Article Text

Abstract
Objective Procuring an affordable eye mount that can stabilise a cadaveric eye and simulate a patient’s normal facial contours represents an ongoing challenge in the ophthalmology simulation wet lab, with notable limitations to all currently available commercial options. This project uses computer-assisted design and three-dimensional (3D)-printing techniques to tackle these challenges for ophthalmologic surgical training.
Methods and Analysis Proof-of-concept study. Using Autodesk Fusion 360, we designed and 3D-printed a modular device that consists of 11 pieces forming a head structure. Standard OR tubing and syringes were adapted to create an adjustable-suction system to affix cadaveric eyes. Further modular inserts were customised to house non-cadaveric simulation eyes.
Results Three-dimensional eye mount for procedures in ophthalmology (TEMPO) reliably fixed a cadaveric eye in stable position throughout surgical manipulation. Trainees were able to drape and practice appropriate hand positioning while corneal suturing. Overall, this model was affordable, at a cost of approximately $C200 to print. The modular nature renders individual pieces convenient for replacement and customisable to simulate regional anatomical variation and accommodate non-cadaveric eyes.
Conclusions TEMPO represents an affordable, high-fidelity alternative to existing commercially available eye mounts. It reliably fixates cadaveric and simulation eyes and provides an enhanced surgical training experience by way of its realistic facial contours. It is released as an open-source computer-aided design file, customisable to interested trainees with appropriate software and 3D-printing capacity.
- eye (globe)
- eye (tissue) banking
- medical education
Data availability statement
No data are available. Not applicable
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Various cadaveric eye mounts are available commercially but have numerous limitations, being costly, non-customisable and poorly replicative of real patient anatomy.
What are the new findings?
We designed and evaluated a three-dimensional-printed eye mount that simulates facial contours and provides stable eye fixation for cadaveric eyes. We found this to have numerous advantages over existing models in terms of anatomic fidelity, stability, accessibility and sustainability.
How might these results change the focus of research or clinical practice?
Surgical wet lab training is a key component in the learning process for ophthalmic surgeons. Our modular, open-source design provides an anatomic eye mount system that is customisable and affordable, even for low-resource settings.
Introduction
In the ophthalmology wet lab, various eye mounts are commercially available that function to stabilise cadaveric eyes for surgical practice. One such device is the Mastel-Mandell eye mount.1 This apparatus centres the eye in a plastic bulb holder on a flat polycarbonate sheet using suction (provided by a syringe and clamp). Its simple design allows for easy use and convenient transport, but the tubing of the vacuum system cannot be easily accessed for cleaning or replacement, posing a sanitary concern and limiting device lifespan. Moreover, its simplicity also limits fidelity: it is not possible for trainees to practice proper hand posture around a patient’s face—a major challenge in the surgical environment—with a flat surface eye mount.
More recently, Ramakrishnan et al designed a simple and affordable eye mount using a hollow iron cylinder with spring action syringe attached.2 With attached mask, this model is more anatomic and provides good stability for cadaveric eyes; however, the design is not available for customisation and replication, cannot accommodate non-cadaveric simulation eyes, and does not fully simulate the size or contour of a patient’s head.
Due to the lack of an acceptable mount system, trainees often resort to securing cadaveric eyes to foam mannequins or trial heads in the wet-lab environment. Although these provide an easily sourced and inexpensive mount that is relatively anatomic, there are many limitations to this approach. The eyes are often anchored by use of pins, which risks perforation of the globe or tape/elastics, which give poor fixation. Moreover, cadaveric eyes are hypotonic, necessitating repeated injection with saline to achieve physiologic intraocular pressure (IOP) and globe contours (a suction-based design, such as those outlined above, mitigates this issue). Finally, trainees must also carve out the space for the eye: this results in a cavity that is difficult to clean. Cadaveric material is often retained in the mount, resulting in potential accumulation of biohazardous waste, and therefore, limited lifespan prior to disposal
Despite the limitations of the modalities available above, an open-source eye mount that simulates facial contours and affixes the cadaveric eye reliably is not yet available. Here, our goal was to design an innovative and affordable modular three-dimensional (3D)-printed cadaveric eye mount, complete with humanoid facial features to better simulate surgical ergonomics and teach proper hand positioning in the wet lab. Secondary objectives included creation of a mount that was modifiable, portable, environmentally conscious and modular to allow increased lifespan and ease of cleaning.
Materials and methods
Computer-assisted design
Using Autodesk Fusion 360 (California, USA), our team created a digital markup for our project titled three-dimensional eye mount for procedures in ophthalmology (TEMPO) (figure 1A). Facial contours for our model were created in Autodesk based on a pre-existing male model face used in the hockey industry for the fitting of hockey protective equipment. The goal of the modular design was to allow for easy modification of the head and facial contours with different components in the future, including the capacity to replace or redesign subcomponents easily, as necessary. The ability to readily deconstruct the mount also enables effective sanitisation post-use. The open-source design is included as a google drive file found at: https://www.ophthalmologyexplorer.com/innovations/project-one-7f9kx.

(A) 3D modelling the eye mount in Fusion 360 (Original photographs; Michael Mak holds copyright and grants permission for publication). (B) 3D printed modular pieces of the eye Mount (original Photographs; Michael Mak holds copyright and grants permission for publication). 3D, three deimensions.
Construction
The above design was 3D printed in a biodegradable polylactic material (ECOTOUGH PLA, Filaments, CA, Canada) using a commercially available 3D printer (Ultimaker 3, Geldermalsen, Netherlands) (figure 1B). Standard-bore surgical suction tubing, tubing clamps, and a 50 cc syringe were obtained from the local operating room (OR). A right-angle (90°) elbow tubing (sourced from a local automotive shop) was used to complete the suction circuit within the head enclosure. Several variations of the design were printed and prototyped to optimise the mount’s function. A separate modular insert was developed to accommodate a simulation eye (Simuleye, California, USA) and demonstrate the flexibility of TEMPO for use with non-cadaveric eyes.
Evaluation
Cadaveric human tissue was sourced from the local eye bank for evaluation and validation of the TEMPO model. In order for TEMPO (or any suction-based system) to provide good fixation and effective simulation of the contours and pressure of the in vivo eye using cadaveric material, saline must be injected into the eye, as they are hypotonous on delivery from the eye bank. Thus, 3–4 mL of saline was injected into the posterior compartment using a 30-gauge needle through the optic nerve head and the eye centred on the cylindrical flange; suction was drawn using the 50 mL syringe, and the overlying orbital rim housing placed prior to evaluation (see Youtube video link below for demonstration). The ability of the model to establish and maintain IOP was assessed using a handheld tonometer (Tonopen Avia, Reichert Technologies, New York, USA). Local surgical residents practised procedures including corneal and scleral suturing and construction of clear corneal incisions and were asked to compare the TEMPO model to other mount systems. The ease with which the model could be disassembled and sanitised was also assessed. A similar battery of tests was performed with the polymer simulation eye. Use of the TEMPO model, including assembly, suturing, and disassembly can be viewed in our YouTube video: (Link) https://www.youtube.com/watch?v=MWdjJjzAk8w.
Results
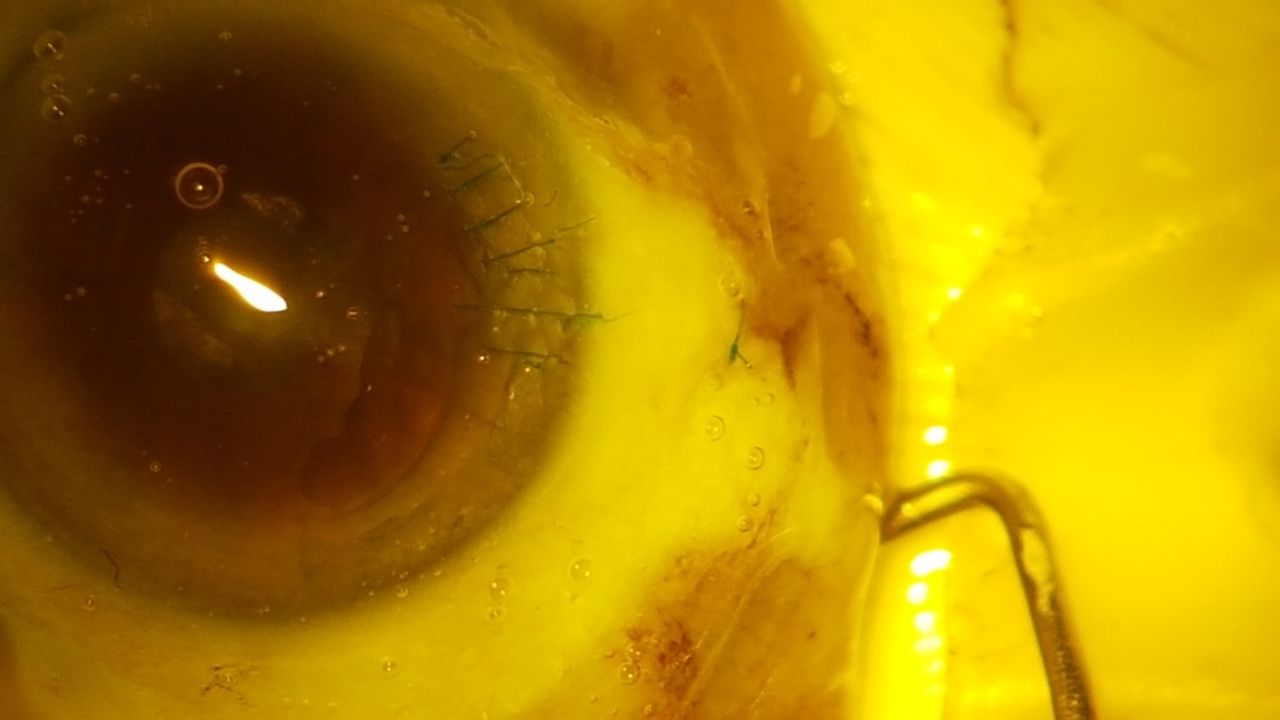
The final design for TEMPO was intuitive and convenient to assemble. Using the suction system, residents could easily position and fixate the saline-filled cadaveric eye (figure 2A). The eye in its ‘socket’ closely resembled how an eye would be viewed in the OR with a speculum in place, including extent of surgical exposure and degree of protrusion; the palpebral fissure opening was further customisable through modification of the orbital rim insert in Autodesk. IOP of 40–50 mm Hg was measured on application of suction: this could be stably maintained over the course of a 30 min suturing session without issue. Corneal suturing was achieved in a similar fashion to that of a human patient, and residents could practice correct hand position to efficiently complete a series of surgical tasks, including simple interrupted corneal sutures (figure 3). Cleanup was simple, where the eye could be released from suction and the mount disassembled to disinfect components independently (figure 4). The Simuleye could be similarly fixated in anatomic position in the TEMPO mount (figure 2B–D), and remained stable throughout a similar battery of surgical activities. The total cost of production for the TEMPO model as pictured in the here is approximately $C200 at current printing rates, and further modular inserts can be developed and customised at modest cost.
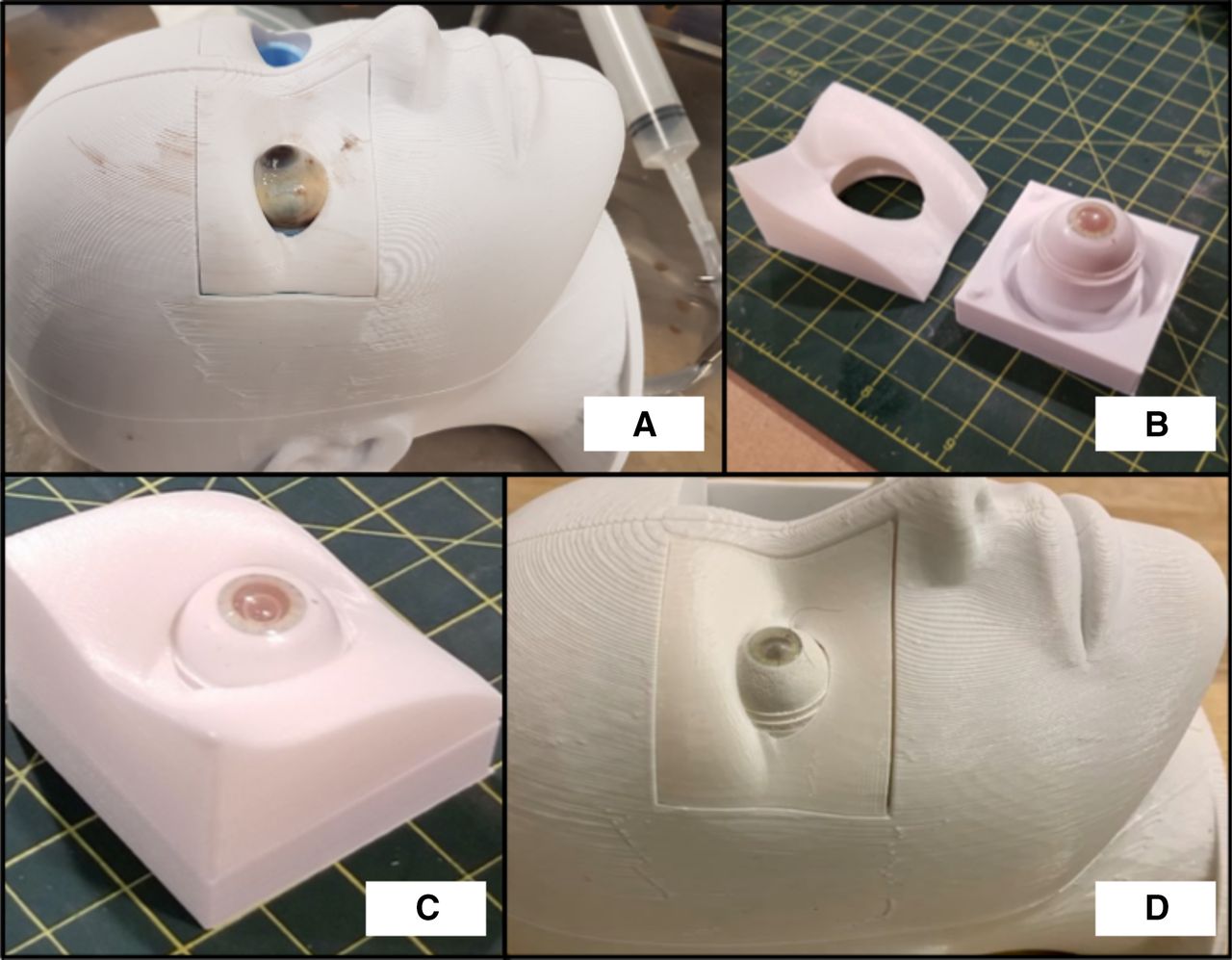
(A) OR suction tubing and a 50 CC syringe provide suction for the eye (original Photographs; Michael Mak holds copyright and grants permission for publication). (B) Modular encasing for Simuleye (disassembled) (original Photographs; Michael Mak holds copyright and grants permission for publication). (C) Modular encasing for Simuleye (assembled) (original photographs; Michael Mak holds copyright and grants permission for publication). (D) Fitting of modular encasing in tempo with Simuleye (original photographs; Michael Mak holds copyright and grants permission for publication). OR, operating room.

Corneal suture practice on cadaveric eye on TEMPO mount (original photographs; Michael Mak holds copyright and grants permission for publication). TEMPO, three-dimensional eye mount for procedures in ophthalmology.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Modular cleanup of TEMPO original photographs; Michael Mak holds copyright and grants permission for publication). TEMPO, three-dimensional eye mount for procedures in ophthalmology.
Discussion
The efficacy of preclinical surgical exposure and simulation for ophthalmology trainees has been widely investigated,3 and of this, wet lab training plays a central role. Although there are increasingly more options for computerised simulations to teach surgical techniques for cataract and vitreoretinal procedures,4 instruction on cadaveric tissues remains a mainstay for teaching various corneal, strabismus and complex anterior segment procedures, as well as the tenets of globe rupture repair. Moreover, given the expense of virtual simulation and the wide availability of various cadaveric tissues (human or animal) by comparison, this modality often represents the sole form of preclinical surgical training in many low-resource settings.
Consequently, there is an obvious need for conditions in the surgical wet lab that closely mimic those in the OR, allowing trainees to cultivate good practices that will translate to clinical practice, speeding skill acquisition and minimising complication rate in the process. Chief among these is the device used to fixate the practice material. Stability, affordability and accurate simulation of facial contours are crucial elements of an effective eye mount in the ophthalmology wet lab, but there currently exists no widely distributed system that incorporates all three of these key characteristics.
Here, we designed and constructed a low-cost, high-fidelity eye mount for surgical training that is open source for wide distribution and usage. TEMPO provided capable of stable, reliable fixation of cadaveric eyes throughout surgical practice sessions—something that the authors have not experienced with other systems, which routinely require ongoing adjustment and refixation over the session. Its suction-based design enables easy achievement and modulation of physiologic/supraphysiologic IOP levels, as desired, by adjustment of the attached syringe. This avoids the pitfalls of non-suction methods, such as the pins/elastics commonly employed with foam mannequin (trial) heads, which frustrate the trainee with frequent loss of globe turgidity and attendant chamber collapse with surgical penetration of the eye. Further, the flat base and reassuring mass of TEMPO provide a solid platform to suture against, unlike the foam heads, which are light and have the tendency to roll, providing very little stability to the learning surgeon.
Integral to the optimal function of a surgical mount is the mimicry of the contours of a patient’s face. Practice without such leads to a tendency for trainees to be comfortable with actions under ‘ideal’ circumstances, but unprepared to perform the same motions over/around facial structures in the OR. This is a major limitation of the flat Mastel-Mandell eye mount. It provides good suction to keep cadaveric eyes in position for surgical manipulation, but lacks the facial contours required for trainees to learn how to effectively place their hands when learning to suture on a real patient, and certainly cannot emulate the various anatomical challenges such as a deep brow or a long nose that frequently confront ophthalmic surgeons. Despite its other drawbacks, the simple foam head has strength in this area, with anatomically correct facial contours. The low-cost Spring action Apparatus for Fixation of Eyeball device designed by Ramakrishnan et al2 is a similar suction design, but one for which the authors developed a ‘mask’ housing that can be superimposed on the mount to approximate facial contours. However, it is obvious from their photographs that this is a non-anatomical design, and there appears to be no solid mechanism of fixation between the shroud and the mount. Indeed, the authors comment that their preference is for handheld usage of the shroudless mount, attesting to these very limitations. TEMPO provides facial anatomy that is not only realistic and accurate, but also modifiable.
Although the Ramakrishnan et al’s design looks promising in many respects, it lacks in availability: it does not appear to be commercially produced, and there are no blueprints available off which one could reproduce their design. Consequently, we were unable to obtain a copy of their device for testing and comparison to TEMPO. Comparatively, our mount can be reproduced and customised by anyone with access to a computer and small 3D printer. Their steel ‘mask’, by contrast, looks to be a single-design piece, and making any alterations to its contours would require a ground-up redesign each time. It should also be added that different ethnicities and age groups have various head sizes and diverse facial contours, and these features can be easily incorporated into TEMPO by adjusting the digital 3D design. For instance, a particularly shallow or deep orbit (common surgical situations) is readily achieved.
Cleanliness and sanitation are a major consideration in the surgical wet lab, given that the cadaveric materials employed are inherently biohazardous in nature, and this is another department in which the existing mount options fall short. The Mastel-Mandell incorporates no means whereby to detach the suction system for effective disinfection/replacement, which can potentially lead to accumulation of cadaveric material within the tubing itself. The authors have experienced that foam heads quickly accumulate cadaveric residue, and have no mechanism for cleaning, effectively making them single-use-disposable. By contrast, TEMPO is conceived to be modular, readily cleaned (as an all-polymer design), and extensively reusable—parts can even be printed as subunits if one were to break/require replacement. Also, unlike the other suction mounts, ours is readily adapted to accommodate non-cadaveric eyes, which increases flexibility and eliminates the issue of biohazard waste altogether. A summary of the characteristics of TEMPO compared with existing mount systems is presented in table 1.
Comparison of TEMPO to other eye mounts
Although we feel the TEMPO mount largely addresses the shortcomings of present mount systems, this project still presented unique technical challenges. 3D printing is becoming increasingly ubiquitous, but it should not be overlooked that our design relies on the availability of such facilities and the attendant technical expertise, which may limit its utility in extremely resource-constrained settings. Prototyping TEMPO involved numerous design revisions and multiple prints to refine; although the mount, as provided, is turnkey ready-to-print, we realistically expect that centres looking to customise our design will have to undergo a similar process.
There are also other limits that we intend to improve over subsequent phases. As the eye is attached to a fixed base with vacuum created by the syringe, it cannot replicate the passive extraocular movements experienced during surgery. We plan to update the design with a ball and socket mount that can simulate this movement in future iterations and release this update online. Although we selected PLA based on its availability as one of the most common 3-D printing filaments as well as its biodegradable nature, it is somewhat porous, limiting the duration for which a suitable vacuum can be maintained. In addition, theoretically minute amounts of biowaste could potentially still permeate the pores of the PLA material, though our mount shows no signs of discolouration or contamination after multiple uses. We plan to continue work on improving and testing different fixation designs, such as a compressive belt surrounding the eye as well as different filament materials in the future, releasing each of these online to allow for ongoing refinement of the design.
As part of this publication, we are releasing TEMPO as a free and open-source file (https://www.ophthalmologyexplorer.com/innovations/project-one-7f9kx). The accessible nature of the file allows anyone in the world to download and 3D print the product for testing. They can also alter the downloaded computer-aided design file to fit their needs or make adjustments to existing components. As 3D printing becomes more ubiquitous, we hope wet lab training equipment can be customised to fit resource-limited training settings. Therefore, not only will TEMPO refine some of the challenges of previous eye mounts, but also maximise affordability of resources for learning.
Conclusion
The functional 3D-printed eye mount for procedures in ophthalmology (TEMPO) allows for proper stability of cadaveric and some non-cadaveric simulation eyes for surgical training. It has the added benefit of anatomically-correct facial contours to facilitate appropriate hand postures and ergonomics for ophthalmology trainees. We hope that its affordability and open-source format can benefit trainees around the world, especially in resource-limited environments.
Data availability statement
No data are available. Not applicable
Ethics statements
Patient consent for publication
Ethics approval
Research ethics approved the use of the cadaveric eyes for research and training purposes in conjunction with our local eye bank in Calgary, Alberta.
Footnotes
Presented at Canadian Ophthalmologic Society Annual Meeting 2020 (Virtual meeting).
Contributors MM conceived the idea and concept, devised the initial model drafts and along with YH, developed the concept further with testing. RT is the owner of Affordable 3D and was paid in part for assistance in refining the concept, 3D modelling and 3D printing of this project. WMT contributed to the manuscript and review process. HC and KJW were instrumental in providing feedback to model testing and supervision. All authors provided critical feedback and helped shape the research, analysis and manuscript. MM is the guarantor of this study, and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.