Article Text

Abstract
Background/aim To determine willingness to pay for children’s spectacles, and barriers to purchasing children’s spectacles in Cambodia.
Methods We conducted vision screenings, and eye examinations as indicated, for all consenting children at 21 randomly selected secondary schools. We invited parents/guardians of children found to have refractive problems to complete a willingness to pay for spectacles survey, using a binary-with-follow-up technique.
Results We conducted vision screenings on 12 128 secondary schoolchildren, and willingness to pay for spectacles surveys with 491 parents/guardians (n=491) from Kandal and Phnom Penh provinces in Cambodia. We found 519 children with refractive error, 7 who had pre-existing spectacles and 14 recommended spectacles for lower ametropias. About half (53.2%; 95% CI 44.0% to 62.1%) of parents/guardians were willing to pay KHR70 000 (US$17.5; average market price) or more for spectacles. Mean willingness-to-pay price was KHR74 595 (US$18.6; 95% CI KHR64 505 to 86 262; 95% CI US$16.1 to US$21.6) in Phnom Penh and KHR55 651 (US$13.9; 95% CI KHR48 021 to 64 494; 95% CI US$12.0 to US$16.1) in Kandal province. Logistic regression suggested parents/guardians with college education (OR 6.8; p<0.001), higher household incomes (OR 8.0; p=0.006) and those wearing spectacles (OR 2.2; p=0.01) were more likely to be willing to pay ≥US$17.5. The most common reasons for being unwilling to pay US$17.5 were related to cost (58.8%). The most common barrier to spectacle wear was fear that spectacles weaken children’s eyes (36.0%).
Conclusions With almost half of parents/guardians unwilling to pay for spectacles at the current average market price, financial support through a subsidised spectacle scheme might be required for children to access spectacles in Cambodia.
- child health (paediatrics)
- optics and refraction
- epidemiology
- public health
- vision
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Uncorrected refractive errors in childhood can result in decades of life spent with vision impairment.
School eye health programs in Cambodia provide vision screening services, but rely on external funding to provide free spectacles or leave parents to access spectacles at market prices.
What are the new findings?
Many parents and guardians in Cambodia are unwilling to pay market prices for children’s spectacles.
How might these results change the focus of research or clinical practice?
Removing or reducing financial barriers may increase access to spectacles for children with uncorrected refractive errors.
Introduction
Vision impairment and blindness in childhood can result in decades of life spent impaired, and a lifetime of financial burden on families and communities.1 Refractive errors increase as children progress through school, and on average globally, over 30% of children in late adolescence are estimated to have refractive error.2
Cambodia, with a population of 16.7 million, has experienced one of the highest recent rates of urban expansion in East Asia.3 With increasing urbanisation, the prevalence of refractive errors is likely to rise.2 A study in 2010 estimated the prevalence of refractive error in urban and rural schoolchildren from two provinces in Cambodia to be 13.7% and 2.5%, respectively.4 The same study demonstrated that access to children’s spectacles in Cambodia was limited, as over two-thirds of children with refractive errors (68.6%) from urban areas did not have spectacles, and no children with refractive error from rural schools had spectacles. In 2007, Rutzen et al reported that almost no eye care services were accessible for those living in rural areas in Cambodia.5
The Cambodian Ministry of Education, Youth and Sport (MoEYS) and Ministry of Health worked with non-governmental development partners and other Cambodian government departments to revise the School Health Policy. The new policy was passed into Cambodian law as the National Policy on School Health in 2019, and now includes a school eye health programme.6 The programme provides vision screening services and promotion of eye health education through the education system for primary and secondary school students.
The availability of affordable spectacles is essential to the success of a school eye health programme. Currently, school eye health programmes in Cambodia rely on external funding to provide free spectacles or leave parents to access spectacles at market prices. The average price of functional (ie, not catering to fashion) custom-made spectacles ranges from US$17.50 (clear single-vision stock powers) to US$40.00 (high spherical/astigmatic powers) at optical vision centres.7 Studies in countries at comparable levels of development suggest only 20%–50% of children have the spectacles that they need,8–11 and that access to spectacles is predominantly impacted by economic constraints, or a lack of services.12
It is currently unknown whether parents/guardians can afford spectacles for children. Identifying the amount various parents/guardians are willing and able to pay for spectacles for children may allow school health programmes to remove, reduce or better target spectacle subsidisation. Adjusting the amount or pattern of subsidisation may reduce eye care programme costs and/or improve coverage. The aim of this study was to determine willingness of parents/guardians to pay for children’s spectacles, and barriers to purchasing children’s spectacles in Cambodia.
Methods
We used a prospective, cross-sectional study design conducted in Phnom Penh and Kandal provinces of Cambodia. The two provinces were purposefully selected to represent urban and rural areas. School selection was restricted to secondary schools as older children are expected to have a higher prevalence of refractive error.4 The schools invited to participate in the screening programme were randomly selected from a list obtained from MoEYS, which covered all districts of the two provinces. Eligible participants were the parents/guardians of schoolchildren with refractive error, who were identified through the secondary school vision screening programme. All secondary students from selected schools were invited to be screened and no students were excluded on the basis of age, despite some students being over the age of 18.
Sample size calculation
We determined that the parents/guardians of 560 children with refractive errors would be required to detect a proportion of 12.5% of adults willing/willingness to pay (WTP) KHR70 000 (US$17.50, which is the average market price of single-vision prescription spectacles) with a 30% relative precision, 80% response rate, 1.5 design effect, alpha value of 0.05 and power of 80%. With the prevalence of refractive errors in children reported to be 13.7% in urban areas and 2.5% in rural communities,4 we determined that we needed to screen 11 500 schoolchildren, with 7500 from rural areas and 4000 from urban areas in order to proportionally represent children living in both urban and rural communities. As refractive error rates were lower than expected in Kandal province, the sample size was increased until sufficient parents/guardians were recruited to meet the target.
School vision screening
A team of refractionists and vision screeners was recruited locally and trained to conduct vision screenings and categorise children. The detailed vision screening flow chart can be found in online supplemental figure 1. In children identified as vision impaired by the screening protocol, refractive error was determined, and other causes identified. All children identified as requiring further eye care were referred to the nearest appropriate eye health service. Children who needed spectacles were provided with spectacles at no charge after completion of the study to minimise participant response bias.
Supplemental material
Refractions were performed without cyclopleiga. Children who were identified as needing cycloplegic refraction were referred to the nearest eye hospital. Refractive error states were defined as myopia ≤−0.50 DS, hyperopia ≥+2.00 DS or astigmatism ≤−0.75 DC in either eye. Primary refractive diagnosis was based on spherical equivalent—that is, children with astigmatism were preferentially classified either myopic or hyperopic when their spherical equivalent refraction qualified. Children with astigmatism and emmetropic spherical equivalent refractions were classified as having mixed astigmatism. We included secondary refractive diagnoses—high refractive error (≥5 D of any kind in either eye), anisometropia (≥1 D difference of any kind between right and left eye) and all astigmatism (≥0.75 DC regardless of spherical equivalent)—as an indication of more complex refractive care needs.
Participant surveys
Parents/guardians of children with refractive error were invited to participate in an interview-based survey (the study participation flow chart can be found in online supplemental figure 2). The survey explored parents’/guardians’ WTP for children’s custom-made spectacles, views on barriers to and preferences in purchasing children’s spectacles, beliefs surrounding access to eye care affordability, perceptions of their child’s vision status and attitudes towards spectacles. WTP is the maximum amount an individual is willing to spend for a proposed service or good.13 There are many methods for eliciting WTP in contingent value using different question formats.13 The binary-with-follow-up method was used to determine parents’/guardians’ WTP for children’s spectacles. Beginning at KHR20 000 (US$5), respondents were asked a series of ‘yes/no’ questions regarding their WTP that amount for their child’s spectacles. Depending on the response, the amount increased or decreased incrementally until the maximum amount was reached. As a follow-up to ascertain amounts that might be above the identified maximum increment but below the next increment, respondents were also asked to state the maximum theoretical amount they were WTP. The published studies describing WTP for eye care services and products have used a variety of methods including open-ended questions, closed-ended binary (dichotomous) questions, triple-bounded dichotomous choice, binary-with-follow-up and payment card format. Binary-with-follow-up is effectively a truncated bidding game,14 which aligns with social norms in Cambodia where bargaining for goods is common. Additionally, binary-with-follow-up method is thought to elicit a more accurate WTP compared with open-ended questions, which reduce the range in which the respondents’ true WTPs lies.14 A previous study also reported binary-with-follow-up to be the most appropriate WTP method for the Cambodian population.15 The WTP survey was developed by the research team in conjunction with relevant local stakeholders and volunteer parents in Phnom Penh.
Supplemental material
Statistical analysis
Study data were collected and managed using REDCap electronic data capture tools hosted at the Brien Holden Vision Institute.16 17 Statistical analyses were performed using SPSS V.21.0 and Stata V.10.
We determined the frequency distributions and prevalence estimates of refractive error for demographic variables and the overall sample. The variance and the 95% CI were estimated based on multistage cluster design sample where individual schools were defined as the primary sampling unit. Taylor linearisation was used for variance estimation. The mean WTP was compared between respondent characteristics using general linear models. WTP was log transformed prior to analysis due to the skewed distribution of the data. WTP was also categorised based on WTP ≥KHR70 000 (US$17.5) and compared between respondent characteristics using Pearson χ2 tests. Multivariable logistic regression was used to identify factors associated with being unwilling to pay KHR70 000. Factors that were significant in the univariate analysis were included in the multivariate model using backward elimination and forward entry methods until only significant factors remained in the model. The level of statistical significance was set at 5%.
Patient and public involvement
Patients and members of the public were not involved in setting the research question or study design but a group of volunteer parents helped to develop the survey.
Results
A total of 12 128 children (mean age 15.1±1.8 years; range: 11–20, female 56.1%), were screened from 21 schools, 5 in Phnom Penh and 16 in Kandal province (table 1). More girls than boys were screened in both locations (gender ratio 1.1 in Phnom Penh and 1.3 in Kandal) which is higher than the net school attendance ratio (gender ratio 1.0 in Phnom Penh and 1.05 in Kandal).18
Refractive error among children
The majority of children (95.7%, n=11 602) presented with normal vision in both eyes without correction, while seven children (0.06%) presented with normal vision with pre-existing spectacles. Refractive error (4.3%; n=519) was the main cause of reduced presenting vision (table 1), with myopia accounting for 4.1% and hyperopia 0.12%. Amblyopia was identified in 36 children (0.3%) and an additional 45 children (0.4%) had reduced best corrected vision due to other causes. Refractive error (10.3% vs 1.7%, p<0.001) and amblyopia (0.5 vs 0.2, p=0.02) were significantly higher in Phnom Penh compared with Kandal province. Myopia was observed to be higher among females compared with males (4.9% vs 3.5%, p=0.005) and among children aged 15–20 years compared with younger children (4.8% vs 3.5%, p=0.094).
Within the newly diagnosed refractive error group, 211 were considered to have refractive needs more complex than those correctable with simple, on-the-spot spectacle options. Some individuals had multiple complexities, but within the 211, 38 had high refractive error, 101 had astigmatism (myopic, hyperopic or mixed), and 146 had anisometropia.
In addition to 519 cases of newly diagnosed refractive error and 7 who had pre-existing spectacles, there were 10 children who had spectacles recommended for hyperopia less than the threshold for diagnosis, and 4 who had spectacles recommended for anisometropia less than the threshold for diagnosis.
WTP survey participants
A total of 540 parents were invited to participate in an interview to discuss their WTP for children’s spectacles (519 new refractive cases, 7 with pre-existing spectacles and 14 recommended spectacles for lower ametropias). There were 49 parents (9% refusal rate) who did not consent to participate in the interview. Of these parents, 33 of the children were females (67%) and 16 males (33%).
Of the 491 parents who consented and participated (91% response rate), 74.1% were in Phnom Penh as the prevalence of refractive error was higher compared with Kandal province (table 1). Most respondents were female (60.5%), aged between 41 and 50 years (42.4%) and identified as the head of their household (85.3%). Secondary school (35.6%) was the most common education level achieved by respondents. Self-employment (56.4%) was the most common occupation of the principle income earner. Over 45% of households earned a monthly income of over KHR1 200 000 (US$296). In 2016, the median household income in Cambodia was KHR 1 186 000 (KHR 2 210 000 in Phnom Penh, and KHR 1 021 000 in other rural areas).19 The majority of respondents (86.2%) reported that they had not had an eye test before. Eighty-nine per cent did not report issues with distance vision, 71.5% did not report trouble with near vision and 88.2% did not currently wear spectacles.
WTP for spectacles
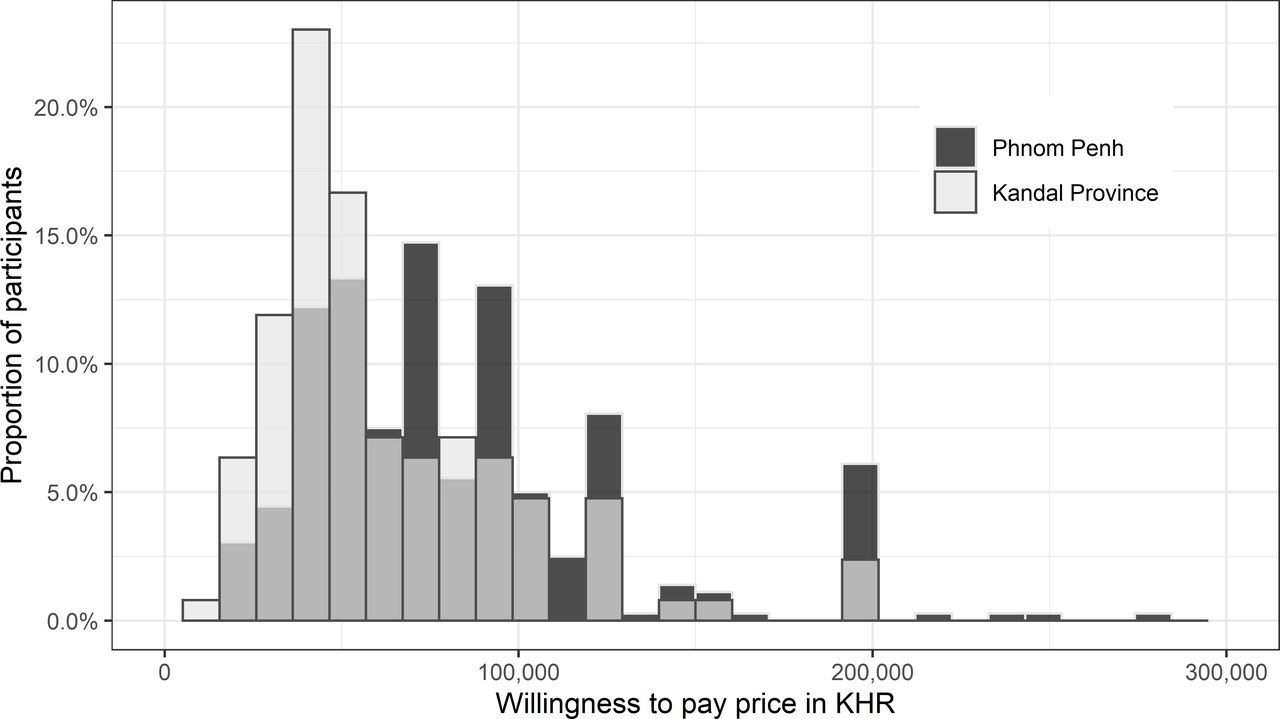
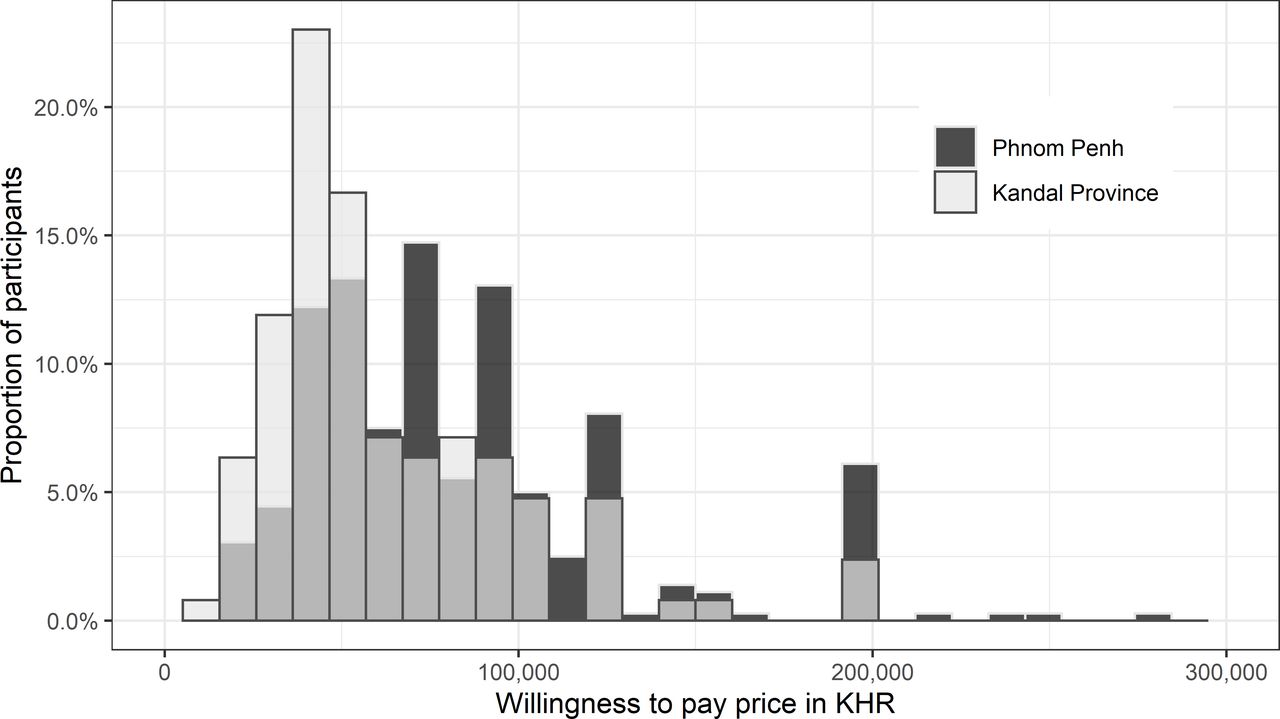
As figure 1 illustrates, we found that 99.8% of participants were WTP the minimum twice daily price of KHR20 000 (US$5) for spectacles and 80% were WTP KHR45 000 (US$11.30). The proportion of parents WTP the average market price of KHR70 000 (US$17.5) was 53.2%. The proportion dropped to 40.9% for KHR80 000 (US$20) and to 23.8% for KHR100 000 (US$25) or more. 59.6% (95% CI 52.1 to 66.7) participants from Phnom Penh reported WTP equal or more than KHR70 000 (US$17.5) compared with 34.6% (95% CI 21.4 to 50.8) participants from Kandal province (table 2). Only 41.7% of participants from Kandal province were WTP KHR45 000 (US$11.30) or less (figure 2). Mean WTP price of participants was KHR74 595 (US$18.6) (95% CI KHR64 505 to KHR86 262; 95% CI US$16.1 to US$21.6)) in Phnom Penh and KHR55 651 (US$13.9) (95% CI KHR48 021 to KHR64 494; 95% CI US$12.0 to US$16.1)) in Kandal province (table 2).
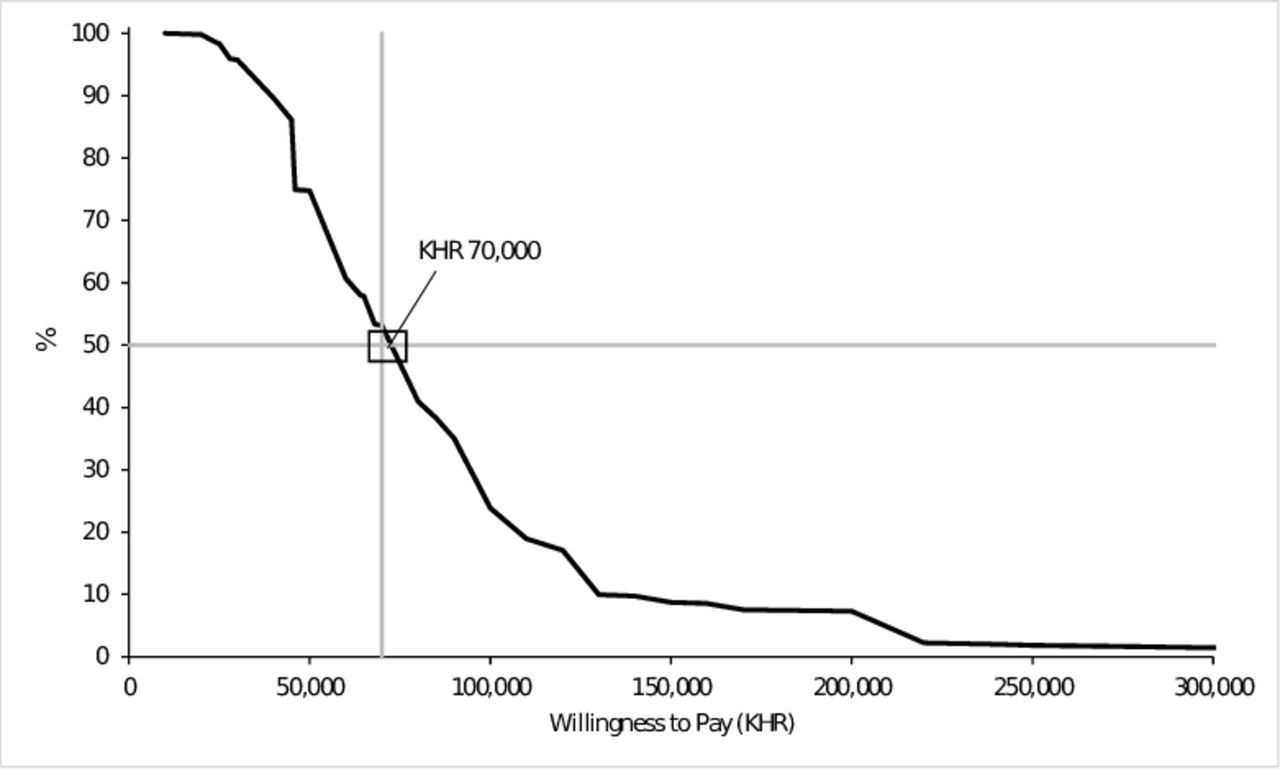
Cumulative percentage of parent’s/guardian’s willingness to pay for children's spectacles, according to the maximum values reported.
{kind=link}
{kind=link}
Distribution of willingness to pay by province.
Demographic details of participating parents/guardians and willingness to pay for custom-made spectacles
The univariate analysis showed parents who reported they were WTP higher amounts for spectacles (calculated mean price) were more likely to be male, from Phnom Penh, younger in age, more highly educated and from a higher income bracket (table 2). Similarly, analysis of participant’s WTP the average price of KHR70 000 (US$17.5) found male (p=0.002), those from Phnom Penh (p=0.008), those with higher education (p<0.001), higher monthly incomes (p<0.001), current spectacle wearers (p=0.02) and those who had noticed their child had a vision problem (p=0.03) were significantly more likely to be WTP US$17.5 or more (table 2). Participants who reported a WTP less than US$17.5 were more likely to believe that children should not have spectacles before the age of 18 (p=0.03), more likely to report they did not have time to take their child for an eye examination (p=0.02), to report that the eye clinic was too far away (p<0.001), and disagreed that parents should encourage children to wear recommended spectacles (p=0.01).
Table 3 shows that in a logistic regression model, parents/guardians with college level education (OR 6.8; p<0.001), higher monthly household incomes (OR 8.5; p=0.006), those currently wearing spectacles (OR 2.2; p=0.01), positive attitudes towards child wearing spectacles (OR 2.4; p=0.04), and those who think free spectacles are poor quality (OR 4.0; p=0.03) were significantly more likely to be WTP US$17.5 (average market price) or more for children’s spectacles.
Factors associated with willingness to pay ≥US$17.5 for children’s spectacles
Reasons for WTP decisions, and attitudes and barriers to spectacle wear
Parents were asked to provide reasons for why they would not be WTP more than the maximum WTP amount they reported for their children’s spectacles. Of the 230 participants unwilling to pay US$17.5 or more, 77% reported reasons related to cost (see online supplemental figure 3). Among those who were WTP US$17.5 or more, 30% reported reasons related to cost, 40% reported ‘other’ and 23.5% reported ‘don’t know’.
Supplemental material
Of 491 participants, the majority of respondents (86.6%) were willing to purchase spectacles from an optical shop and 18.9% were willing to purchase from the eye unit/hospital. Respondents believed transport to eye care facilities to be affordable (83.9%), however, many respondents considered eye examination fees to be unaffordable (28.9%) or were unsure of the cost of an eye examination (27.1%).
The most commonly cited attitudinal barrier to spectacle wear was related to fears that spectacles weaken children’s eyes (see online supplemental figure 4).
Supplemental material
Reasons why a child has not had an eye examination and not wearing spectacles
A total of 275 of 491 (56.0%) children had not had an eye examination prior to the school screening. The common reasons reported by parents/guardians for their child not having had an eye examination were that they did not notice vision problems (51.7%), they had no time to take their child for an eye exam (15.7%), and the distance to an eye clinic (3.3%).
According to parents/guardians, 202 (41.1%) reported their children had spectacles. The common reasons for a child not wearing spectacles that had been purchased were that they were uncomfortable to wear (6.3%), the child does not like wearing spectacles (4.3%), spectacles will harm or worsen vision (1.6%) and friends tease when spectacles are worn (1.2%).
Interestingly, while 95.5% of respondents would be happy to purchase spectacles for their child, there is also positivity towards free spectacles—96.7% reporting they would feel good if their child received free spectacles and 94.1% disagreeing that free spectacles were of poor quality.
Discussion
Willingness to pay for health services and health insurance in low-income and middle-income countries has been widely reported.20–24 However, there are only a handful of studies reporting WTP for eye care services such as cataract surgery,25–27 glaucoma services,28 29 specialty emergency eye services,30 trachoma treatment31 and spectacles.15 32–36 All published studies have focused on WTP for eye care services and products in adult populations. Our study is novel in that it reports parent/guardian WTP for children’s spectacles.
Our study results showed that 53.2% of parents/guardians were WTP KHR70 000 (US$17.5) or more. A study conducted in 2004 in Kampong Cham province in Cambodia reported that 76.6% adult patients were WTP KHR1500 (US$0.40), which at that time was the lowest price possible for ready-made spectacles.15 The apparent change over time could be entirely explained by the dramatic economic growth and broader developments that have taken place in Cambodia. Other explanations such as greater willingness to spend on children’s eye care than personal care may be contributing but are impossible to prove by comparing our study with the older one.
The refractive error rate we determined (4.3%; 95% CI 2.5% to 7.1%) was lower than that reported by a 2010 study (6.57%; 95% CI 5.91% to 7.22%) conducted in the same provinces,4 although the overlapping confidence intervals indicate that the difference is not significant. This low rate suggests that a future study is needed to explore the schoolchildren behaviours to see if there are any preventative factors. Further, restricting our results to the age range of the 2010 study (11–14 years old) means the difference became greater—3.5% (95% CI; 1.7% to 6.9%) had refractive error in our study versus 6.57% (95% CI 5.91% to 7.22%) in the 2010 study. The difference could be attributed to chance effects, a decrease in refractive error over time (against expected trends), subtle protocol differences or the differences in sampling method. In the current study, our primary sampling cluster was 21 secondary schools in which all schoolchildren were screened, while the Gao et al study randomly selected classes from 36 schools.4
Our WTP results are broadly consistent with previous studies,15 32 35 37 showing effects of education, income, gender, urbanisation, employment type and personal ocular/refractive history. However, there are potential biases and confounders in these results. For example, culturally specific and gendered interpretations of what defines a head of household (age, primary caregiving, decision making, allocation of resources, etc) might affect classifications and decision making.
Barriers to purchasing spectacles in our current study—mainly around cost—were also consistent with other studies from developing countries.12 36 38 Our finding that most (95%) parents/guardians would purchase spectacles for their child but that most (97%) would also feel good if their child received free spectacles, potentially stems from a history of external agencies funding children’s spectacles in Cambodia. External agencies will need to provide clear and coherent messaging about any subsidisation in order to move towards locally sustainable, independent refractive care.
Parents’ positive attitudes to spectacle wear is essential for making spectacle purchase decisions.12 In the present study, parents fear that spectacles weaken children’s eyes, and beliefs that ‘wearing spectacles is a health problem’ and ‘spectacles are not needed for a little myopia’ are common attitudinal barriers to spectacles use, and this finding tallies with findings in low-income and middle-income countries.12 39 Eye and healthcare systems have an expectation that parents/guardians will detect their children’s eye problem and take them to an appropriate professional for an eye examination. The present study found that over half of the parents did not notice vision problems and about one-fifth did not get time to take children for eye examinations. These reasons were similar to those reported by parents and students in China.39 A study in Vietnam demonstrated that eye health education and promotion activities in schools and communities were beneficial to overcoming negative beliefs and fears about spectacle wear and increasing awareness of the need for eye examinations at school age.40
Limitations
Past studies have shown that the stated WTP would be different than a real payment for spectacles purchase.15 The hypothetical WTP amount is usually higher than the amount participants would really pay.41 Although respondents are likely to bid higher WTP when they have less experience with the services and products, a few studies have shown hypothetical/stated WTP being validated with the actual pay.34 42 Furthermore, when diagnosed with refractive errors, the respondents tend to report a higher WTP price for spectacles.35 Given that 13.6% respondents reported having had an eye examination and 11.8% currently wearing spectacles, the majority of parents had little experience in purchasing spectacles and thus may have reported different WTP price than that they would actually pay.
Our study sample size was based on the refractive error rates of secondary school children from the previous study in the Phnom Penh and Kandal provinces. However, the refractive error rates were lower than expected and thus the screening sample population in Kandal province was increased by approximately 700 children. This adjustment allowed us to detect 540 children with refractive error so that we could invite parents/guardians of these children for the WTP survey. The higher-than-expected response rate (91% vs 80%) resulted in a sample that was more than adequate for the main objective of this study.
Implications
40.9% of parents/guardians were WTP KHR80 000 (US$20.0) or more which is a price that could generate enough revenue to enable cross-subsidisation of spectacles for those unable to afford cost price. Implementing a tiered pricing structure based on customer self-selection of spectacle frame and capacity to pay could improve equity of access to simple frame spectacles and decrease dependence on external funding. However, pricing needs to be well within parents/guardians maximum WTP, as willingness does not necessarily equate to ‘ability’ to pay and parents/guardians willingness to purchase spectacles may result in financial hardship. With ‘cost’ identified as a significant barrier, the eye care needs of children in Cambodia should be an integral part of Universal Health Coverage to meet population needs and avoid financial hardship.
School vision screenings and provision of spectacles in schools are considered effective where public and private eye care services are difficult to access and/or afford.12 Preferably, school vision screenings should both identify children with vision problems and provide spectacles for those with significant uncorrected refractive error but unable to pay.
In conclusion, about half of participating parents/guardians were WTP US$17.5, an average price for custom-made single-vision spectacles with stock lenses. However, the other half were unwilling to pay this amount, suggesting equitable access to spectacles for children in Cambodia requires financial input for a significant portion of the community, either via cross-subsidisation, health insurance, or some other form of support. This WTP data enables government and other organisations to design an evidence based, equitable and affordable eye care system for Cambodian children. Additionally, barriers and negative attitudes continue to contribute to children living with avoidable vision impairment rather than accessing treatments. It will be interesting to see if the Cambodian government’s new National Policy on School Health6 is able to address these barriers and attitudes via eye health education and promotion programmes.
Acknowledgments
We thank the Cambodian Ministry of Health/National Program for Eye Health and the Ministry of Education, Youth and Sports for their assistance in completing this project. We also thank Seila Chea and Malis Dean for their data collection work, and the Cambodian Eye Care Subsectoral working group for their feedback.
References
Supplementary material
300 Multiple Choices This is a pdf-only article and there is no markup to show you.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AB and LL designed data collection tools, monitored data collection and drafted and revised the paper. PP cleaned and analysed the data and drafted and revised the paper. JM monitored data collection for the whole trial, cleaned and analysed the data and drafted and revised the paper. NK designed data collection tools, monitored data collection for the whole trial and drafted and revised the paper. EK designed data collection tools, monitored data collection for the whole trial and drafted and revised the paper. VT analysed the data and drafted and revised the paper. TRF analysed the data and revised the draft paper.
Funding This work was supported by the Lions Clubs International Foundation under a Sight First Grant (SFP2012/UND).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was conducted in accordance with the Declaration of Helsinki with written informed consent obtained from participants. Ethics approvals were obtained from the Cambodia National Ethics Committee for Health Research (087NECHR) and the University of New South Wales Human Research Ethics Committee (HC108151).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.