Article Text

Abstract
Objective To explore living with heritable retinoblastoma, specifically survivors’ perceived role of regular follow-up at a retinoblastoma survivorship clinic.
Methods and analysis Adult survivors of heritable retinoblastoma were recruited from the Retinoblastoma Survivorship Clinic, Aarhus University Hospital. Ten survivors participated in individual explorative, semistructured interviews. Thematic data analysis was conducted.
Results Five key themes relating to vision, social life, family, second cancer risk and the healthcare system were identified. Subthemes relating to the Retinoblastoma Survivorship Clinic included the retinoblastoma coordinator, cancer risk, psychosocial support and genetic knowledge. The retinoblastoma-related physical and psychosocial issues influenced survivors’ everyday living; however, the opportunity to live a normal life varied considerably, with the majority experiencing no major limitations. The need for specialised management and a coordinator was emphasised to be the main value of the Retinoblastoma Survivorship Clinic.
Conclusion Despite reporting an overall normal life and no major limitations in daily living activities, our data confirm that heritable retinoblastoma impacts several aspects of daily living. Uniquely, this study demonstrates that the main value of the Retinoblastoma Survivorship Clinic was a specialised contact person and coordinator in the healthcare system, providing continuous and necessary management and guidance after retinoblastoma treatment, and for all aspects of health related to heritable retinoblastoma. The needs of heritable retinoblastoma survivors are complex and extensive, and the specific role of the healthcare system to support survivorship should be prioritised, specialised and multidisciplinary.
- genetics
- retina
Data availability statement
Data ara availble upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Retinoblastoma survivors generally report a good overall health-related quality of life, but there are several concerns.
What are the new findings?
In-depth insight describing that despite an overall normal life and no major limitations in daily living activities, heritable retinoblastoma impacts important and complex aspects of survivors’ life. The needs of survivors with heritable retinoblastoma may be more adequately met by a retinoblastoma survivorship clinic with a coordinating specialist.
How might these results change the focus of research or clinical practice?
Anticipation of retinoblastoma survivor requirements and the coordination of multidisciplinary input via a retinoblastoma survivorship clinic may better support the specific health needs of heritable retinoblastoma survivors with the potential for improved health outcomes. Centralised, longitudinal follow-up of retinoblastoma survivors may also facilitate research opportunities of the overall health outcomes of survivors.
Introduction
Retinoblastoma (RB) is a rare intraocular cancer most often occurring in children before the age of 5 years. The overall prognosis is good, with a survival rate above 95% in high-income countries.1 The type of vision loss in survivors of RB is variable and depends on laterality, stage and treatment of disease.1 Approximately 50% of affected children develop heritable RB due to a pathogenic RB1 germ-line variant.2 Patients with heritable RB have a 50% risk of passing on the RB1 variant to their child,3 and also have a significantly increased risk of second primary cancers later in life.4–7 Screening protocols for second primary cancers have been suggested, but currently, there are no international consensus guidelines1 8 9; whole-body MRI at regular intervals has limited sensitivity and specificity.10 11
The RB Survivorship Clinic at Aarhus University Hospital was established in 2016, and has since been iteratively developed and modified to better meet the needs of RB survivors and parents. The clinic was initially implemented due to the anecdotally reported clinical experience of unmet needs in survivors and families with heritable RB. The primary aims of the RB Survivorship Clinic are to: (1) aid the early diagnosis of second primary cancers by improving survivors’ knowledge and help-seeking intentions, and to institute relevant physical examinations (eg, regular dermatological examinations); (2) reduce mental health problems by identifying and addressing possible psychosocial issues related to their disease and its treatment; (3) facilitate optimal family planning.12 Improved health education and health awareness support survivors of RB to act and react appropriately to concerns and to be advocates for their own health.1
Previous studies have examined the multifaceted psychosocial effects and needs of RB survivors.13–19 Studies from Holland observed a relatively good overall health-related quality of life in children13 and adults,14 but highlighted concerns related to their mental health, such as anxiety, feelings of depression, as well as loss of control among adult survivors.14 Survivors of RB who were treated by enucleation of one or both eyes report specific psychosocial problems: struggling with self-consciousness due to treatment-related effects on their physical appearance and social and relationship issues (bullying and teasing).16 Bilaterally affected survivors identified greater fear of recurrence of primary disease, second cancer and passing on the condition to future children, all likely reflecting their understanding of the genetic nature underlying bilateral disease.17 Despite overall good psychosocial functioning in RB survivors, heritable RB has added complexity and likely greater overall associated burden, the elements of which could be anticipated and mitigated in a survivorship programme.17 The needs for improved psychosocial care and support have been highlighted in previous studies.18 19 However, there remains a lack of knowledge about heritable RB survivor’s overall and specific needs, the optimal setting for and the specific function(s) of an RB survivorship clinic. Heritable RB survivors represent the highest number of survivors with a cancer-predisposing germ-line variant in the USA,20 a statistic that would be echoed in other countries. Thus, exploring the experiences and needs of these survivors is relevant.
The aim of this study was to (1) explore the personal experience of life after surviving heritable RB and (2) the perceived role of regular clinical follow-up visits at a newly implemented RB survivorship clinic, and to explore living with heritable RB in the context of participating in an RB survivorship programme. The results of this study will be used to improve patient-centred care for RB survivors.
Materials and methods
Study design
An explorative, qualitative study design was undertaken to obtain in-depth insights into the lived experience of RB survivors and the perceived role of an RB survivorship clinic.
Study setting
All Danish citizens have free access to medical care, and RB management has been centralised in one national RB unit in Aarhus since 1963. In 2016, regular ophthalmological follow-up throughout childhood and for many into adulthood, was extended by establishing an RB Survivorship Clinic. All heritable RB survivors who have completed acute treatment of their primary disease are eligible to attend this service.
The RB Survivorship Clinic is a multidisciplinary clinic primarily comprising ophthalmologists, geneticists and oncologists and is conducted in a hospital setting. The primary coordinating clinician is a clinical geneticist with experience with rare genetic conditions and cancer predispositions syndromes in children and adults. For the majority of the RB survivors attending the RB Survivorship Clinic, a yearly outpatient consultation is planned with a focus on physical and psychological problems, continuous information/education on optimal health behaviour, as well as anticipatory genetic counselling as required. Yearly examinations by a dermatologist is instituted, and referral to additional specialists or imaging is initiated where indicated (eg, mammography). The survivors can access the clinic coordinator in between their regular visits as required via mail, telephone or an additional visit to the outpatient clinic.
Sampling and recruitment
Patients above the age of 18 years, diagnosed with heritable RB who attended the RB Survivorship Clinic, Aarhus University Hospital between 1 June 2019 and 1 June 2020, were consecutively invited to participate in the study. Written and verbal information about the study was provided by the first author (PAG), a senior consultant clinical geneticist at the RB Survivorship Clinic. Of the 11 patients approached, 10 provided consent to participate and a time and date for the interview was arranged.
Data collection
The interviews were based on a semistructured interview guide that was informed by scientific literature and by the interdisciplinary expert knowledge of the authors (from fields of genetics, ophthalmology, anthropology). An RB survivor provided feedback on the draft interview guide and volunteered to participate in a pilot interview. Interview questions were revised for clarity and meaning (table 1). Relevant demographic questions were added to the guide (table 2). All individual interviews were conducted by the last author, SL (senior anthropologist, PhD) who has extensive experience in conducting patient perspective interviews. SL is not associated with the RB Survivorship Clinic, allowing participants the opportunity to express potentially negative issues relating to their experience with the clinic.
Interview guide
Demographics, self-reported
By participant choice, the interviews were conducted by telephone (n=6), videoconference (n=3) or face to face (n=1). On average, the interviews lasted 53 min (range 38–75 min). During the interviews, participants were encouraged to speak freely about their experiences and to include any topic they found relevant to the issue. All interviews were audiorecorded, transcribed verbatim and deidentified prior to analysis. Transcripts were not returned to participants for comments/correction. During data collection, the preliminary findings and potential interpretations were continuously discussed among the authors. Data collection ceased when the first and last author assessed that the data were rich and adequate, and thus, had sufficient 'information power'21 to provide for an analysis.
Demographic information was collected by a combination of self-report (completing demographic questions in interview) and collection from the participant’s medical records.
Data analysis
The data were thematically analysed.22 Following initial data familiarisation, a coding framework was developed using a combination of deductive and inductive codes. To illustrate, the deductive codes were drawn from topics in the interview guide and included codes such as ‘patient support groups’ or ‘level of visual impairment’. Inductive codes were issues that emerged from the data and included codes such as ‘I’m normal’ or ‘fear of death’. A test coding of two selected interviews by two researchers (PAG and SL) was independently undertaken to ensure consistent coding, and the material was then coded by PAG using NVivo V.12 qualitative data analysis software (QSR International, V.12, 2020). The coded material was read and compared and codes were collated into preliminary clusters of meaning (themes and subthemes) in Danish, which were then discussed by the broader research team. No significant changes to the analysis were necessary.
The quotes as reported here have been translated from Danish to English, reviewed by both native Danish and English-speaking research team members to ensure the meaning was not lost in translation. Additional information about the translation process is available in online supplemental material. To support participants’ anonymity, no additional personal, medical or demographic information is provided for each quote.
Supplemental material
Reflexivity
Throughout the research process, the authors were reflexive about how their positions and preconceptions could influence the research. With the exception of SL and MHO, all authors see patients with RB and survivors, or are involved in RB management in their respective clinical specialties, and we acknowledge that they all share a strong motivation to improve services to RB survivors. However, the interdisciplinary discussions in the research team (consisting of professionals from genetics, ophthalmology, anthropology, oncology and public health) served to challenge and make visible potential biases in the study, for example, preconceptions about RB survivors needs and concerns.
Patient involvement
This study was led by a cross-disciplinary and international research group with substantial knowledge about RB survivors. An adult RB survivor was engaged in developing the patient information sheet and the interview guide. During the research process, SL encouraged the participants to provide feedback on the interviews and the researchers’ preliminary interpretations. All interested participants will be provided with the overall study results and an opportunity to discuss them with the research team.
Results
A total of 11 patients met the inclusion criteria and were invited to participate in the study. Of these, 10 agreed to be interviewed: 6 by phone, 3 by videoconference and 1 face to face. Specific demographic characteristics of the participants are outlined in tables 2–4.
Demographics, medical reports (treatment)
Demographics, medical reports (visual acuity)
The majority of the participants did not recall their initial course of disease, but all remembered repeated ophthalmic examinations and follow-up treatments. Variable degree of discomfort was related to these memories (eye-drops, general anaesthesia, etc). All participants lived with a variable degree of reduced vision, but repeatedly emphasised that they led normal lives and were able to participate in daily living activities.
Figure 1 outlines the five major themes identified following data analysis and are described in detail below.
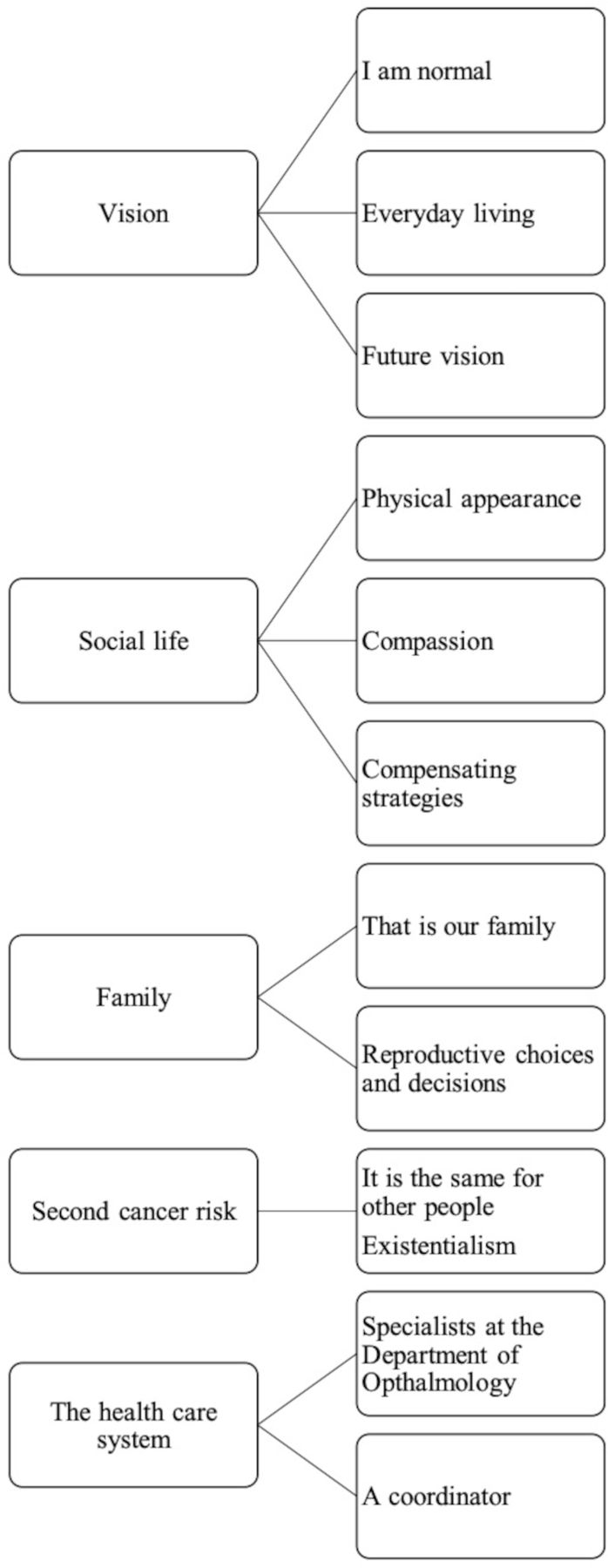
{kind=link}
Five major themes and subthemes following thematic analysis.
A life with vision impairment
Vision impairment was the major concern following RB as emphasised by all participants, although their degree of reduced vision varied by severity as well as type of impairment (table 2). Several participants experienced deterioration of vision over time, due to treatment-related complications (ocular surface problems, cataract, etc) or age-related effects on vision (presbyopia):
I always have it in the back of my mind, when will it decline? I didn't worry earlier in my life, because my vision was relatively stable. But I fear that this is the first step downhill. I am only in my 30s, and hopefully I will have a long life, so I hope my vision is not absolutely miserable in my 40s. (P08)
Vision impairment affected daily activities. The participants did not describe practical chores such as maintaining their ocular prothesis, the daily use of eye-drops and the use of glasses and contact lenses as a significant problem, but still a time-consuming, laborious task influencing everyday life. In addition to these practicalities, vision impairment sometimes meant that everyday activities such as pouring water or lighting a candle could be challenging. Participants with no vision in one eye described how the decreased field of vision could lead to reduced awareness of their surroundings, and at times led to collisions with objects or people:
I accept that my field of vision is reduced compared to others, and that just means that I still walk into the door frame sometimes, or into people standing on my wrong side. (P04)
However, despite vision impairment and related practical challenges, all participants reported an overall normal life:
We can still do most of the things we want in everyday life with the exception of watching 3D movies and stuff like that (laughing). (P03)
Regarding education and work life, only one person reported that the reduced vision directly influenced her choice of vocation. Several did mention, on a more hypothetical level, that some professions where unattainable due to their vision impairment:
A part of me would like to be part of the helicopter team, evacuating patients; but from what I have read, it’s not super smart to be partly blind in one eye. (P05)
Even among participants who seemed very successful and fulfilled in their everyday lives, (two were elite-level athletes), regret was expressed related to not being able to exploit their full potential:
Imagine, if I could see with both my eyes. I mean, I think I am pretty good at many things, and I thought: imagine, if I was not hindered by this? (P01)
Navigating social life
The majority of the participants described how RB indirectly impacted their social life. Some participants’ prosthetic eye was the only ‘clue’ to their visual impairment while others described how the RB treatment (eg, radiation) had significantly impacted their physical appearance. The majority of participants reported none or only ‘normal’ bullying during childhood, but two participants experienced massive bullying, with social and emotional consequences following them into adulthood:
Today, I guess I am what you would call socially handicapped. I do not trust people because I have experienced that people attack me, degrade me and become personal. (P05)
As adults, some participants were very conscious of how strangers might respond to their physical appearance. They described how children and adults would stare at them or whisper behind their back in public places, and how they sometimes felt the need to confront this behaviour or wished that people would just ask about it. Some expressed concern with being judged by their physical appearance instead of their personality (eg, when going on dates or for job interviews), and a few described trying to hide their prosthetic eye with their hairstyle or by only photographing from certain angles:
When I was younger, I tried to cover half of my face with my hair. I still have that habit if I am among many people. (P02)
In addition to the social impact of their physical facial features, many participants reported how they also tried to hide, or compensate for, their reduced vision when participating in social engagements:
When I am invited to dinner, I quickly find the corner of the table that is best for me in terms of my vision. I prefer not to have an unknown person on my right side because it reduces my social interaction because I miss a lot on that side. The person might pass me the dish, and I do not see it. (P04)
However, the participants also frequently expressed that they did not want ‘special treatment’ or to take up unnecessary social attention, or to draw any additional attention, compassion or special considerations. For all participants, it was important that their RB-related challenges did not overshadow social relationships and situations.
Being an RB survivor could sometimes impact social relations, as many people respond emotionally when being confronted with childhood cancer:
One thing I have become better at is telling others about ‘the cancer story’. It is like an art, because if you just say: ‘I had cancer,’ people are ‘Oh no, are you dying… ‘So, it is a balancing act. (P01)
By constructing a ‘cancer story’ and being careful how, when, and to whom they revealed the vision impairment and/or the cause of it, the participants kept the RB diagnosis from taking centre stage in their lives:
It is part of who I am, but it is not my personality. (P01)
Interestingly, the participants did not interact with other RB survivors (beyond their family). Patient support groups were not in high demand and while several commented on the benefits of such support for parents of children with RB, the majority argued that they did not identify with the condition and did not want it to be an issue in their lives:
I have tried to hide it. I will not call it a trauma, but it is after all a burden from my childhood, I do not wish to relate to, if I do not have to. (P04)
It runs in the family
The genetic nature of the condition was reported as playing a very important role for the majority of the participants: often many family members were affected, some had affected children and/or concerns about the risk for future children. As such, the possibility, responsibility or burden to make active decisions regarding a heritable family condition was a central concern in their lives:
Since my childhood, it was always stressed, how I could stop this condition in my family. (P10)
All participants reported that they did not wish for their children to inherit RB:
I have always known for sure that I would not pass this on, no matter what. I would almost rather avoid having children than risk having a child with this disease. (P08)
As many of the participants reported living fulfilling lives, we enquired further about this wish to avoid RB in future children:
With this, I can do something. I might not be able to prevent that my kids are bullied, get sick, need treatment. They can get all sorts of other things, that I can’t do anything about. However, I can do something about this. (P05)
Reflections on the lifelong consequences of RB despite a normal life was expressed:
Specifically this higher risk of becoming sick again, that this is not just an eye disease. It is not just treatment for that disease. The fact that this follows you for the rest of your life. (P07)
Of the seven participants who had children, three had not had the opportunity for prenatal testing and of these, two now had children with RB:
I would give my right hand for this not to have been the case… but my reasonable thought is after all, that I can’t help it. (P04)
Four had had preimplantation genetic testing or prenatal diagnostic testing in order to avoid passing on the condition. However, this decision was not easy as undergoing fertility treatment or waiting for a prenatal diagnosis caused considerable stress and some participants expressed feeling guilty for putting their partner though this process, because of their own genetic ‘flaws’.
Managing the second cancer risk
All participants were aware of the increased risk of developing second primary cancers; half had known about it since childhood or adolescence, and the rest were informed as adults. Hence, for some participants, this had always been a circumstance in their life:
I recall it, as I have almost always known it. My parents have always been very up front about telling me these things, and so have the doctors. (P01)
Despite generally not being worried about this increased risk, several stated that they paid extra attention to sun protection, had their skin checked regularly, and in general aimed for a balanced, healthy lifestyle:
We are told, you have to avoid sun burn because it increases your risk for skin cancer etc., but for me that’s not so special—it belongs to the general mantra: live healthy. (P08)
Talking about the potential psychological impact of knowing about the risk, the vast majority said that they preferred knowing about it, in order to be able to be proactive and prepared:
I’d rather look at the monster up front instead of being beaten by it. (P04)
However, they also recognised how this knowledge could cause worry and anxiety:
My wife is extremely worried on my behalf, and of course that reminds me about it. But it does not ‘ride me like a mare’, not at all. It is not something I walk around and worry about. (P10)
While the majority was not particularly worried, for some families, the risk of second cancer was more present:
Looking back, my mother had retinoblastoma, skin cancer, malignant melanoma and breast cancer, i.e., she was hit four times. That is not a nice knowledge to have. (P05)
This knowledge, however, had not caused the participant to live differently. Many participants emphasised how the precautionary measures they took were not different from what other people should do:
We all have to die at some point, and I do have—no matter I had cancer or not—a healthy lifestyle. I like to do exercise and do not live on McDonald’s. To me, that’s not because I had cancer, I live healthy. It’s just because I have to. (P08)
Being an RB survivor in the healthcare system
Many participants described a lifelong connection with the specialist-RB ophthalmologist at the hospital. With only one specialist unit in Denmark, most participants had made annual visits to the RB eye clinic throughout their childhood. As adults, the participants described a high level of satisfaction with the RB eye team, and specifically described how they appreciated and valued the continuous, direct access to this specialised care.
What I particularly appreciate is going directly through the eye department for further treatment, instead of having to go through some random, generic eye doctor first. (P08)
This underlined the struggles and frustrations that participants had experienced when seen by an eye doctor who lacked specific knowledge about RB and the long term or late effects of treatment:
The non-specialized eye doctors take one look at me and find all kinds of deathly conditions, because there is nothing [in my eye] that looks the way it should. (P05)
The need for better psychosocial support as part of the follow-up RB treatment at the eye department was mentioned:
They are eye specialists. There is very little focus on the psychological consequences following treatment or living with this condition. (P10)
As described above, none of the participants were engaged in patient networks or online RB support groups. Thus, many had felt alone with the questions and concerns related to being an RB survivor.
The value of the RB Survivorship Clinic
RB coordinator
The need for an RB coordinator was emphasised: the majority of participants reported that the main value of the newly initiated RB Survivorship Clinic was to have a coordinator in the healthcare system, who remained abreast of the latest RB knowledge and evidence and could provide access to the diverse medical specialties as required:
It’s nice to talk to a specialist that can tell me things, I did not know, and that I might need to pay attention to. (P02)
Several participants had experienced complications related to RB and RB treatment, were not always recognised or effectively managed in the general healthcare system. Specifically, two participants described how the treatment of dental complications related to RB treatment was unnecessarily complicated, and for the majority of the participants, dermatological examinations had not been initiated before attending the RB Survivorship Clinic.
The participants valued the continuous relationship with their RB coordinator who were knowledgeable about both the medical and family history of the participant
It’s nice to meet a familiar face, and someone who knows your history. (P08)
The experience of living with a rare and complex condition caused frustration and a sense of being invisible in the healthcare system, who is not optimally equipped or sufficiently knowledgeable to care for patients with conditions that stretch across multiple medical specialties. When asked about what the healthcare system could do for making life easier, one participant responded:
Take me seriously. Listen to me and take me seriously.[…] If I did not have [name redacted], I would not be heard. (P05)
The more holistic approach was also acknowledged:
[Name redacted] is more in attentive to me as a human being, in contrary to the eye department, where I am more of a ‘patient’. (P01)
Thus, the value of the RB Survivorship Clinic was viewed as a medical assessment beyond the ophthalmological examination, and the increased attention to managing heritable RB in the healthcare system in general seemed to be a so far unmet need:
I just clap my hands when there is more focus on, and knowledge about, RB. That is exactly what I have been missing, and I can’t imagine that I am the only one missing that. (P05)
Overall, the participants conveyed that the visits led to a feeling of security, and some valued how the visits had a more universal and comprehensive approach to their condition:
[Name redacted] has emphasized that there might be things I can do to be proactive … to lower the risk for cancer later in life. And one reason why I will continue to go to the RB clinic is that they have knowledge about your life after the treatment. (P08)
Second cancer risk
The need for better knowledge on second cancer risk was emphasised, and specifically valued as a direct result from participating in the RB Survivorship Clinic:
If it was not for [name redacted], we would not have known about the skin cancer and malignant melanoma risk. (P05)
That the evidence of higher risk of cancers was acknowledged and supported by the RB Survivorship Clinic gave the participants a sense of certainty and legitimacy in their interactions with the general healthcare system. Also, participants appreciated that they could refer to the Clinic if their requests were not met (eg, for dermatological examination) or if they needed a coordinator facilitating necessary actions:
If the doctors don’t take me seriously, then I am deeply dependent on [name redacted]. That someone says, that due to this genetic mutation and the family history, what needs to be done, must be done. (P05)
The participants valued having an opportunity to evaluate their current situation in general, however the psychological impact of the enhanced cancer-risk knowledge was also reflected on:
It is nice to know if there is anything new, and we get to talk about how we are doing, and [name redacted] can check if there is anything that needs to be checked up on… But at the same time, it is a reminder that there is something [increased risk]. (P07)
Psychosocial support
None of the participants reported feeling anxious or nervous prior to a consultation at the RB Survivorship Clinic and only a few prepared for the consultations, for example, preparing questions or topics they would like to discuss. The expected (and experienced) benefit of the consultations for some participants was an update on the latest research and a plan of action regarding future physical and psychosocial health issues.
The need for increased psychosocial focus and support was emphasised by some participants, as well as the beneficial role of RB patient organisations. The existing patient organisations primarily meeting parents’ needs and hence the present lack of an organisation for adult RB survivors was mentioned. The specific needs to be covered by patient organisations was reflected on:
I would still be interested in meeting others… I think it could be interesting and giving… It could give another perspective of how they have been doing. I always find it inspiring to hear what others have done with their life, and what has affected them. (P02)
Currently, the RB Survivorship Clinic does not facilitate contact between patients, but some participants expressed an interest in participating in patient seminars and/or meetings.
The need for better social support in terms of understanding and navigating the public social and healthcare systems was underscored by the perceived difficulties with understanding the legislation and what social/health benefits the survivors were entitled to:
I am very grateful for the system we have, but some time, I get really frustrated over things and think: Bloody h…, you really need to have many resources. (P02)
Genetic knowledge
Repetitive genetic counselling as part of the RB survivor care was valued:
One of the reasons for attending [name redacted] was related to the genetics…I was at that time a place in life, where having children, and because it is heritable, I wanted to know the possibilities for avoiding passing on the genetics [RB1 variant]. (P08)
Some of the survivors’ expressed regrets over not having known about the various reproductive options for avoiding RB in children.
It’s easy to second-guess—but then I might have… known more about how big the risk for RB actually is. And what other options there are, or are there other options? (P09)
Discussion
The purpose of this study was to explore the impact of living with heritable RB, and more specifically, the perceived role of regular follow-up visits at an RB survivorship clinic. Particularly, we wanted to explore the specific needs of survivors of heritable RB, physical and psychosocial, and how an RB survivorship clinic may support RB survivors.
The results show that survivors with heritable RB in general lead normal lives and participate in daily living activities despite some restrictions: variable degrees of vision impairment, cosmetic concerns and the genetic nature of their condition leading to increased risk for second cancers and RB in children. These findings confirm previous studies.15 16 19 Uniquely, the study results demonstrate that the main value of the RB Survivorship Clinic is the comprehensive approach and a familiar contact person and coordinator in the healthcare system. Providing continuous and necessary management and guidance after RB treatment, and for all different and often age specific aspects related to heritable RB, the survivors’ needs appear to be met. The significant need for coordination and specialised management of the complex late effects of treatment, long-term complications, genetic issues and future problems is known from other rare genetic conditions with possible involvement of various organ systems.23 The study specifically explored the perspectives of adult survivors of heritable RB, to both avoid parent’s and non-heritable survivors’ differing perspective, though acknowledging their shared perspective.
The first listed RB Survivorship Clinic goal is to aid the early diagnosis of second primary cancers by improving survivors’ knowledge and actions, and instituting relevant physical examinations. The participants confirmed the importance of specialised knowledge and management in the healthcare system, and the need for a coordinating contact person.
The anticipation that balancing knowledge of second cancer risk and the psychosocial effect of knowing was confirmed by several participants explaining the ambivalence of knowledge. The risk for second primary cancer was acknowledged as a potential concern, but for the majority of the participants, it did not seem to be an overwhelmingly heavy burden. The participants seemed to cope well holding the knowledge, and the majority preferred being able to be proactive. Survivors emphasised that everyone has a risk of cancer, and in this way, they tried to normalise their increased risk. Overall, they seemed to appreciate knowing, a finding that resonates with previous research showing that, despite the serious nature of the information, the majority of RB survivors want this information.24 Our results suggest that the impact of living with an increased cancer risk due to heritable RB might be lighter than anticipated. However, an interpersonal dichotomy in the RB population towards RB knowledge in general is reported previously19; as suggested by authors, individual approaches are necessary to provide only as much information as desired by the survivor,19 and the RB Survivorship Clinic could be optimised by even more individual approach to RB survivors. Refined methods for this still need to be developed and validated.
The results suggest that the RB Survivorship Clinic’s comprehensive and more holistic approach to heritable RB, anticipates the survivors’ needs. Specialised and dedicated knowledge and experience with all aspects of RB and living with RB, was important for the participants. Vision impairment, the related limitations and compensatory strategies related to the social and variable psychological consequences of their condition/disability, were a daily living issue for several of the participants, although the majority strongly emphasised that it did not prevent them from living a normal life. The desire to live a normal life was a consistent sentiment of the interviews. This is in accordance with other studies reporting difficulties related to physical appearance and social life, but no overall major impact on psychosocial functioning and quality of life.14–19
The second RB Survivorship Clinic goal is to reduce mental health problems by identifying and addressing possible psychosocial issues related to RB and above-mentioned issues. Participants did emphasise the need for psychosocial support; this finding was previously reported.18 In the RB Survivorship Clinic, psychosocial issues are addressed by the primary consultant, and referral for further evaluation is initiated if needed, but the study highlights the need for specialised psychosocial support by professionals (psychologists) with specific RB knowledge. Furthermore, the study team recognise the participants recurring issues, and even though patient organisations were not in high demand, we anticipate that sharing of peer-to-peer experiences facilitated in the setting of the RB Survivorship Clinic, could be beneficial.
Concerning heritability, all participants had a clear wish to avoid passing on RB to their children. Genetic counselling including information about reproductive options was a need identified by all participants. Some of the survivors’ expressed regrets over not having known about the various reproductive options for avoiding RB in children. The appreciation of presenting new knowledge/research about RB was also mentioned by the participants, a finding that confirms previous reports.19
As the third RB Survivorship Clinic goal is to facilitate optimal family planning, knowledge about heredity and various reproductive possibilities should be conveyed repetitively to ensure correct interpretation and informed choices in RB survivors. Survivors’ knowledge about genetics in RB can be variable and often limited,18 and the perception of risk is important for reproductive behaviour.12 Visits to the RB Survivorship Clinic include regular comprehensive genetic counselling, though adapted to survivors’ individual age and needs.
In order to ensure sufficient survivor information and to anticipate the impact of heritable RB, the RB survivorship Clinic have recently performed genetic follow-up: all Danish RB survivors without prior affiliation to the RB Survivorship Clinic and no known previous genetic testing have been invited to undergo genetic counselling and testing for heritable RB. Our study confirms the need for comprehensive genetic information and knowledge, especially keeping in mind that all participants expressed a clear wish to avoid passing on RB to their children.
This study confirms the concerns and burdens of living with heritable RB,15 16 19 but more importantly, how an RB survivorship clinic may support RB survivors. The study emphasises the survivors’ need for a voice in the healthcare systems, and a coordinator bringing relevant healthcare resources in play, when needed.
The major limitation of our study is the small number of RB survivors and possible selection bias. As the participants were all recruited survivors attending the RB Survivorship Clinic, they might cope better than the general population of RB survivors, thus underestimating the negative psychosocial consequences. Accordingly, the needs of the survivors as expressed by the participants might deviate from the general population of RB survivors’ needs. Furthermore, the demographics of our study was narrow as the majority of the participants were below the age of 40 years: the oldest participant, one of two participants above the age of 40 years, was only 64 years old. Hence, the study group was skewed towards a younger demographic. This may have affected the interpretation of results towards underestimation of, for example, the impact of having a high risk for second primary cancer.
Notably, our study is narrowed to adult survivors with heritable RB, acknowledging that survivors of non-heritable RB may share several of the RB-related complications and hence presumably share many of the needs revealed by this study.
Future studies and implications
Future studies
More studies including a greater number of RB survivors are needed to further elucidate the multifaceted and lifelong changing impact of heritable RB, the needs of RB survivors, and more importantly: how to optimise lifelong healthcare for RB survivors. Specifically, a wider demographic group of participants with a broader age span of participants is preferable. Quality improvements studies in RB survivorship clinics, comparing data from different but comparable clinics would be valuable, and could preferably focus on both medical and psychosocial needs and interventions. Furthermore, strategies to ensure an individualised approach to delivering relevant information and knowledge to RB survivors, need to be developed and validated.
Implications
The task of managing and coordinating the complex, diverse and age-specific challenges in heritable RB should be assigned to a specialist with experience in RB, and a multidisciplinary approach should be encouraged. The latter primarily involving ophthalmology, genetics and oncology is of utmost importance, since the lifelong implications of RB do not naturally fit into one specific medical field; the ophthalmologist plays a key role in ensuring non-ophthalmic follow-up in heritable RB survivors. Furthermore, the multidisciplinary approach must include psychologists and social workers: The need for a psychosocial focus and appropriate intervention when required must be stressed in order to support RB survivors to develop optimal coping skills including compensatory skills and, ultimately, to build resilience.
Given the multiple, different and at the same time deeply inter-related aspects of the disease, heritable RB should be managed as a lifelong and complex condition. However, despite many shared RB-related matters, variability among RB survivors is evident, and since survivors in general live a normal life, the RB survivorship clinic services should be adapted to the survivors’ individual needs.
Data availability statement
Data ara availble upon request.
Ethics statements
Patient consent for publication
Ethics approval
According to Danish legislation, interview studies do not require approval from the National Committee on Health Research Ethics; although, the study was approved by the Danish Data Protection Agency (J. No. 1-16-02-104-20).
Acknowledgments
We are very grateful to the RB survivors for their participation in this study.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors The idea of the study was formed by the first and last author. The first author recruited the participants, the last author interviewed the participants. Both analysed the data; both the first, last and third last author managed and interpretated the results. All authors contributed with writing of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.