Article Text

Abstract
Objective To evaluate the effect of weightlifting (leg press) on intraocular pressure (IOP).
Design Prospective cohort study.
Subjects A total of 24 participants met the inclusion criteria and completed the study procedures. Participants had an average age of 22.7±2.7 years and included nine women. The mean baseline IOP was 13.9 mm Hg (SD=2.4) with an average body mass index of 24.5 (SD= 3.1).
Methods The maximum load for a single lift was found for each participant. Participants then performed three leg press regimens: one repetition using 95% of maximal load (1RM), six repetitions using 75% of maximal load (6RM) and isometric push against a weight much heavier than maximal load (ISO).
Main outcome measure IOP was measured pre-exercise, during and immediately following the exercise using an iCare TA01i rebound tonometer. Blood pressure and HR were being monitored continuously during the lift. Optical coherence tomography images were obtained pre and postexercise session.
Results The average maximum weight lifted by our participants was 331.9 Kg (SD=97.3). Transient increased IOP was observed across the 1RM, 6RM and ISO exercises with an average increase in 26.4 mm Hg (23.7 mm Hg to 28.7 mm Hg) to reach an average max IOP of 40.7 mm Hg (27.8 mm Hg to 54.2 mm Hg), with an absolute maximum of 70 mm Hg in one participant.
Conclusions There is a transient and dramatic fluctuation in IOP with resistance training. This coupled with regular exposure to resistance training is potentially a significant risk factor for glaucoma. It should be noted that this study has been carried out in a healthy young population, and, thus, the external validity of these results in glaucoma participants requires further investigation.
- intraocular pressure
- glaucoma
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Resistance exercise that requires with Valsalva Manoeuvre can significantly affect intraocular pressure.
What are the new findings?
When pushed to their maximal muscular engagement during resistance exercise, the participants mean intraocular pressure (IOP) was increased by average 26.4 mm Hg.
How might these results change the focus of research or clinical practice?
While this study was performed on healthy subjects with no history of glaucoma or IOP fluctuations, strenuous resistance exercise could be considered hazardous for individuals who are more susceptible to IOP changes
Introduction
The impact of exercise on intraocular pressure (IOP) and health is an area of increased interest as the importance of physical activity for maintenance of overall health is widely promoted.1 IOP results from the net balance between the production and drainage of aqueous humour. Elevated IOP is a significant risk factor for the development of glaucomatous optic nerve damage.2 However, different types of exercise are recognised to impact IOP differently. Acute changes in IOP have been noted during and immediately after different forms of exercise.3 Aerobic exercise such as running and jogging are associated with transient lowering of IOP postexercise compared with baseline values.3–8 The mechanism is presumed to be stimulation of the sympathetic pathway, resulting in increased aqueous outflow via the trabecular meshwork.9–12 In contrast, studies focused on muscle strengthening resistance exercise have produced mixed findings with both acute increases and decreases in IOP being reported.13–19
A fundamental principle in muscle-strengthening exercise is that strength is developed when a muscle or muscle group works against increasing amounts of resistance or weight over a period of weeks and months.20 Although muscle strength can be gained by lifting relatively light loads, maximal strength gains are made when muscles lift heavy, near-maximal loads.21 22 Lifting heavy loads requires core stability or bracing that is achieved by trunk muscle contraction and, although discouraged, the initial effort phase of lifting a heavy load often results in a Valsalva manoeuvre. Core bracing and Valsalva-induced increases in intra-abdominal and intrathoracic pressures are transmitted to systemic vascular and intracranial transmural pressures.23 IOP is known to be affected by changes in systemic and intracranial blood pressure and, thus, could be impacted by fluctuations in these pressures during weightlifting exercise.24 A current gap in the literature is a detailed understanding of the magnitude and time course of effect acute strength training exercise with near-maximal training loads has on systemic blood pressure and IOP.
The aim of the current study is to measure IOP and systemic blood pressure responses during high intensity weight-lifting exercise. We hypothesise that IOP and blood pressure will be dramatically affected by near-maximum effort weightlifting (leg press),24 and the effect will be much more significant compared with what is measured previously.25 26 We also hypothesise that such sharp change of IOP could be affecting the retina and choroid thicknesses.27 The focus of this study is to characterise the time course of change measured before, during and after the leg press exercise. The novelty of our study is that the IOP is measured truly ‘during the rep’ while the participant is still bearing the weight. This is unlike other studies where the IOP is measured ‘during the set’ when the weight is racked and muscular pressure is released. Furthermore, we performed optical coherence tomography (OCT) to investigate the effect of leg press-induced changes to IOP and systemic blood pressure on retinal and choroidal thickness.
Methods
This prospective study was approved by the University of Auckland Human Participants Ethics Committee (UAHPEC reference number 022578) and participants provided written informed consent. All research adhered to the tenets of the Declaration of Helsinki.
Study participants
Healthy volunteers between the ages of 21 years and 30 years of age were recruited through social media from local powerlifting clubs. Participants included1: individuals with at least 2 years of experience in resistance exercises training,2 a training history that included at least two sessions per week,3 free of any musculoskeletal or cardiovascular limitations4 familiarity with a leg press machine, with this exercise routinely performed during training. Participants underwent a comprehensive ophthalmological assessment including detailed general, family and ocular history, visual acuity (Snellen visual acuity), refraction arc perimetry (using confrontation fields by Bott wand), contact tonometry (Goldmann applanation tonometry), slit lamp examination and a fundus examination. Retinal photographs and fundus autofluorescence were taken using the Eidon Centervue SLO or Optos (Optos plc) camera. Participants were excluded if they had any systemic health conditions such as hypertension or previous physical injuries that could impact their safe participation. Participants were excluded if they had a diagnosed chronic health condition such as cardiovascular disease including hypertension and or previous physical injuries that could impact their safe participation as well as evidence of ocular pathology due to narrow anterior chamber angles, elevated IOP greater than or equal to 21 mm Hg, optic nerve or retinal pathology, cup:disc ratio of greater than 0.7 or asymmetry of cup:disc ratio of greater than 0. 2. Participants were also excluded if they were not able to complete the study protocol.
Experimental procedure
The full study protocol is explained in the supplementary material (see text, Supplemental Digital Content 1, which details the exercise protocol used in this project). Briefly, the experiments included baseline measurement of participants’ IOP, height and weight. This is then followed by finding the measurements of ‘maximum weight to be lifted’ by each participant, while performing a set of leg press exercises (figure 1). The participants are then asked to perform three types of lifts of (a) one repetition at 95% of maximum weight (1RM), (b) six repetitions at 75% of maximum weight (6RM) and (c) isometric hold of 10 s against weight that is much heavier than maximum weight that could be lifted by the participant (ie, immovable) (ISO) (Supplementary Figure 1)).
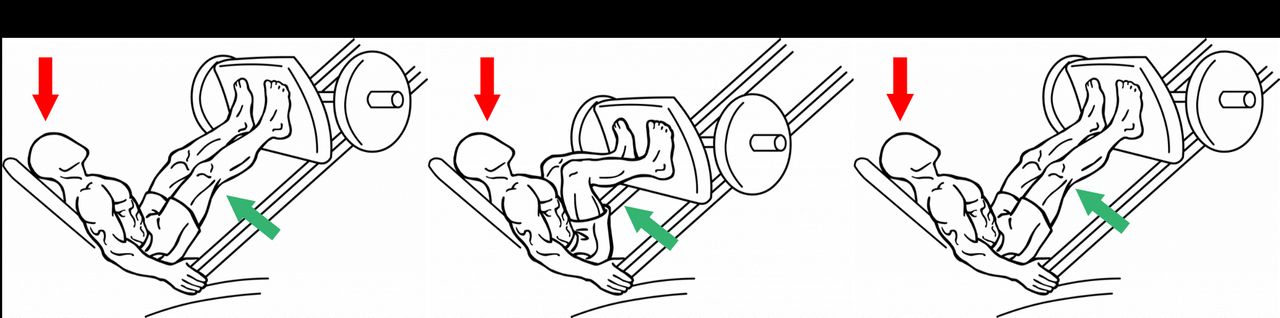
The steps of performing the leg press exercise, while measurements are taken. Initially, the participants are seated in the inclined position, while the weights are racked (ie, no muscular tension) when the ‘baseline’ IOP is measured (A). Next, the participant unracks the weight and bring them down until the knee joint angle reaches 90°. The weight is held there by the participant (ie, maximum muscular tension), while the IOP is read ‘during’ the exercise (B). Finally, the weights are pushed up and racked by the participant (ie, muscular tension released), and the last IOP is measured almost immediately (C). IOP, intraocular pressure.
Data analysis
All data were entered into an Excel spreadsheet and analysed in STATA V.15 (StataCorp 2017, College Station, Texas, USA). Change in IOP, mean systolic blood pressure (SYS), mean diastolic blood pressure (DIA), mean arterial blood pressure (MAP) and mean heart rate (HR) were calculated as the difference between the measurement during the exercise and the baseline measurement and expressed as ΔIOP, ΔSYS, ΔDIA, ΔMAP and ΔHR, respectively. Parameters for male and female subjects were compared with t-test; and paired t-tests were used to compare ocular and systemic variables pre and during exercise. Repeated measures multiple analysis of variance was used to see whether the physiological changes differed between the three exercises. Regression analysis was undertaken for 1RM, 6RM, isometric hold, maximum IOP out of the three exercises, retinal thickness change, retinal nerve fiber layer (RNFL), ganglian cell layer (GCL+), choroidal scleral interface (CSI) and choroidal thickness change. These data sets were analysed and compared with patient demographics, maximum IOP change, weights lifted and/or retinal and choroidal thickness changes. All tests were two-tailed, and results were considered statistically significant if the p value was <0.05.
Results
A total of 24 participants met the inclusion criteria and completed the study procedures. Participants had an average age of 22.7 years (SD=2.7), 9 women. The mean IOP was 13.9 mm Hg (SD=2.4) with an average body mass index (BMI) of 24.5 (SD=3.1). There was no statistical difference between male and female participants in regards to age (p=1.000) and BMI (0.574). The maximum weight lifted per BMI was lower in women compared with men (11.1 vs 14.8 p=0.0013) (Suplementary). The average maximum weight lifted by our participants was 331.9 Kg (SD=97.3).
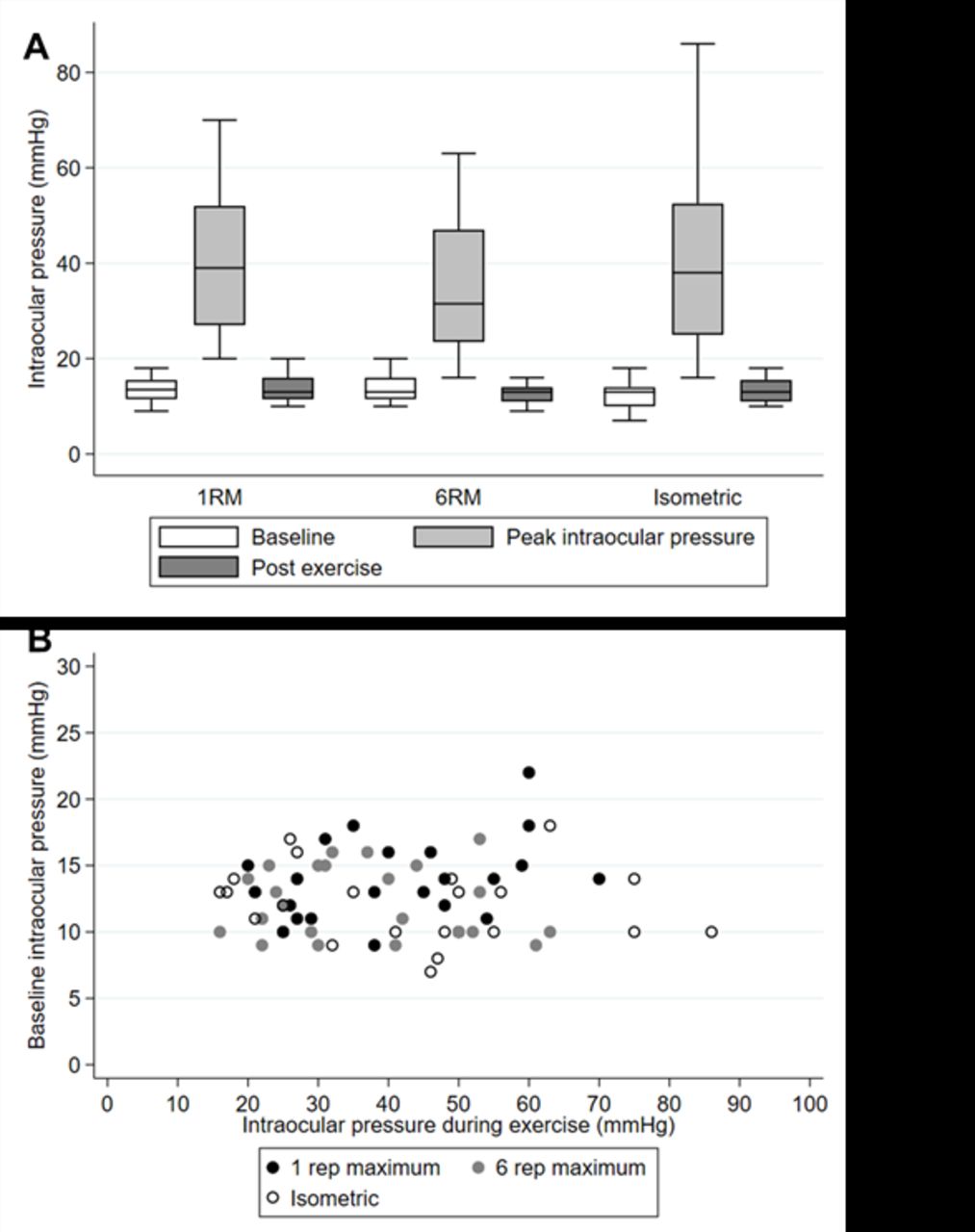
There was a significant increase in the IOP during weight-lifting exercises with the mean increase being 26.5 mm Hg (p<0.001) and a mean IOP across the group of 39.2 mm Hg. The greatest increase was during isometric resistance (28.7 mm Hg ± 20.7 mm Hg) and the least during the 6RM (23.7 mm Hg ±13.9 mm Hg), although there was no statistical difference (p=0.125 between the different type of resistance exercise as calculated by repeated measures MANOVA test (figure 2). The postexercise IOP was measured when MAP returned to baseline. In all participants, this occurred less than 1 min from release of the weight (figure 3).
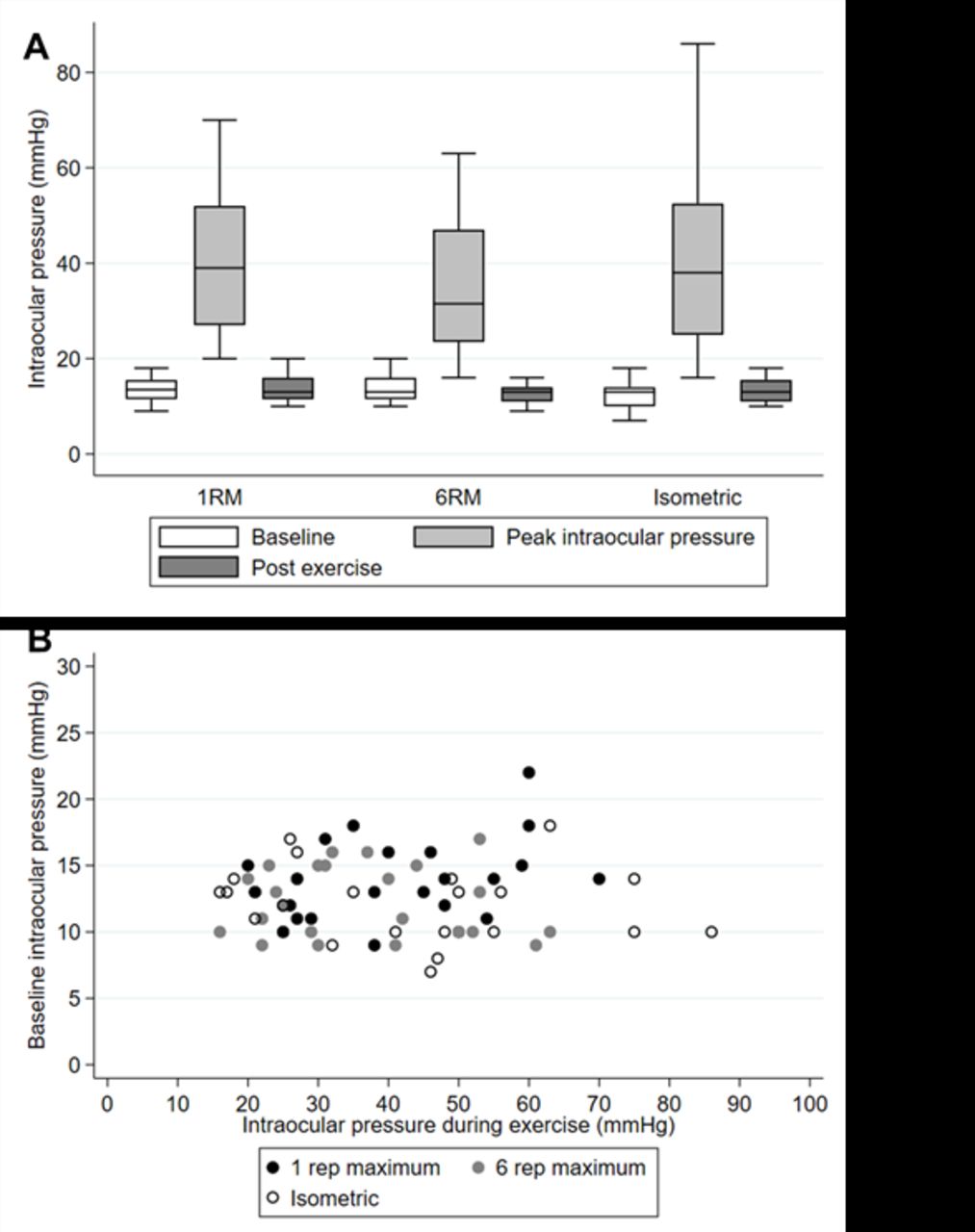
The IOP measurements at baseline, peak and post exercise, during 1RM, 6RM and ISO exercises (A). The baseline IOP values are plotted against the peak IOP values for the 1RM, 6RM and ISO exercises (B). IOP, intraocular pressure; 1RM,one repetition using 95% maximal load; 6RM, six repetitions using 75% ofmaximal load.
{kind=link}
{kind=link}
{kind=link}
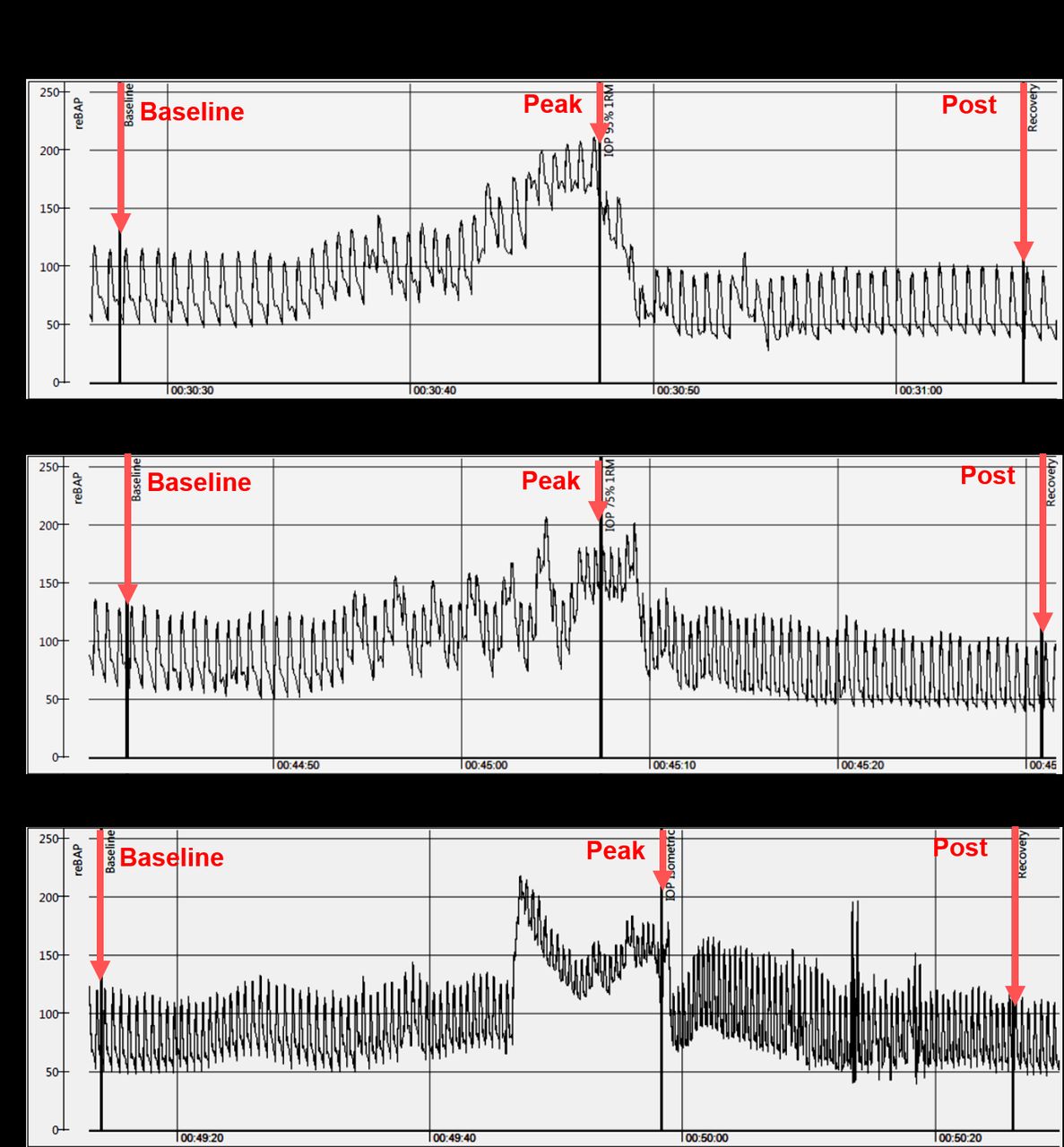
Blood pressure and HR monitoring output, which was time stamped with the participant’s lift and changes in the IOP. Different HR and blood pressure (SYS, DIA and MAP) patterns are observed for 1RM (A), 6RM (B) and ISO (C) exercises. The baseline IOP measurement was less than a minute prior to the peak IOP measure, and the post IOP measure was less than a minute from the peak IOP measurement. IOP, intraocular pressure; 1RM,one repetition using 95% ofmaximal load; 6RM, six repetitions using 75% ofmaximal load; ISO, isometric; HR, heart rate; MAP, mean arterial pressure; SYS, systolic pressure; DIA,diastolic pressure.
All values of IOP, SYS, DIA and HR were significantly higher during all three of the exercises (p<0.001 for all). Change in HR and DIA was greatest for the 6RM (p=0.001 and p<0.001, respectively). In the 6RM exercise, the ΔIOP was highly correlated with maximum weight lifted per BMI (p=0.00001) and ΔMAP (p=0.0003) (table 1).
The summary of recorded changes in intraocular and blood pressures, measured as a difference between the baseline and peak values recorded
Repeated measures multiple analysis of variance was used to see if the physiological changes differed between the three exercises. These results are reported in table 1. On multivariate regression analysis, for 1RM change in IOP was significantly associated with maximum weight lifted (t=5.66 p<0.001), ΔSYS (t=2.90 p=0.010), ΔDIA (t=2.82 p=0.013), ΔMAP (t=−3.21 p=0.005) but not ΔHR (t=1.48 p=0.150) (F=13.90 η2 0.794). The association was less strong for the 6RM change in IOP. On multivariate regression analysis, only ΔSYS (t=−2.52 p=0.020) and ΔMAP (t=3.94 p=0.001) were significantly associated with ΔIOP (F=14.88 η2 0.699). For the isometric exercise, only ΔDIA was significantly associated with ΔIOP (t=3.27 p=0.003) (F=10.70 η2 0.327).
Blood pressure changes
The ΔMAP showed significant correlation with ΔIOP change in all three 1RM (p=0.02), 6RM (p=0.0002) and ISO (p=0.03) exercises. The ΔMAP showed no correlation with participant demographics.
Retinal nerve fibre layer changes
OCT scans’ postexercise showed an average choroidal change of +3.39 μm±10.15 μm and an average retinal change of −0.45 μm±3.42 μm. The average choroidal thickening was highly correlated with retinal thinning (p=0.01) and especially the retinal ganglion cell layer complex (p=0.008). No significant difference with exercise was observed in retinal thickness (p=0.846), ganglion cell layer (p=0.777) or choroidal thickness (p=0.112)
Discussion
This study demonstrates that high-intensity weightlifting (leg press) results in dramatic and transient changes in IOP. During effort, IOP increases rapidly (~%200) in apparent association with parallel increases in systemic blood pressure. With cessation of effort, IOP and systemic blood pressure rapidly return to pre-effort values. We demonstrated that leg press results in a dramatic and transient increases in IOP across the 1 RM, 6 RM and ISO exercises with an average increase in 26.5 mm Hg to reach an IOP of 40.7 mm Hg, which normalised within seconds of release of the weight. Our study investigated three forms of resistance exercise: with 1RM representing primarily anaerobic activity, 6RM would have a combination of aerobic and anaerobic works and isometric has the highest Valsalva contribution of the three groups. There was also a concomitant increase in MAP of 77.0 mm Hg and HR of 33.2 bpm from baseline that also rapidly normalised on release of the weight.
The clinical implication of such repeated spikes in IOP has been an area of increasing interest. There is evidence that fluctuations in IOP may have an impact on the development of glaucoma.28 29 Acute transient spikes in IOP have been documented to occur while playing wind instruments and investigators have shown that high-resistance wind instruments were more likely to be associate with an abnormal visual fields with the degree of visual field defect being correlated with the cumulative practice time.30–35 Schumann et al31 measured IOP with pneumotonometry during playing a wind instrument and showed that IOP rose from 24 mm Hg to 46 mm Hg over a 12 s period. Schumann postulated that this increase in IOP was predominantly the result of the Valsalva Manoeuvre.31 Furthermore, there is accumulating data that rapid pressure transients may induce acute retinal ganglion cell damage. Resta et al36 found that applying 1 min of transient IOP elevation to levels of 50–90 mmHg in isolated retinas induces retinal ganglion cell (RGC) injury within 1 hour of application. Other investigators have also identified that transient spikes in IOP can cause temporary visual field deficits that usually recover to although permanent deficits by short but high pressure elevations have been shown.37 38
The mechanism of the spike in IOP in the present study, likewise, is most likely to be the result of Valsalva manoeuvre given the dramatic increase in IOP as well as the rapid return to baseline levels. The Valsalva manoeuvre involves exhaling forcefully against a closed glottis, which may lead to elevated IOP through a rise in intrathoracic pressure and compression of the intrathoracic venous system.39 40 Venous pressure rise is transmitted through jugular, orbital and vortex veins to the choroid, bringing about vascular engorgement, an increase in the choroidal volume and a rise in IOP.31 40 The postexercise choroidal measurements with the OCT were not statistically significant in our study, however, we did not measure choroidal thickness during exercise. In their investigation of wind instrument players, Schumann et al31 measured uveal volume with ultrasound during play and documented an increase in uveal volume. Further evidence that the Valsalva manoeuvre was involved in the present study is the concomitant increase in DIA during exercise.40 41 Similarly, Dimsdale and Nelesen reported a French horn player whose DIA rose in tandem with the frequency of the note he played.42
The venous pressure is also elevated in the episcleral veins with Valsalva manoeuvre, creating an increased resistance to aqueous outflow and causing a rise in IOP, although at a much slower rate than choroidal engorgement. However, the rapid rise in IOP and subsequent normalisation following release of the weight suggests that changes in episcleral pressure were not the main mechanism. Increased episcleral venous pressure acts as an increase in afterload to aqueous outflow, so the rate of IOP change would be dependent on the rate of aqueous humour formation as well, which is unlikely to significantly change in the time frame of seconds.
Other mechanisms have been proposed to explain the increase in IOP during Valsalva maneouvre. Racynski et al43 reported that an increase in IOP during the Valsalva manoeuvre was related to an increase in electromyographic activity.43 It has also been suggested that the extraocular muscles play a role in the increase in IOP that is known to occur during lid squeesing.44 Others have suggested a role for the autonomic nervous system.42 Sun et al have shown that the expansion and collapse of Schlemms canal during the Valsalva manoeuvre may arise from autonomic nervous system activity as well as the changes in blood flow.
Other investigators have studied the effects of weightlifting and IOP.11 19 25 45–49 Vera et al have extensively evaluated different aspects of the impact of weight lifting on IOP. They have demonstrated that the execution of 1 min isometric squat exercise resulted in an IOP rise of approximately 8 mm Hg at the end of the 1 min effort, once the weight is released.26 They have also observed that there is a progressive IOP increment with increasing repetitions with the magnitude of the increase in IOP being dependent on the type of exercise.25 The investigators have also studied the IOP during 2 min of isometric exercises and observed an increase in IOP of 25% from baseline.11 The difference in their finding and ours can be attributed to the variation in instruction to the participants. Vera et al advised the participants to keep a constant pattern of breathing during the hold while our participants were allowed to perform the test with the regular breathing technique.49 50 Here, the participants were performing lifts that were very close to their maximal effort, and the chances of failure (of the rep) were high. So long that the participants performed the repetition with good form, they were not told how to breathe during the exercise. It should be noted, however, that lifting weights close to maximal effort always include an abdominal ‘bracing’, which also always includes a Valsalva Manoeuvre. In our observation, all of our participants ‘braced’ during the performed reps and performed Valsalva Manoeuvre. Our findings complement their observations that the spike in IOP is a combination of complex interaction of variables including, the increase in the MAP, magnitude of weight being lifted and the degree of Valsalva Manoeuvre.
The investigations that have evaluated the role of Valsalva maneouvre on IOP have involved a range of methodologies.31 32 40 51 52 A simulation of the Valsalva manoeuvre by tightening a rope around the waist also showed the increases in IOP.53 IOP was measured during Valsalva by Mete et al.54 Valsalva manoeuvre was performed in the sitting position while the patient was blowing in a mouthpiece attached to a manometer. IOP was recorded before and during Valsalva once the manometer reading achieved 35–40 mm Hg. With this technique, the mean IOP increased from 15.7 mm Hg to 20.4 mm Hg. Some studies have suggested that IOP may increase with weightlifting independent of Valsalva Manoeuvre, with participants in several studies being instructed to avoid the Valsalva Manoeuvre. However, it cannot be excluded that Valsalva Manoeuvre was unintentionally used.19 31 45 55 This study was different to previous publications in three major ways. First, all previous studies have measured the IOP ‘during the set’ (ie, when the repetitions were finished and the load was racked). In this study, we measured the IOP ‘during the rep’ where the participants were still bearing the full load and muscular tension was at maximum. Second, in several previous studies, the exercises were mainly smaller muscle groups (eg, biceps, shoulders, etc), whereas in this study, we used the largest body muscle group (ie, legs). Finally, previous studies have used loads that were not close to 1RM of the participant and were in higher rep range (8–15). In this study, we focused on maximal effort using weights almost equivalent to 1RM, where the muscle loading and effort are close to participants’ maximum capacity.
Resistance training is recognised to cause acute rises in blood pressure.56 In the present study, MAP increased by an average of 77.0 mm Hg with the difference greatest for 6RM while HR increased by 33.2 bpm (again also greatest increase for 6RM). Such increases MAP and HR have been documented to occur with exercises involving Valsalva manoeuvre.57 Such acute haemodynamic changes are potentially clinically relevant. In terms of IOP, the increase in MAP means that ocular perfusion pressure is maintained (MAP–IOP).
This study has several limitations. This study has been carried out in a healthy young population, and, thus, the external validity of these results in glaucoma participants requires further investigation. While IOP was measured during exercise, the RNFL and choroidal thickness were measured with OCT, which was done several minutes following cessation of weightlifting (leg press). Therefore, it is possible that there were increases in choroidal thickness that occurred with Valsalva that were not identified by our methods. While this study documented dramatic increases in IOP during weight lifting, there is no evidence that these repeated spikes lead to glaucoma. A longitudinal study of weightlifters is warranted to answer this question.58 The participants in this study were all young and healthy volunteers with no evidence of glaucoma. It is unclear whether our results can be extrapolated to older individuals or those with established glaucoma. However, evidence to date suggests that there is no difference in increase in IOP during Valsalva Manoeuvre in participants with and without glaucoma.39 40 59 60 Other investigators have identified that the fitness levels of the participants influences the changes in IOP with exercise. All our participants were individuals who undertook weightlifting at least three times per week. Vera et al have demonstrated that highly fit participants show more stable IOP behaviour and, therefore, it is possible that our findings underestimate the IOP spike in those who do not undertake as regular exercise.45 47 61
In conclusion, IOP increases dramatically through all forms of resistance that involves the Valsalva Manoeuvre which rapidly normalises to baseline. These IOP spikes might have implications for developing glaucoma in weightlifters over long term. It remains unclear whether regular repetitive IOP spikes are damaging to individuals who have no features of glaucomatous optic neuropathy or who have a family history. However, we would suggest that it is important to discuss the spike in IOP with glaucoma participants or in those in whom IOP fluctuations are undesirable. However, this is an area that requires further investigation, in particular, given the increased popularity of weightlifting among all ages.
Data availability statement
Data are available upon request.
Ethics statements
Ethics approval
This study was approved by the University of Auckland Human Participants Ethics Committee (UAHPEC ref number 022578) and participants provided written informed consent.
Acknowledgments
We wish to thank Rosemary Kim, Kevin Li, Lisa Lim, Winnie Ye and Vlad Zorzoliu who assisted in patient recruitment and data acquisition.
References
Footnotes
Contributors EV and CS designed and supervised the experiments. SR, TS and VB provided expertise and supervision in Sports Science field. GP and RLN provided optometric and statistical expertise. HD-M and EV drafted the paper and supervised its progress through submission and revisions
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.