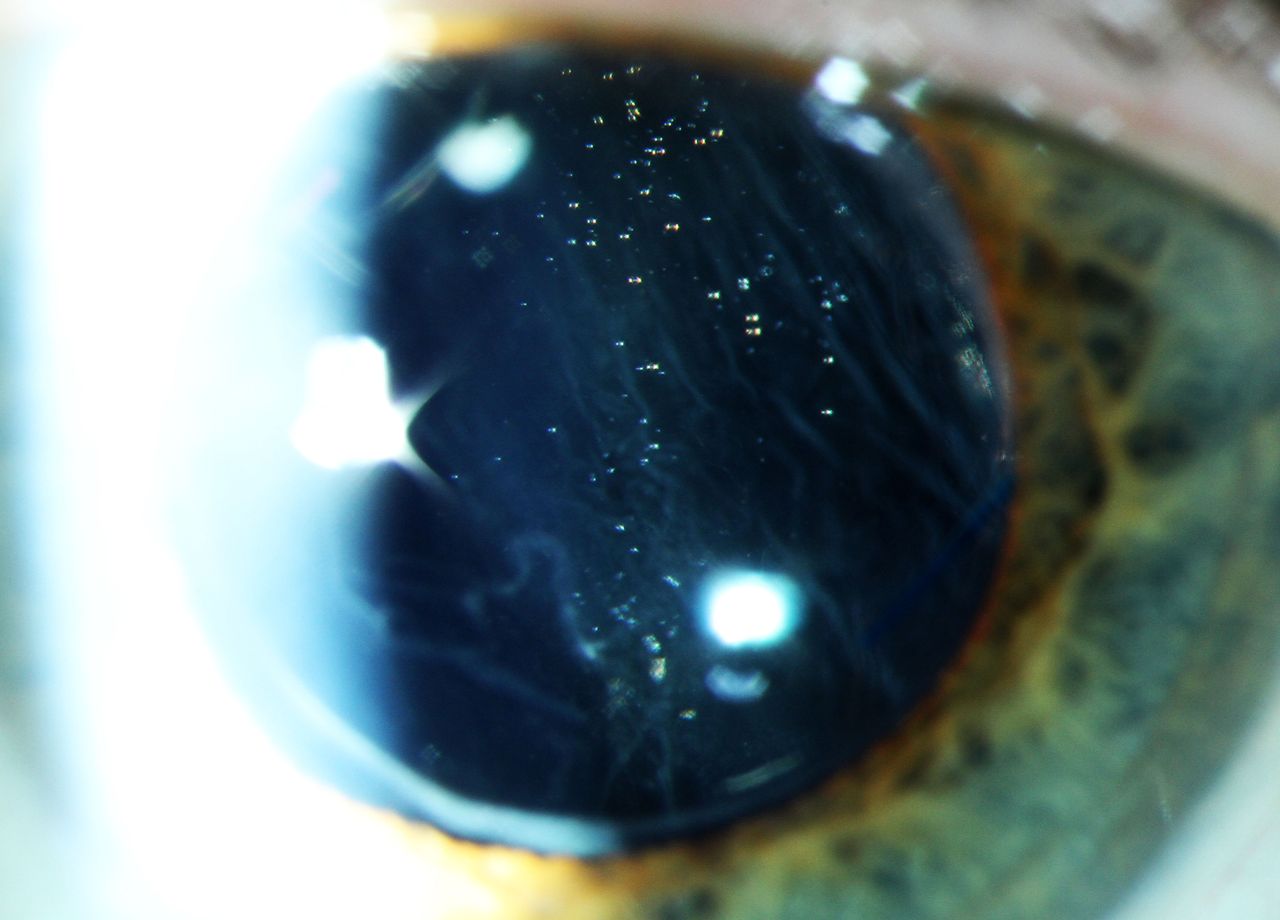
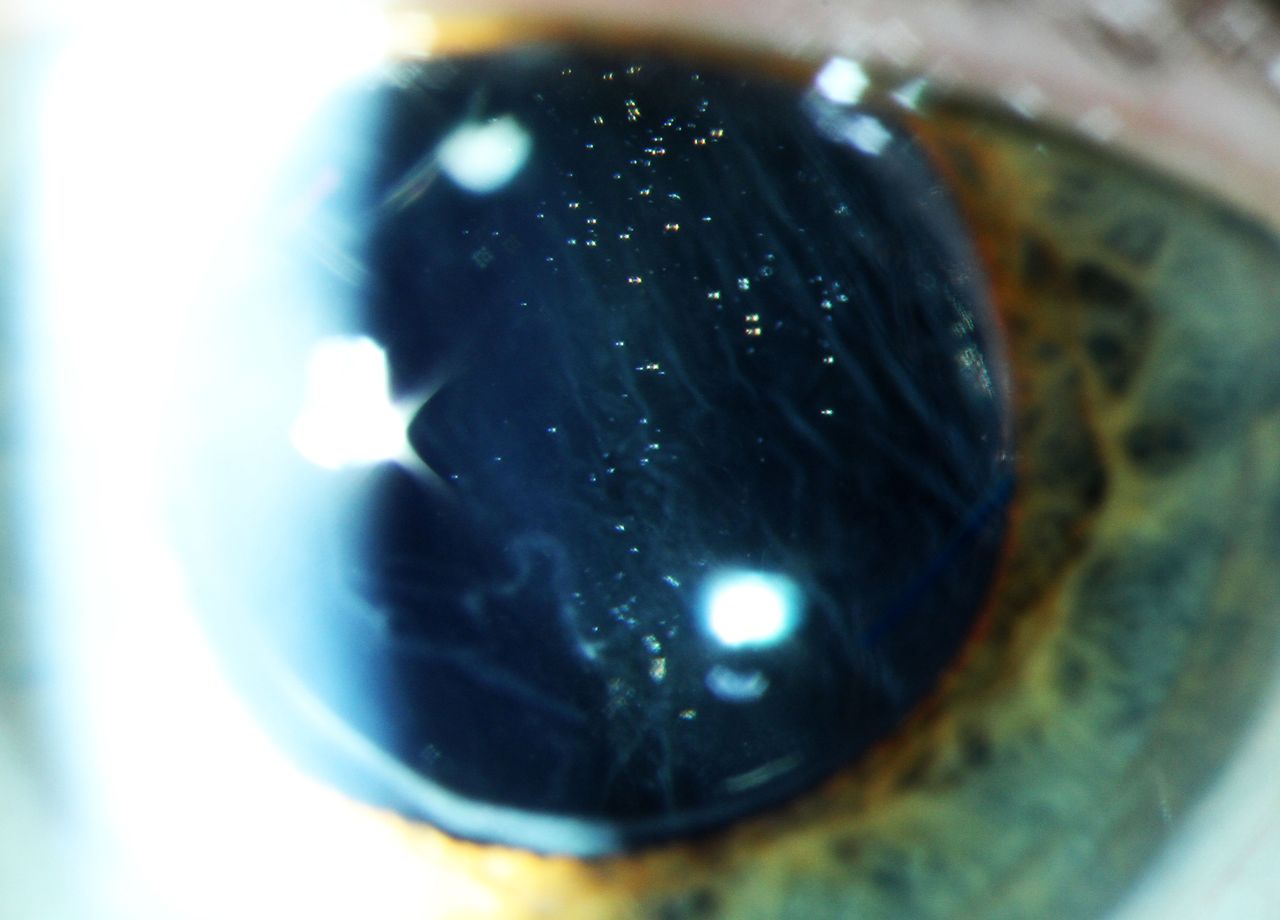
The study was conducted as an observational quality registry study. It took place at the Department of Ophthalmology, Oslo University Hospital, Norway. The inclusion criteria were: (1) persisting floaters after an IVI, reported spontaneously, that is, without being asked about floaters; (2) transparent spheres in the vitreous cavity consistent with SiO droplets (figures 1 and 2); (3) at least one IVI performed between April 2018 (start of the cluster) and November 2019 (12 months after shifting to a SiO-free IVI procedure). In our department, IVIs are performed using injection-ready syringes compounded at our hospital pharmacy. The compounding method is identical for all anti-VEGF agents used in the department: bevacizumab (Avastin, Roche), aflibercept (Eylea, Bayer) and ranibizumab (Lucentis, Novartis). From March 2016 to November 2018, the IVI procedure used insulin plastic syringes with SiO coating and a staked-on needle (BD Micro-Fine Plus, 0.5 mL, 30 G, 8 mm, Becton, Dickson and Co, Franklin Lakes, USA).12 In November 2018, it was replaced with a SiO-free syringe (Injekt-F, 1 mL, B Braun, Melsungen, Germany) and a low dead space needle hub 33 G×9 mm needle (TSK Laboratory, Tochigi, Japan).11

Wide-field retinal image of the right eye of a patient with branch retinal vein occlusion who complained about floaters after the very first anti-VEGF injection. The patient had no posterior vitreous detachment, and intravitreal silicone droplets could be seen in front of the retina, scattered over much of the upper hemisphere. VEGF, vascular endothelial growth factor.
{kind=link}
{kind=link}
Slit-lamp photograph of the left eye of a pseudophakic patient with posterior vitreous detachment, who complained about persistent floaters following an intravitreal injection. A large number of silicone oil droplets can be seen just behind the artificial lens.
Twelve months after the middle of the cluster (mean interval: 346 (±57) days after the SiO-causing injection), a telephone survey to all affected patients was conducted, using the following questions: (1) Do you still see floaters?; (2) If no, when did the floaters disappear?; (3) If yes, have the floaters improved or worsened?; (4) Are you bothered by them?; (5) Do they negatively affect your life?
Relevant patient information was collected from the patient records, including best corrected visual acuity (BCVA), total number of IVIs (until 12 November 2018) and number of IVIs during the outbreak period. We defined the ‘outbreak period’ as 6 April–12 November 2018, corresponding to the first and last SiO-causing IVI in the cluster.
To further evaluate the extent of the problem, 50 eyes of 50 consecutive IVI patients without floater complaints were evaluated for intravitreal SiO. These examinations were performed in connection with regular appointments. We included patients who had: (1) at least one IVI between April and November 2018; (2) no complaints about floaters.
Statistics
The Student’s t-test was used to compare means when variables were normally distributed, otherwise the Mann-Whitney U test was used. Distributions were compared using the Fisher’s exact test. Statistical analyses were performed with SPSS (V.25, IBM). Statistical significance was set at p<0.05. Distributions are presented as mean (±SD) or median (range).
Patient and public involvement
It was not appropriate to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Symptomatic patients
Fifty eyes of 46 patients (29 women) with spontaneously reported floaters and intravitreal SiO after IVI were identified. The patients described the floaters as clouds of small round dots, flies, pearls or diamonds or, in a few cases, as one or a few large bubbles. The SiO droplets were usually found in close proximity to the posterior vitreous membrane, either preretinally (figure 1) in patients without posterior vitreous detachment or just behind the lens (figure 2) in patients with complete posterior vitreous detachment. Mean age was 73 (±13) years. All IVIs associated with symptomatic SiO were performed between 6 April and 12 November 2018. During this period 13 429 IVIs were performed. Median time from the IVI-causing floaters to diagnosis of intravitreal SiO was 67.5 (11–267) days. Forty-one patients (89%) reported floaters in connection with a scheduled visit, while five patients (11 %) contacted the department between appointments to report on floaters. Of the 46 included patients, 43 (94%) completed the telephone survey. Thirty-four (79%) reported persistent floaters. Patients who no longer perceived floaters had stopped seeing them after a mean of 234 (±57) days. Twenty-one (49%) experienced improvement in symptoms, whereas three (7%) reported worsening. Eighteen (42%) were bothered by the floaters, and eight (19%) responded that the floaters negatively affected their lives. In November 2018, a change was made to syringes without SiO coating. During 12 additional months of follow-up (until November 2019), no new cases of symptomatic SiO were identified.
Comparison with non-symptomatic patients
Among the 50 consecutive patients without reported floaters, intravitreal SiO was found in 34 of 50 examined eyes (68.0%). The presence of intravitreal SiO was not related to total number of IVIs (mean without SiO 25.7 (±18.9) vs 34.3 (±29.8) with SiO; p=0.447) or IVI during the outbreak period (4.5 (±2.1) without vs 4.5 (±2.0) with; p=0.983). We also compared characteristics of the non-symptomatic patients with documented SiO with the symptomatic patients in the outbreak (table 1). The symptomatic patients were younger (mean age 72.7 (±13.0) vs 81.2 (±8.8) years; p<0.001) and had received fewer IVIs (20.6 (±16.7) vs 34.3 (±29.8); p=0.033) than the non-symptomatic patients. The difference in age persisted when looking only at patients with neovascular age-related macular degeneration (AMD) (mean age 78.3 (±7.2) vs 84.1 (±6.0) years; p=0.002). There were no statistically significant differences in BCVA, number of injections during the outbreak period, gender ratio or distribution of diagnoses between the two groups.
Comparison between the symptomatic patients with silicone floaters identified during the outbreak period and the 34 non-symptomatic patients where intravitreal silicone was found in the examined eye among 50 non-symptomatic consecutive patients investigated (Non-symptomatic)
Discussion
We describe a large cluster of floaters caused by intravitreal SiO following IVI. During this cluster, 6.3 patients were identified per month, usually at the next appointed visit after the IVI but sometimes after a concerned phone call from the patient. After switching to SiO-free syringes, no new cases were identified.
Overall, IVI has proven to be a relatively safe procedure. The most concerning complication, post-injection endophthalmitis, has an incidence of about 0.1 per 1000 IVIs in our clinic.13 14 Floaters caused by intravitreal SiO are certainly less devastating than bacterial endophthalmitis but as evident from this study, they still may create considerable discomfort. It is concerning that in the follow-up interview after 1 year, nearly 80% of included patients reported persisting floaters and almost 20% reported that the floaters negatively impacted their lives. Traditionally, intravitreal deposition of SiO has received little attention, but in recent years increasing numbers of case series have been published.4 6 10 15 Khurana et al4 found long-term symptoms in only 12% of patients and speculated as to whether SiO migrated out of the visual axis or patients gradually adapted to their presence. By contrast, 79% of the patients reported persisting symptoms in our material. This difference may be methodological; we performed a follow-up interview to specifically address whether patients still experienced floaters, whereas Khurana et al4 conducted a retrospective study, which presumably was based on medical records.
Our investigation of 50 consecutive non-symptomatic patients revealed a very high prevalence (68%) of intravitreal SiO droplets, closely matching a prevalence of 67.57% found in another study.5 The much lower percentage (1.3%) who spontaneously reported floaters shows that most cases of intravitreal SiO are not reported as floaters. The explanation may be that the patients do not experience floaters, or that they see them but do not report them. Hopefully, the former explanation is the most common, but this cannot be gauged directly from our data, as we did not routinely ask patients about floaters. As to why intravitreal SiO only causes floaters for some, but not all patients, we can only speculate. Presumably, the explanation relates to both the amount and position of SiO within the vitreous body. The visual acuity does not seem to be important, since our material shows no difference in BCVA between symptomatic and non-symptomatic patients with intravitreal SiO. We did, however, find a difference in age; symptomatic patients were on average 8.5 years younger than non-symptomatic. The difference in age but not BCVA may indicate age-dependent differences in perception, that elderly patients have lower demands concerning visual quality, or that they are less likely to complain. Notably, some non-symptomatic patients had surprisingly large amounts of intravitreal SiO, which presumably would have been reported as floaters by other patients. It is known that both the perception and degree of nuisance from floaters are influenced by psychological factors,16 17 which is why we routinely avoid asking IVI patients about floaters. Asking about floaters may otherwise give rise to a problem the patient did not have before being asked about it.
Previous studies have concluded that the origin of intravitreal SiO following IVI is the SiO lubricant used to reduce friction between syringe barrel and plunger. Moreover, syringes with low dead space have a particular risk of depositing SiO.4 8 The particular brand of syringe used in our clinic contained SiO, has low dead space, has been shown to release more silicone than other comparable syringes8 and has been the culprit of intravitreal SiO in previous case series.3 4 In January 2021, the manufacturer issued a security statement regarding SiO floaters, emphasising that their syringes were not validated for IVI. A change to a syringe without SiO eliminated the problem, even though the new 33 G injection needle (TSK) also was coated with SiO. This strongly points towards the insulin syringe as the source of intravitreal SiO. It is uncertain why the syringes suddenly started causing floaters after several years of use. Since no changes had been made to the compounding or injection procedure, minor alterations in the syringe production seem likely.
Some important limitations of the study should be noted. First, among the 19 physicians who evaluated the patients, 2 physicians (MCM and MSS) diagnosed 22 of 46 included cases. An increased awareness towards this problem may have contributed to this over-representation. Second, the study only addresses a cluster at a single centre. Still, our department is the largest provider of retinal care in Norway and performs nearly 30 000 IVIs annually.18 Accordingly, it is a suitable centre for addressing relatively uncommon complications of IVI, including deposition of intravitreal SiO.
Conclusion
We describe a large cluster of symptomatic intravitreal SiO following IVI with compounded syringes. A majority of symptomatic patients reported prolonged complaints, and non-symptomatic cases were also prevalent. Changing to SiO-free syringes eliminated the problem of intravitreal SiO.
Data availability statement
Data are available upon request.
Ethics statements
Ethics approval
This study was approved by the Oslo University Hospital data protection officer, approval number 2013/6682.
Acknowledgments
The authors would like to thank all the physicians and nurses who contributed to the data collection in this study. They would also like to thank their hospital pharmacy for excellent collaboration to develop and continuously improve the described compounding procedure.
References
Footnotes
ØKJ and MCM are joint senior authors.
HEL and TTG contributed equally.
Contributors MSS, MCM and ØKJ designed the study and analysed the data. MCM and MSS performed the data collection and prepared the figures. MSS, MCM, ØKJ, HEL, TTG, GP and JTA drafted, revised and edited the manuscript.
Funding HEL was supported by the South-Eastern Norway Regional Health Authority (grant no 40109), and in part by Dr Jon S Larsens Foundation and The Norwegian Association of Blind and Partially Sighted. TTG was supported by internal funding from Division of Head, Neck and Reconstructive Surgery, Oslo University Hospital.
Competing interests MSS, ØKJ, MCM and JTA have, through the hospital technology transfer office (Inven2), signed an industry development agreement with a company producing syringes for intravitreal injections. MSS has been an investigator in an Alcon sponsored clinical trial. ØKJ has received lecture fees from Allergan, Alcon, and Bayer, has been a member of a Bayer advisory board and an investigator in an Alcon sponsored clinical trial. MCM is member of Bayer and Novartis advisory boards and has been an investigator in an Alcon sponsored clinical trial
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.