Article Text

Abstract
First-line treatment of centrally involved diabetic macular oedema (CI-DMO) is often with an anti-vascular endothelial growth factor (anti-VEGF) agent. Although this can provide efficacy in the majority of eyes, a sizeable proportion do not respond sufficiently and many continue to receive anti-VEGF therapy after it may be optimal. This imposes a treatment burden on both patients and clinicians and, most importantly of all, can be sight threatening. Changing treatment to an intravitreal corticosteroid implant at the appropriate time may help optimise patient outcomes and reduce injection frequency, thereby reducing treatment burden.
Eight retina specialists convened to discuss how to ensure eyes with CI-DMO receiving intravitreal anti-VEGF therapy are evaluated for a potential change to intravitreal corticosteroid therapy at the most effective time in their treatment journey. They concluded that clear criteria on when to consider changing treatment would be helpful and so developed a consensus guideline covering key decision points such as when and how to assess response to anti-VEGF therapy, when to consider a change to corticosteroid therapy and when and how to assess the response to corticosteroid therapy.
The guideline was developed before the COVID-19 pandemic but, with the additional challenges arising from this including even greater pressure on clinic capacity, it is more important than ever to reconsider current working practices and adopt changes to improve patient care while also easing pressure on clinic capacity, reducing hospital visits and maintaining patient safety. This publication therefore also includes suggestions for adapting the guidelines in the COVID-19 era.
- macula
- retina
- treatment medical
- vision
- drugs
- COVID-19
- intraocular pressure
- inflammation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Tailoring treatment to pathophysiology in diabetic macular oedema
Diabetic macular oedema (DMO) is the main cause of vision loss in patients with diabetes.1 Depending on glycaemic control and the treatment given, the effects of DMO can range from being fully reversible with an apparent restoration of normal visual function to persistent severe oedema with progressive visual loss.2 Early intervention may help prevent permanent visual loss.2
DMO has a multifactorial pathophysiology and can involve angiogenesis, increased vascular permeability and inflammation. A breakdown in the blood-retinal barrier causes intracellular and extracellular accumulation of fluid and lipid exudates in the retina, which leads to retinal thickening and oedema.3 Loss of visual acuity correlates with central macular involvement, and with the degree and duration of central macular thickening,2 and the goal of therapy is to preserve or improve retinal function and vision by reducing retinal thickening and oedema.
Although the exact mechanisms involved in the pathogenesis of DMO are unclear, it is believed that upregulation of several angiogenic and inflammatory cytokines contributes to the disruption of the blood-retinal barrier and that the balance between angiogenic and inflammatory mechanisms may change with time as DMO progresses. Thus, acute inflammation and vascular dysfunction may characterise early DMO and chronic inflammatory mechanisms may be more prominent in later disease.4 5 Theoretically, clinical outcomes could therefore be optimised by tailoring treatment to the predominant pathology—with treatment changing to match the pathology. In practice, we are unable to determine which pathology is most clinically relevant at a particular time6 other than by evaluating the response to different treatments that have different mechanisms of action. However, patients who are refractory to one treatment may benefit from changing to a different agent.5
In the UK, first-line medical therapy for centrally involved DMO (CI-DMO) is generally an intravitreal anti-vascular endothelial growth factor (anti-VEGF) agent if central retinal thickness (CRT) is ≥400 µm.7 This is usually ranibizumab or aflibercept, although bevacizumab is also used off-label in some centres (table 1). The relative effectiveness of these agents appears to depend on baseline visual acuity; although they are similarly effective when the initial visual acuity is 69–78 letters, when initial visual acuity is <69 letters, aflibercept is significantly more effective than bevacizumab at 1 and 2 years and significantly more effective than ranibizumab at 1 year but not 2 years.8 9
Intravitreal treatments for diabetic macular oedema (DMO)
DMO is not solely due to increased VEGF levels and VEGF-independent inflammatory pathways are important too.10 If anti-VEGF treatment is contraindicated or does not achieve a sufficient response (despite an appropriate injection frequency and regular monitoring), then intravitreal corticosteroid implants (dexamethasone or fluocinolone acetonide) are indicated (table 1). Current guidance from the National Institute for Health and Care Excellence (NICE) stipulates that these corticosteroid implants are funded in eyes with DMO only if they are pseudophakic. Thus, phakic eyes requiring cataract surgery will qualify once the surgery is performed.
A significant proportion of eyes with DMO are insufficiently responsive to anti-VEGF treatment.11–14 Up to 40% of eyes show only a minimal response (<5 letter gain) in best corrected visual acuity after 3 months and only a minority of these eyes (~20%–30%) are expected to develop a clinically significant visual response with continued intensive anti-VEGF treatment over the following 1–3 years15—thus, the early response to anti-VEGF helps predict the longer term response to anti-VEGF treatment in the majority of patients.
Reducing the duration and/or severity of macular oedema during the first year of anti-VEGF therapy appears to have greater prognostic importance than merely reducing macular thickness, perhaps because the presence of chronic oedema signifies a transition from the acute inflammation and vascular dysfunction characteristic of early DMO to the chronic inflammation of later DMO.16 Potentially, the retinal response to anti-VEGF treatment changes as DMO pathophysiology evolves16 and an insufficient response may signify a shift to a more chronic phenotype.4
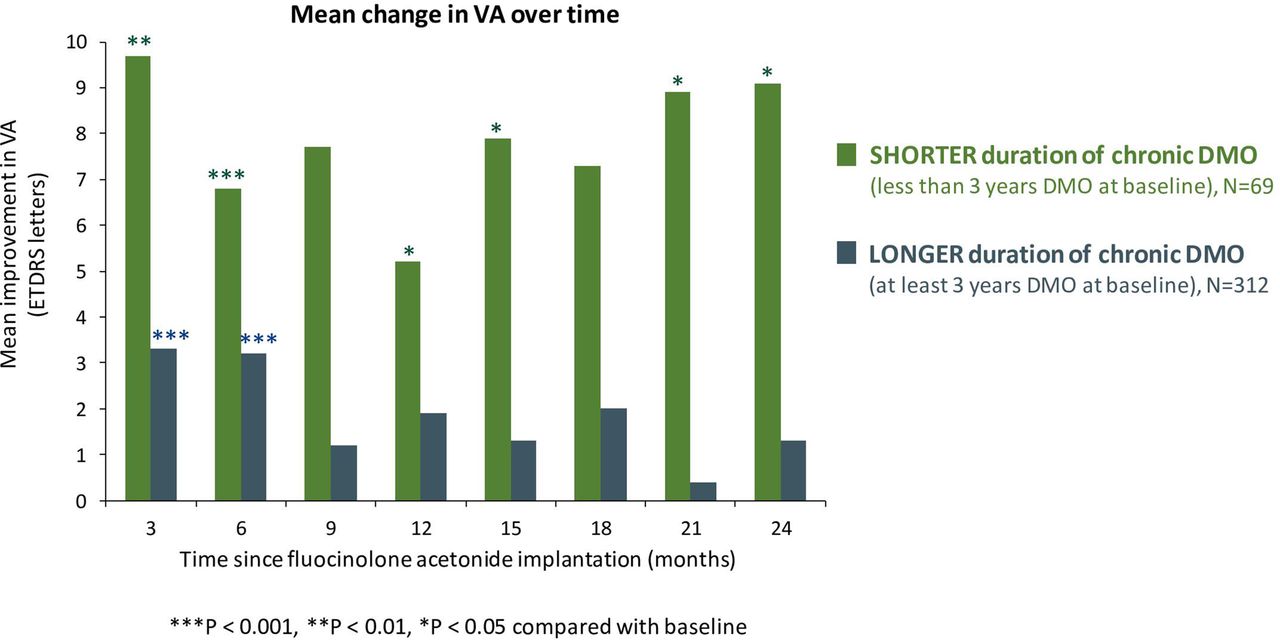
Eyes that are insufficiently responsive to anti-VEGF or have persistent or recurrent DMO despite treatment may benefit from an alternative treatment strategy,17 including possibly a change to intravitreal corticosteroid treatment. However, as functional responses to corticosteroid therapy also appear to wane with longer durations of chronic DMO (figure 1),18 there is a need for timely initiation of corticosteroid therapy to reduce the risk of premature, avoidable and irreversible vision loss. Especially in clinics with a high-throughput anti-VEGF service, it can be easy to default to the status quo of continuing with the existing treatment and miss the optimal opportunity to change therapy.
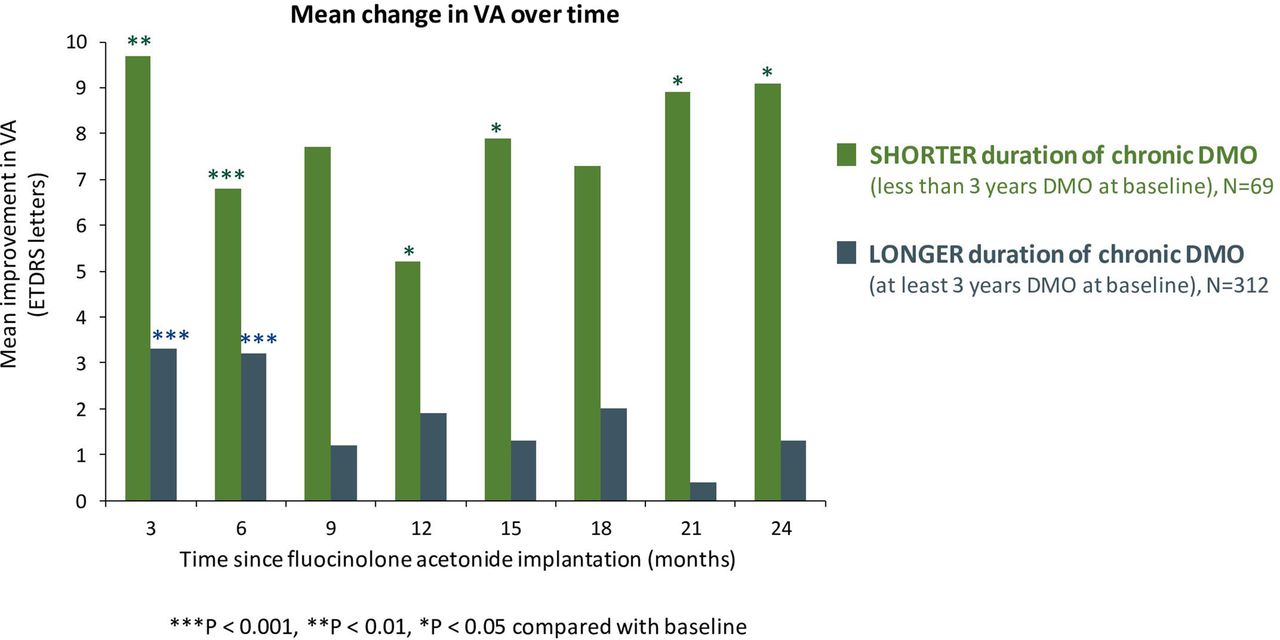
Improvement in visual acuity (VA) following fluocinolone acetonide implantation is greater when the duration of chronic diabetic macular oedema (DMO) at baseline is shorter (<3 years) rather than longer (≥3 years). (18, Data on file, Alimera Sciences, 14 March 2017) Adapted by permission from BMJ Publishing Group Limited. [British Journal of Ophthalmology, Chakravarthy U, Taylor SR, Koch FHJ, et al. 103,1072–7, 2019]18. ETDRS, Early Treatment Diabetic Retinopathy Study.
If a risk-to-benefit assessment of overall retinopathy status (including peripheral and proliferative retinopathy in addition to CI-DMO) concludes that intravitreal corticosteroid therapy would be appropriate, then the challenge for clinicians is to determine when it needs to be introduced to ensure patients are always receiving the most effective treatment. There is evidence that persistent abnormal pooling of extracellular fluid alters the spatial relationships between different retinal neuronal components and may destroy the connection between photoreceptors and ganglion cells in the neuroretina.19 Once such anatomical degradation has occurred, vision is likely to deteriorate irreversibly. Hence, it can be counterproductive to continue anti-VEGF therapy for too long if this prevents the chance of clinical benefit from a corticosteroid from being fully realised.
Although NICE guidance20 recommends dexamethasone and fluocinolone acetonide implants for patients with DMO who have failed to show a sufficient response to previous treatments, it does not provide any detail regarding what constitutes an insufficient response and at what point in the natural history of DMO treatment this assessment should be made. There is, therefore, an unmet need for clear and practical guidance on when to consider the option of corticosteroid treatment. Without this, continuing anti-VEGF treatment for longer than is warranted or beneficial can be detrimental in the long term for both clinical outcomes and healthcare resources. Although data from Protocol U have provided some evidence for the value of combining therapies (off-label treatment),21 robust data regarding switching between therapies are lacking and additional guidance regarding this is needed.
The aim of this paper is not to provide a comprehensive comparison of the advantages and disadvantages of the available treatment options but to offer evidence-based practical guidance on how insufficient response can be defined and when it is best to consider alternative options. Any recommendation for when to consider changing treatment cannot be taken in isolation without an evaluation of the potential risks and benefits. For intravitreal corticosteroid therapy, potential risks include increased intraocular pressure (IOP), glaucoma development and, in patients with a phakic lens, cataract formation. However, these are typically manageable and should be considered in the context of insufficiently treated DMO. The risk of raised IOP can be mitigated by appropriate patient selection (individuals with a history of elevated IOP being at higher risk for another rise)22 23 and, if IOP does increase, it can be managed with medication (in the majority of cases) or surgery.17 18 Similarly, cataracts—which are typically already present or developing in a significant proportion of patients with DMO—can be resolved with routine surgery.17
Consensus guideline
A group of eight retina specialists convened to discuss how to ensure patients with DMO receive the most appropriate intravitreal therapies at the optimal time in their treatment journey. These clinicians are senior medical retina specialists in large National Health Service trusts in the north of England. The group held two face-to-face meetings in York (in June and September 2019) and two teleconferences (in February and June 2020). They agreed that, in general, ophthalmology services have been focused mainly on service developments and expansions to manage the significant extra workload since the introduction of anti-VEGF treatments in recent years. They expressed concern that insufficient attention has been paid to considering clear guidance for appropriate timely conversion of patients with DMO and an insufficient response to anti-VEGF treatment to other alternative treatments such as intravitreal corticosteroid therapy. As a result, there is a risk that patients may continue to receive anti-VEGF treatment after it has failed to produce a sufficient therapeutic benefit.
Root causes for clinicians failing to consider a change from anti-VEGF to intravitreal corticosteroid therapy in a timely manner in DMO were identified, including: a lack of awareness of the benefits of early versus late treatment with corticosteroid; a lack of clear service protocols defining adequate response and clarifying when anti-VEGF should be discontinued; a lack of clarity over the exact meaning of ‘insufficiently responsive’ in labelling information for corticosteroids24 25; difficulty in easily identifying (in terms of lens status) which patients should be considered for a change; inertia and problems in changing staff habits away from the routine use of regular anti-VEGF injections; pressures on staff time; and the need for ophthalmologists to be available to inject corticosteroid implants.
The group concluded that clear guidance on when to consider changing DMO therapy would help address the problem and, as a result, developed a consensus guideline (figure 2). The guideline covers key decision points such as when and how to assess a patient’s response to anti-VEGF therapy, when to consider intravitreal corticosteroid therapy and when and how to assess the response to corticosteroid therapy. In essence, the guideline recommends that anti-VEGF therapy should be assessed after the initial three to six monthly injections and a change in therapy considered if the eye shows <20% reduction in CRT and <5 letters gained from baseline. If anti-VEGF therapy is continued, it should be assessed again at 24 months (or earlier if services have been interrupted) when, if injections in the preceding 12 months have been more frequent than every 8 weeks, a change in therapy should be considered. Corticosteroid therapy response should be assessed at 8-week intervals and clinicians should consider the advantages and disadvantages of a longer acting versus shorter acting corticosteroid implant. For example, even though a longer acting implant can help minimise the treatment burden for patients and clinics and ensure continuity of treatment during exceptional circumstances such as pandemics where timely retreatment may not be possible, any adverse events may be longer lasting.
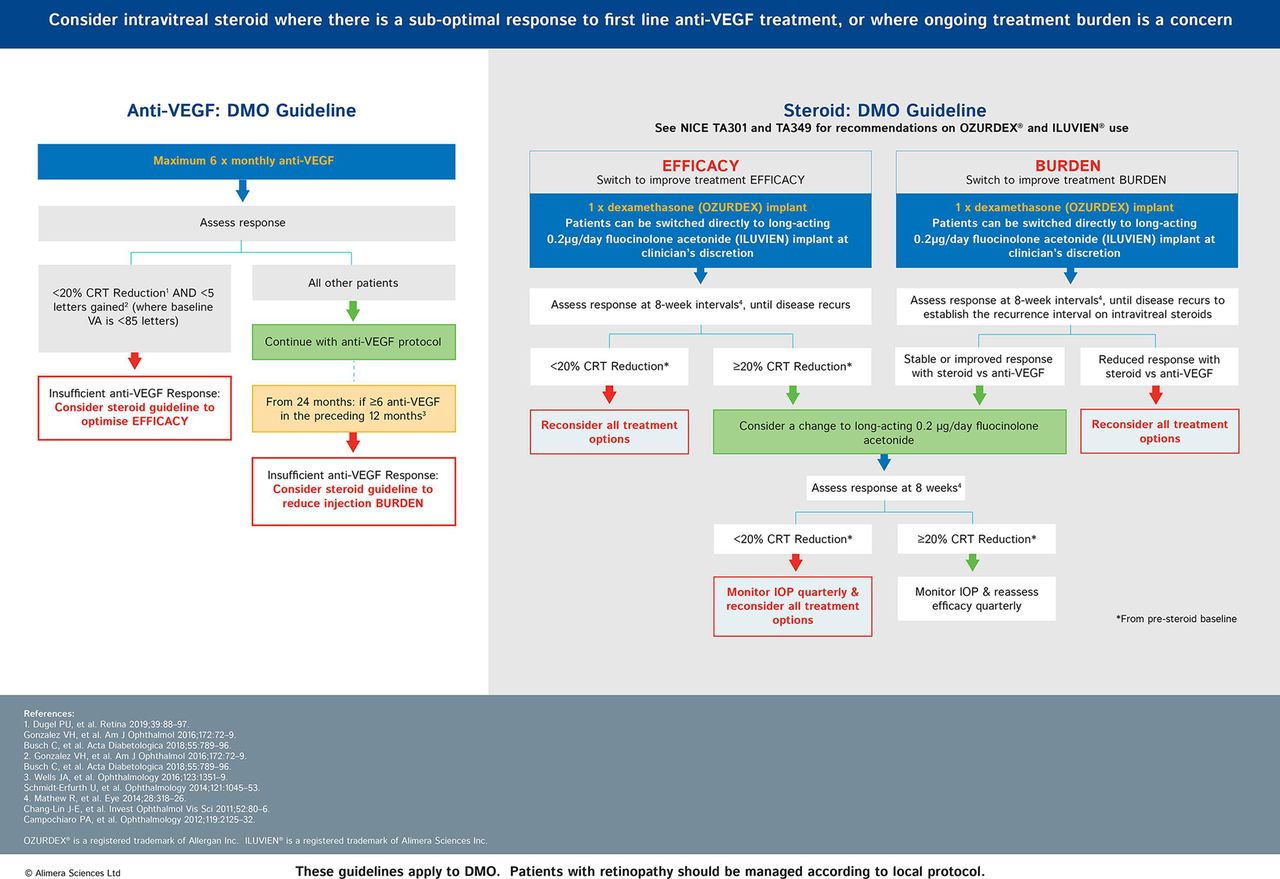
Consensus guideline for anti-VEGF and corticosteroid treatment of diabetic macular oedema (DMO). The guideline refers only to DMO and does not consider proliferative retinopathy, so treatment for this may need to be determined separately. CRT, central retinal thickness; IOP, intraocular pressure; NICE, National Institute for Health and Care Excellence; VA, visual acuity; VEGF, vascular endothelial growth factor.
The need for the guideline was confirmed at a webinar introducing it to ophthalmology staff across the UK and Ireland in July 2020, where 89% of more than 100 attendees who voted reported that it would be useful either in its current form or with local adaptation (H Devonport, personal communication, 2020). Details explaining the components of the guideline, together with the evidence supporting each decision point, are summarised below. Note that the guideline refers only to DMO and not other potential complications of diabetic retinopathy such as proliferative retinopathy.
When should response to anti-VEGF treatment first be assessed?
The optimal time to consider a change to corticosteroid treatment in DMO depends on a patient’s response to anti-VEGF treatment. However, the time point at which this is assessed varies between clinicians. Some may determine this after three injections of anti-VEGF at monthly intervals and some will continue for up to six injections.
Evidence supporting an evaluation after 3 months comes from Protocol I data which showed that the CRT response to anti-VEGF at week 12 is a significant prognostic indicator of medium-term to long-term anatomical outcome in CI-DMO.11 Eyes with a poor anatomical response to ranibizumab (ie, CRT reduction <20%) at 3 months were less likely to show a strong anatomical response in the longer term than eyes that had shown a strong response at 3 months (≥20% CRT reduction was achieved at 1 year in 31% of the early poor responders vs 84% in the early strong responders, and 52% vs 83%, respectively, at 2 years).11 Functional response data from Protocol I also showed that, among eyes with an early suboptimal functional response to ranibizumab (<5 letter improvement at 3 months), 63% continued to have a suboptimal functional response after 6 months of treatment and 53% continued to have a suboptimal functional response after 3 years of treatment (figure 3).15 As a result, continuing treatment beyond 6 months in this cohort imposes a large treatment burden with only modest benefit.

Long-term best corrected visual acuity outcomes among 135 eyes with an early suboptimal functional response (<5 Early Treatment Diabetic Retinopathy Study (ETDRS) letter improvement at 12 weeks) to intravitreal ranibizumab treatment+prompt/deferred laser treatment. After 6 months of treatment, 63% continue to have a suboptimal functional response and, after 3 years of treatment, 53% continue to have a suboptimal functional response.15 Continuing treatment beyond 6 months therefore imposes a large treatment burden with only modest benefit. BCVA, best corrected visual acuity.
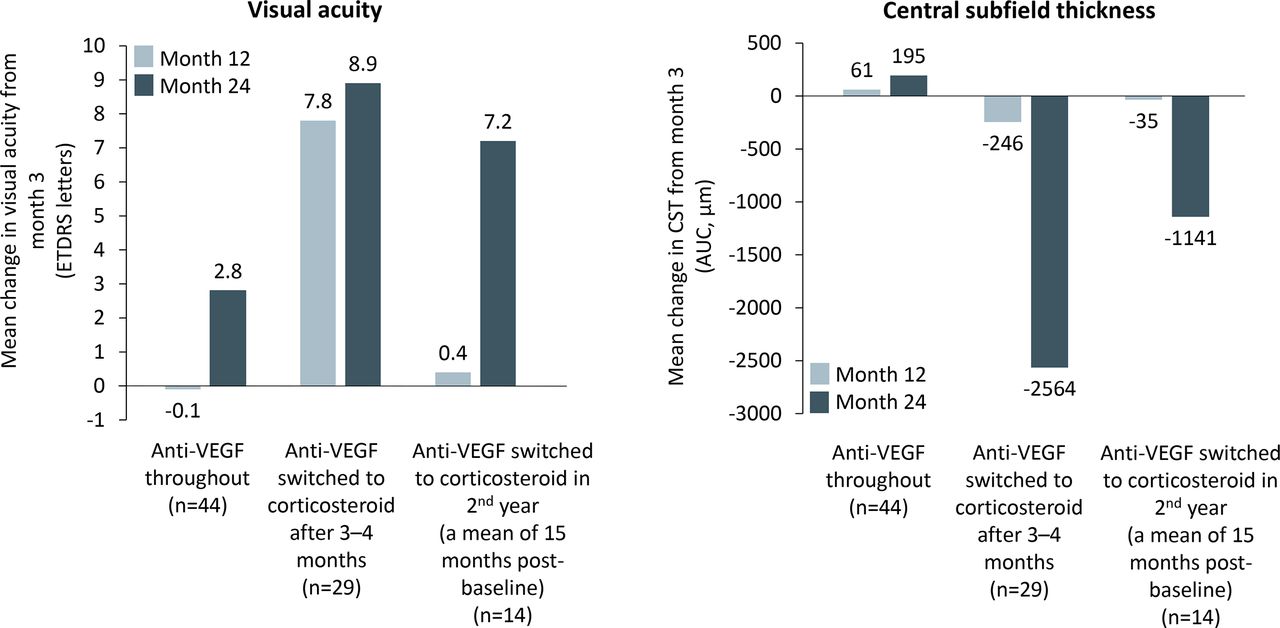
Although continuing anti-VEGF treatment beyond 3–6 months may elicit some further clinical improvement in a proportion of patients, this would be uncertain and potentially slow15—and therefore may fall short of the therapeutic objective of achieving timely elimination of subretinal and intraretinal fluid.11 Clearly, delaying a change to an alternative treatment in insufficiently responding eyes risks losing valuable time and may result in avoidable vision loss. The clinical benefits of a timely change have been confirmed in a real-world setting. For example, data from a retrospective, multicentre, case–control study confirmed that eyes with DMO considered refractory to anti-VEGF therapy after three monthly injections show better visual and anatomical outcomes at 12 and 24 months if they are moved to intravitreal corticosteroid treatment at 3 months than if they continue treatment with anti-VEGF therapy (figure 4).26 27

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean change in visual acuity and central subfield thickness (CST) after eyes with diabetic macular oedema (DMO) refractory to 3 months of anti-VEGF treatment (ie, achieving ≤5 letter gain in visual acuity or <20% reduction in CST from baseline) followed one of three treatment paths: continuing on anti-VEGF treatment, switching to dexamethasone treatment after months 3–4 or switching to dexamethasone during the second year of treatment. At months 12 and 24, visual acuity showed a mean change from month 3 of +7.8 and +8.9 letters, respectively, if eyes were switched to the corticosteroid after months 3–4, compared with -0.1 and +2.8 letters, respectively, if they had continued anti-VEGF therapy. For CST, standardised area under the curve (AUC) values over months 3–12 and 3–24 were calculated using the Trapezoid rule. These values showed a mean change in CST of -246 and -2564 µm, respectively, in eyes switched to the corticosteroid after months 3–4, compared with +61 and +195 µm in eyes that had continued anti-VEGF therapy.27 ETDRS, Early Treatment Diabetic Retinopathy Study; VEGF, vascular endothelial growth factor.
How should ‘insufficient response’ to anti-VEGF treatment be defined at the initial assessment (after three to six injections)?
Our guideline adopted a definition for insufficient response that included ‘<20% reduction in CRT and <5 letters gained’ from baseline. This conforms with the thresholds used in the analysis of Protocol I data (which termed <20% reduction in CRT a ‘limited early CRT response’ and ≥20% reduction in CRT a ‘strong early CRT response’).11 It is also consistent with the criteria used in a retrospective chart review focused on refractory DMO (where a suboptimal response was defined as <20% reduction in central subfield thickness (CST) on spectral domain optical coherence tomography or ≤5 letter gain).27
Some reports in the literature have used other definitions (eg, Protocol T defined lack of improvement as <5 letters or <10% reduction in CST28 and Pieramici et al used CST >300 µm and ≤10% reduction in CST in their definition of a limited early response).14 Although appropriate in the context of a highly controlled clinical trial environment,29 we consider that <10% reduction in retinal thickness may not be clinically meaningful or broad enough to ensure clear differentiation in real life and that failure to reach a 20% threshold would be more predictive of a poor response in the longer term.
How should ‘insufficient response’ to anti-VEGF treatment be defined after longer term treatment?
The guideline considers eyes to be insufficiently responsive to anti-VEGF if, at an assessment at the end of the second year of anti-VEGF treatment, they have been given six or more anti-VEGF injections in the preceding 12 months. This was informed by results from Protocol T and the RESTORE extension study where it was shown that the number of anti-VEGF injections received in the second year of treatment was a median of 5–6 (in Protocol T)9 or a mean of ~3.7 (in the RESTORE study).30
In line with this evidence, the reassessment of efficacy is recommended 2 years after the initiation of anti-VEGF therapy so that the number of injections in the second full year of anti-VEGF therapy can be evaluated. A reassessment at 18 months rather than 2 years would also be possible but was not chosen for the guideline for reasons of simplicity and in order to align with time points at which usage data are more usually published. Nevertheless, to ensure optimal outcomes, it is important that persistent oedema and the frequency and burden of anti-VEGF injections are monitored on an ongoing basis and not just at the 2-year review point.
When should response to corticosteroid treatment be assessed?
The guideline recommends that the response to intravitreal corticosteroid treatment is assessed at 8-week intervals, a time point which is based on the results of phase III studies with both dexamethasone and fluocinolone acetonide implants.3 31 32 With dexamethasone, the maximum reduction in CST has been shown to occur at 8 weeks and the maximum mean visual acuity at weeks 8–12.31 Similarly, with fluocinolone acetonide, the majority of the improvement in both anatomical and functional measures is evident by month 2.17
When should a long-acting corticosteroid be considered versus a short-acting corticosteroid?
Our guideline (and NICE guidance) leaves the choice of which corticosteroid therapy to use in DMO to the clinical judgement of the physician. The two intravitreal corticosteroid implants approved for DMO in the UK have different durations of actions, and one or the other may be more appropriate initially depending on the patient and clinical environment.
There are no published pharmacokinetic studies for the dexamethasone implant (OZURDEX, Allergan, Marlow, UK) in human eyes3 but, in animal eyes, the implant has been shown to release dexamethasone in two phases—the first phase provides a high dexamethasone concentration in the vitreous for approximately 2 months and the second phase provides a considerably lower dexamethasone concentration (vitreous levels decline by approximately 100 000-fold between months 2 and 3 and are below the limits of detection by 6 months).33
The ILUVIEN implant (Alimera Sciences, Aldershot, UK) is designed to deliver 0.2 µg of fluocinolone acetonide each day for up to 3 years. The release profile is flatter than that of dexamethasone with mean aqueous levels of fluocinolone acetonide in human eyes being 2.2 ng/mL at 1 month, 1.8 ng/mL at 3 months and 0.5–1.2 ng/mL between 6 and 36 months.34 There is, therefore, less than a fivefold variation in mean aqueous levels over the 3-year life of the implant—which helps ensure that the retina is treated continually and more consistently, rather than in periodic bursts. In a small number of patients reported as having received a dexamethasone implant initially and a fluocinolone acetonide implant subsequently, outcomes after each have been similar (although sustained long-term effects were achieved only with the fluocinolone acetonide implant).22
Although corticosteroid implants can result in elevated IOP in some patients, appropriate patient selection may ameliorate some of this risk because data suggest that the occurrence of prior IOP events (regardless of whether a patient has previously received a corticosteroid implant or not) may be a good predictor of subsequent IOP events with a corticosteroid implant.22 23 Patients who do not show a significant rise in IOP with previous corticosteroid treatment have a positive predictive value of 80% for the maximum observed IOP not exceeding 25 mm Hg with the fluocinolone acetonide implant.35 Furthermore, the positive predictive value is no higher with multiple versus single prior dexamethasone implants.35 Even if IOP does increase, this is generally manageable with topical medication and/or surgery.18 23
Adaptations in the COVID-19 era
Our consensus guidelines were developed before the COVID-19 pandemic affected the delivery of ophthalmological services. However, even before the pandemic, ophthalmology was the busiest specialty in England with the highest number of attendances for outpatient appointments36 and delays in hospital eye care services were resulting in permanently reduced vision in some patients.37 As the most common cause of delay is in regard to follow-up appointments,37 it is clear that this is an area where improvement needs to be a priority, particularly as an intensive intravitreal regimen has a considerable effect on patients’ quality of life and increases the risk of patient non-adherence.38 The additional pressures on the system brought by the pandemic—including a reduction in capacity due to social distancing and staff sickness, and a desire among patients with diabetes (who are at greater risk of COVID-19 complications) to attend hospital less frequently—mean that it is more important than ever to reconsider working practices and adopt whatever changes can help optimise patient care while easing pressure on clinic capacity.
While the pandemic persists, many adaptations may be necessary to facilitate social distancing and mitigate the effects of staff shortages. Within our consensus group, strategies included reducing the frequency of clinic attendances, reducing the number of patients allowed in waiting areas, offering weekend appointments, reducing the number of slit-lamp examinations, switching to therapies requiring fewer intravitreal injections, transferring some services to community facilities, taking consents by telephone prior to clinic visits, providing a helpline for patients, asking patients to proactively self-report the effects of treatment, monitoring patients virtually and with non-contact tonometry and providing pressure-lowering drops prophylactically if there is a risk the patient might not attend for an IOP check. Depending on the local situation the transfer of some services to the community may help reduce the need for patients to use public transport and keep a geographic separation from hospital wards that may contain patients with COVID-19. However, community facilities may not be as well provisioned as hospital clinics in terms of personal protective equipment and the separation of care can create challenges in communication.
The authors’ suggestions for potential adaptations to the guideline are detailed in table 2. The practicality of these in individual clinics may be influenced by a patient’s lens status, patient preferences and a variety of local issues including availability of IOP monitoring, glaucoma support and cataract surgery.
Potential adaptations to the guidelines for DMO in the COVID-19 era
Inevitably, the pandemic has interrupted the treatment of many patients and suggestions for how to resume previous treatment are also included in table 2. However, while the effects of the pandemic remain, possibly the most prudent course of action would be to take a longer term view of therapy and plan current treatment in the anticipation of continued capacity issues and potential further treatment interruptions from future waves of the pandemic.39 Making best use of treatments with a longer duration of action would therefore be instrumental in minimising the number of future treatment visits, helping patients retain continuity of treatment in the event of further lockdowns or insufficient clinic capacity and minimising the backlog of untreated or undertreated patients.
Tips for facilitating the adoption of the guidelines
Anti-VEGF injections are the mainstay of treatment in eye clinics (being used in both DMO and age-related macular degeneration) and so most ophthalmology services have been designed around optimising anti-VEGF delivery. As a result, current processes in clinics may not be ideal for optimising corticosteroid delivery. It is worthwhile taking a little time to ensure that any challenges impeding adoption of the guidelines are resolved so that corticosteroid delivery is not marginalised in favour of the ‘treadmill’ of anti-VEGF injecting as the benefits of corticosteroid treatment can be profound for both patients and clinics. Furthermore, given that the incidence of diabetes-related complications is forecast to increase by 20%–30% in the first 35–45 years of this century,40 even clinics that are operating within capacity at the moment are likely to benefit from such ‘future proofing’ measures. With this in mind, we would recommend ensuring copies of the guideline are readily available in each injection room and holding local multidisciplinary training meetings in order to educate about the guideline, encourage consistent and confident decision-making and agree on any local adaptations that may be required.
Summary
Anti-VEGF therapy and corticosteroid therapy have different—although overlapping—mechanisms of action and so are thought to be optimally effective in different types of DMO pathophysiology. Ophthalmology clinics may be able to improve clinical outcomes in DMO by promptly identifying eyes not responding sufficiently to intravitreal anti-VEGF treatment and considering a possible change to intravitreal corticosteroid treatment where a risk-to-benefit assessment supports this. Real-life data have shown that a corticosteroid implant may offer greater clinical efficacy than continued anti-VEGF therapy in this scenario but the timeliness of such a change is important to avoid compromising long-term visual outcomes—it needs to occur while the macula is still capable of functional response, so anti-VEGF treatment should not continue so long that the window of opportunity for benefiting from a corticosteroid has passed. Although intravitreal corticosteroid therapy can be associated with a risk of increased IOP, glaucoma development and cataract formation, these are generally manageable with medication and/or surgery and should be considered in the context of insufficiently treated DMO.
As corticosteroid implants require injection considerably less frequently than anti-VEGF, their use can help clinics dramatically reduce the number of treatment visits needed. Although this is always welcome to ease capacity issues, it is especially valuable during a pandemic when clinics need to limit the number of patients in the clinic and the number of invasive procedures performed. After the treatment visit to inject the corticosteroid implant, a local pathway should be in place to mitigate the consequences of elevated IOP. This might include a two-stop system with patients monitored using non-contact tonometers in virtual clinics or by optometrists in community facilities to further help ease pressure on clinic capacity.
A consensus guideline is presented to offer clarity regarding when and how to change DMO therapy. Anti-VEGF therapy should be assessed after the initial three to six monthly injections and a change in therapy considered if the eye shows <20% reduction in CRT and <5 letters gained from baseline. If anti-VEGF therapy is continued, it should be assessed again at 24 months (or earlier if services have been interrupted) and, if injections in the preceding 12 months have been more frequent than every 8 weeks, a change in therapy should be considered. Response to corticosteroid therapy should be assessed at 8-week intervals and clinicians should consider the benefits of a longer acting versus shorter acting corticosteroid implant (including minimising the treatment burden for patients and clinics and ensuring continuity of treatment during exceptional circumstances such as pandemics where timely retreatment may not be possible) against the possible disadvantages including potential adverse events.
Acknowledgments
The authors are grateful to LD and HD for chairing the consensus group meetings; Yvonne Imrie (Alimera Sciences) for coordinating and helping to facilitate the meetings; and Gill Shears (Write on Target Ltd., Leighton Buzzard, Beds) for writing support.
References
Footnotes
Correction notice This article has been corrected since it was published. Figure 4 has been updated.
Contributors Organisation of meetings: Yvonne Imrie (Alimera Sciences). Discussion of topic and development of guidelines: all authors. Facilitation of discussions: LD, HD, Yvonne Imrie. Writing first draft of the manuscript: Gill Shears. Reviewing, critiquing and approving the manuscript: all authors, Alimera Sciences.
Funding Publication of this supplement is made possible by an education grant from Alimera Sciences (Aldershot, Hants). The overall project and this publication both received financial support from Alimera Sciences.
Competing interests All authors received remuneration for their contribution to this work from Alimera Sciences. LD reports honoraria from Allergan, Bayer, Heidelberg Engineering, Novartis and Roche, and travel grants from Allergan, Bayer and Novartis. HD reports honoraria and travel grants from Alimera, Allergan, Bayer and Novartis. RG reports grants and personal fees from Novartis and Bayer. MH reports honoraria and travel grants from Bayer, Alimera, Allergan and Novartis. VM reports travel fees from Bayer and personal fees from Novartis. RM reports honoraria and travel grants from Bayer, Allergan and Novartis. PS reports honoraria and travel grants from Bayer and Novartis.
Provenance and peer review Not commissioned; internally peer reviewed.