Article Text

Abstract
Several studies have compared binocular therapy and patching for the treatment of amblyopia. However, most of them involved a small number of cases and reported controversial results. Thus, the benefit of binocular therapy remains to be confirmed. We conducted a meta-analysis to evaluate the efficacy of binocular therapy versus patching and to testify whether binocular therapy could become supplementary method in children with amblyopia. Randomised controlled trials that evaluated the efficacy of binocular therapy for amblyopia versus patching were identified using PubMed, Embase, Cochrane Library, Ovid, Web of Science, ClinicalTrials.gov, and the WHO International Clinical Trials Registry Platform. Data screening, extraction and quality assessment were performed independently by two researchers. Six trials were identified and analysed to compare binocular therapy (708 eyes) with patching (664 eyes) for change in best-corrected visual acuity and stereoacuity. Efficacy estimates were evaluated by standard mean difference (SMD) and 95% CI. The best-corrected visual acuity in binocular group was better than that of in patching group (SMD=−0.21 logarithm of the minimum angle of resolution (log MAR), 95% CI of −0.50 to 0.08 log MAR, p=0.003). The results showed statistically significant difference in the change of best-corrected visual acuity between the groups, but not in stereoacuity. Binocular therapy may be a promising treatment of conditions affecting visual acuity, and could be applied as a supplementary method to patching for amblyopia in clinical practice. The present analysis showed that some children with amblyopia may benefit from binocular therapy. Nevertheless, larger randomised controlled clinical trials are required to confirm these findings.
- visual perception
- vision
- treatment medical
- public health
- low vision aid
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Amblyopia (‘lazy eye’) is a form of cortical visual impairment, defined clinically as a unilateral or bilateral decrease in visual acuity (VA) that cannot be attributed to structural abnormalities of the eye or visual pathway. The pediatric eye conditions in amblyopia refer to strabismic, refractive, anisometropic, visual deprivation and occlusion causes. Amblyopia is the main cause of preventable blindness in children, with a prevalence of 1%–5%, and remains one of the most common causes of persistent unilateral visual impairment in adulthood. Amblyopia is classified as mild (20/25–20/40), moderate (20/50–20/100) and severe (<20/100).1 Children with amblyopia may have low self-esteem, negative self-image and feelings of depression, frustration and embarrassment.2 Therefore, it is vital to promptly administer treatment for children with amblyopia.
The standard treatments for amblyopia include optical method, occlusion and pharmacological blurring treatment.3 Although patching of the dominant eye is currently the most effective therapy of amblyopia, it has some limitations, particularly among children with low compliance.4 Impaired eye–hand coordination skills and abnormal binocularity were improved under binocular treatment in children with amblyopia.5 Binocular therapy is attracting considerable interest for the prevention of amblyopia recurrence and improvement of VA. The method which involves playing computer games or watching movies on digital displays is appealing to children, thereby improving adherence to this treatment.3 Binocular therapy presents with three systems, including ‘antisuppression therapy’, ‘balanced binocular viewing’ and ‘interactive binocular treatment (I-BiT) system’. This approach allows children to overcome interocular suppression, reduces the extent and depth of suppression and improves stereoacuity.6 Moreover, experiencing binocular vision while playing a game may yield better vision outcomes, VA and binocular function.7–9 The use of a binocular iPad game improves VA sooner by several weeks,10 which demonstrates that home-based binocular iPad games may be an effective treatment for amblyopia.11 However, it remains uncertain whether the benefit of binocular therapy is restricted to improving VA.
To date, few studies have investigated the association between binocular therapy and patching for amblyopia in children. Therefore, we conducted a meta-analysis of randomised controlled trials (RCTs) to systematically evaluate the efficacy of binocular therapy versus patching in terms of change in best-corrected visual acuity (BCVA) and stereoacuity. The objective was to determine whether binocular therapy could become supplementary therapy to patching in amblyopia for the improvement of VA.
Methods
This was a meta-analysis of existing RCTs; thus, approval by the institutional review board was not required. A study protocol was registered with PROSPERO (CRD42020188628). This meta-analysis adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.12
Data sources and search strategy
The PubMed, Ovid, Ovid Embase, Cochrane Library and Web of Science databases were systematically searched for articles published in English from their inception to 22 May 2020. The following search strategy was used: (exp amblyopia/ or amblyop$.tw. or exp strabismus/ or strabism$.tw. or squint$.tw. or exp refractive error/ or (refractive adj2 error$).tw. or exp anisometropia/ or anisometropi$.tw. or lazy eye$.tw.)and (occlu$.tw. or patch$.tw. or shield$.tw.) and (exp vision, binocular/ or binocular fusion.tw. or binocular perception.tw. or binocular view.tw. or binocular visual field.tw. or perception, binocular.tw. or vision, binocular.tw.) and(randomized controlled trial.pt. or (randomized or randomised).ab,ti. or placebo.ab,ti. or dt.fs. or randomly.ab,ti. or trial.ab,ti. or groups.ab,ti.)not(exp animals/ not (exp animals/ and exp humans/)). (“$” indicates truncation; “/” means MeSH heading)
The Cochrane Library, ClinicalTrials.gov (www.clinicaltrials.gov), and the WHO International Clinical Trials Registry Platform were screened for relevant electronic studies of RCTs related to amblyopia. The electronic database search was supplemented by a manual search of the reference lists of included articles.
Prospero registration number
CRD42020188628.
Inclusion and exclusion criteria
Articles were selected independently by two investigators and disagreements were resolved through discussion. The inclusion criteria were: RCTs that enrolled participants of age 3–17 years; diagnosis of strabismic, anisometropic and combined amblyopia; BCVA worse than 20/50 for ages 3–4, 20/40 for ages 4–5, 20/30 for ages 5 or more; no previous amblyopia therapy (eg, patching, atropine, Bangerter and vision therapy) in the past 2 weeks; absence of ocular pathology; no prior surgery; absence of systemic disease; and absence of Down syndrome or cerebral palsy. Studies with primary data, involving at least 2 weeks of binocular therapy with patching or not in one group, patching with placebo binocular iPad game or patching in the other one, were included. Binocular therapy including iPad game, dichoptic movie and I-BiT. The outcome measure of the study was BCVA, and there was no restriction for the duration of the follow-up. Studies in which amblyopia was due to deprivation (eg, congenital ptosis or cataract) and not meeting the aforementioned study design criteria were excluded.
Data extraction and management
Researchers independently screened articles and extracted the data that were abstracted using a standardised collection form. The data included the first author, year of the study, mean age, study design, type of amblyopia, sample size, intervention method, mean duration of treatment, percentage of study discontinuation, adherence data, change in BCVA and improvement in stereoacuity.
Methodological quality assessment
The risk of bias for each included article was evaluated independently by the authors according to the methods established in the Cochrane Risk of Bias Tool for RCTs13: random sequence generation, allocation concealment, blinding of the participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting and other biases.
Statistical analysis
Data needed to determine the effect size were extracted independently by two researchers. Summary estimates, including 95% CIs, mean and SD (mean±SD), p value, and Z-value, were calculated. For continuous outcomes data (eg, BCVA), the means and SD were used to calculate the standard mean difference (SMD) between groups, where p<0.05 was regarded as statistically significant. For analysis, statistical heterogeneity was tested using the χ2 test and I² statistic.14 According to the Cochrane review guidelines, in the presence of severe heterogeneity (I²>50%), the random effect models were selected; otherwise, the fixed effect models were used. Subsequently, we considered performing sensitivity and subgroup analyses by follow-up duration or age to investigate the source of the severe heterogeneity when applicable (I²>50%). Moreover, considering that visual inspection of the funnel plot has several limitations, both Begg’s and Egger’s linear regression tests were performed to assess publication bias. Following the detection of publication bias, we used the trim and fill method to determine the stability of the results.
Results
Study characteristics
Literature search was performed using the search strategy indicated in figure 1. A total of 507 articles were identified. The full text of the remaining 44 articles was examined in further detail. Finally, 6 RCTs were included in this meta-analysis with 1272 eyes;15–20 304 participants underwent binocular therapy and 332 were treated with patching. The characteristics of the included studies are described in table 1. The compliance rates of studies15 17 were objectively recorded from the iPad device, indicating that numbers of participants who completed >75% of the prescribed treatment. Besides, subjectively rates using the log calendars were also provided. Improvement in BCVA is standardised as an increase of 0.025 logarithm of the minimum angle of resolution (log MAR) units (which equates to one letter), ensuring the facticity of the results between two groups.21 The methodology assessment presented a relatively high method quality.13
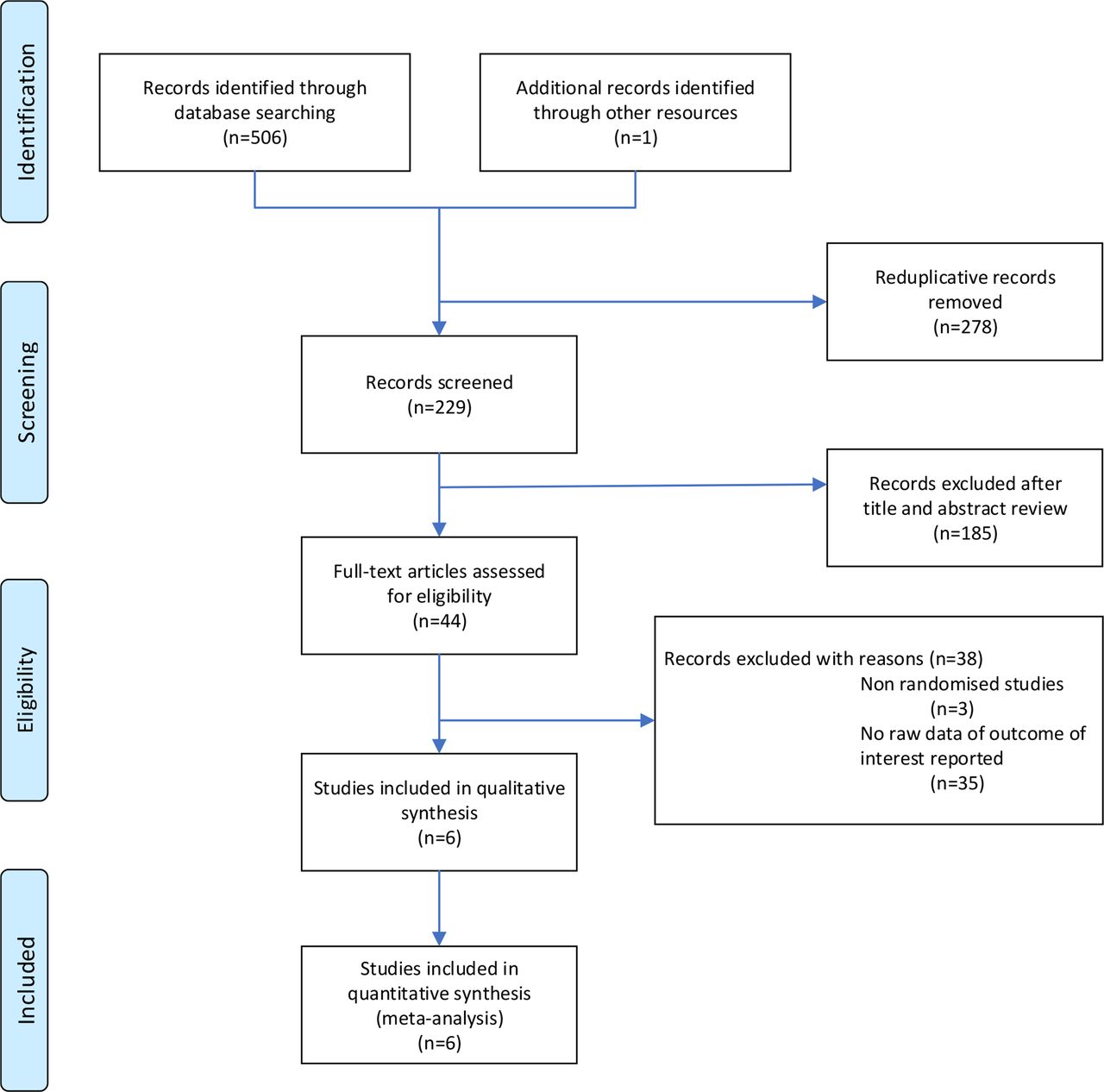
Flow chart of the search strategy used in the selection of articles.
Characteristics of included trials
We found that the estimated true effect size was 0.17 log MAR (95% CI 0.02 to 0.32 log MAR) in pretreatment BCVA, and there was no statistical difference between the two groups (Z=1.42, p=0.16).
We compared the overall effectiveness of binocular therapy for amblyopia, as well as the change in BCVA and stereoacuity in the six selected trials.15–20
Best-corrected visual acuity
The extent of heterogeneity in trials was I²=56.8% (p=0.04), indicating severe heterogeneity (figure 2A). The effect size and p values refer to BCVA improvement, that is, the difference between pretreatment and post treatment. The means are 0.13±0.14 log MAR in binocular group, 0.16±0.14 log MAR in patching group. The improvement in BCVA was significant (SMD=−0.21 log MAR, 95% CI of −0.50 to 0.08 log MAR). These findings indicated that binocular therapy for amblyopia was effective. In addition, binocular treatment improvement was lower than patching in BCVA. The test result for the combined effect was Z=3.01 (p=0.003), showing a statistically significant difference between the two groups (figure 2A). As illustrated in figure 2A, the diamond located on the left side of the vertical line indicates statistically significant differences between the two groups. It demonstrated that the patching group may be better significantly.

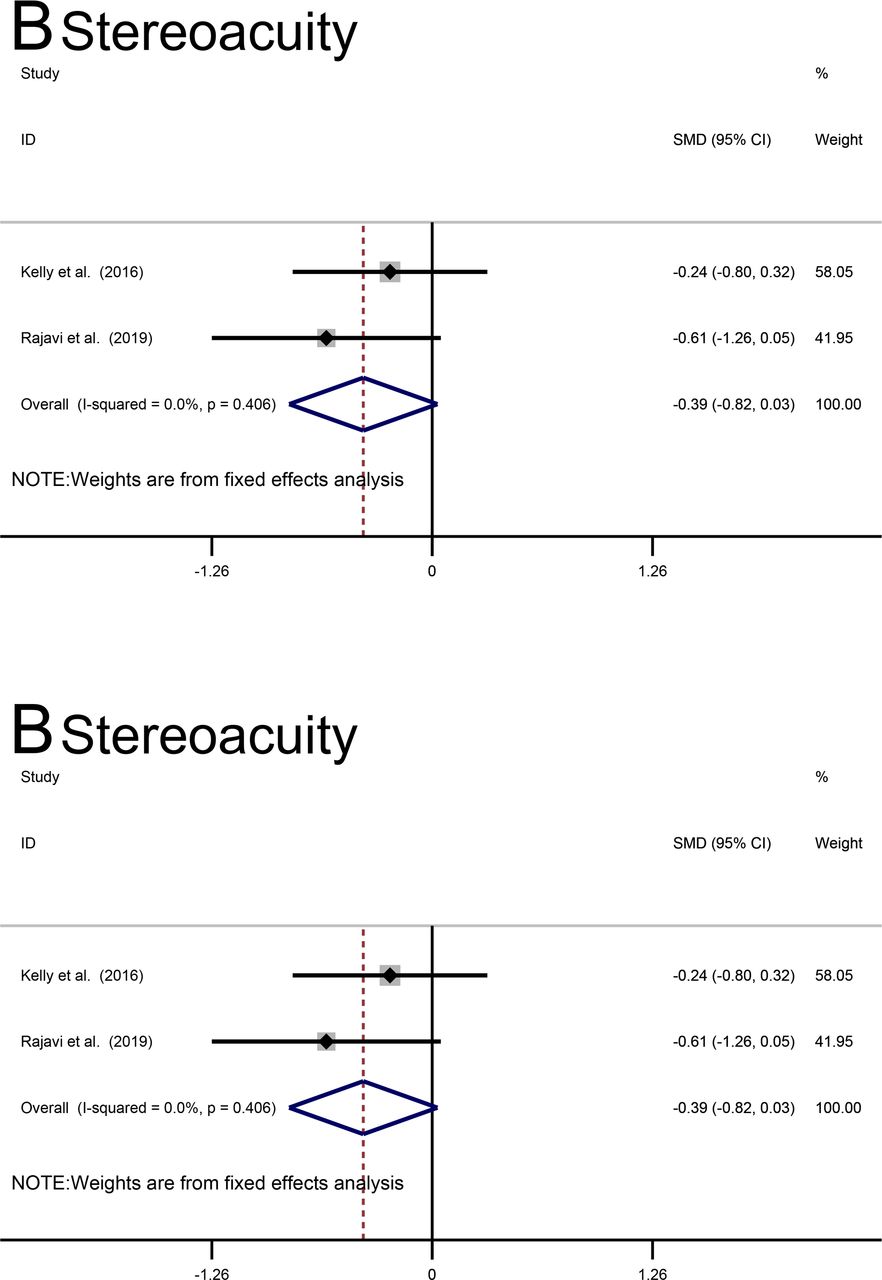
Forest plot of the effect of binocular therapy and patching on the change in best-corrected visual acuity (BCVA) and improvement in stereoacuity. (A) Forest plot of the effect of binocular therapy and patching on the change in BCVA. (B) Forest plot of the effect of binocular therapy and patching on improvement in stereoacuity. The dotted red line refers to the dashed line located on the left of the black vertical line (0). The left side of the black vertical line (0) refers to binocular therapy. The right side is patching treatment. SMD, standard mean difference.
Stereoacuity
The secondary outcome measure was stereoacuity using the Randot Butterfly and Randot Titmus Stereoacuity Test (Stereo Optical Co, Chicago, Illinois, USA). Only a few trials reported complete raw data, including baseline and post-treatment data. We used the obtained data to calculate the overall effects. The extent of heterogeneity in trials was I²=0.0% (p=0.41), indicating absence of heterogeneity. The mean and 95% CI of improvement in stereoacuity from each of the studies are shown in a forest plot in figure 2B. We found that the estimated true effect size was −0.40 log (seconds of arc), 95% CI −0.82 to 0.03 log (seconds of arc). The test result for the combined effect was Z=1.82 (p=0.07), showing that there was no statistically significant difference between the two groups.
Sensitivity analysis
We conducted a sensitivity analysis to determine the source of heterogeneity. We found limited difference between these trials in BCVA, indicating that the results were relatively stable. A severe degree of heterogeneity was identified in change of BCVA (I²=56.8%, p=0.041). The results of the sensitivity analysis demonstrated that one study,16 in which the inappropriate randomisation was found, had influenced the data analysis.
Publication bias analysis
We assessed publication bias in studies comparing binocular therapy with patching using the funnel plot. As shown in figure 3, the funnel plot is generally symmetric. There was definitely absence of publication bias, as determined by both Begg’s test (p=0.71) (figure 3) and Egger’s test (p>0.60). This indicated that the publication bias had limited influence on the results. The diversity of binocular therapies in studies18 20 resulted in the poor weight on the funnel plot.

{kind=link}
{kind=link}
{kind=link}
Funnel plot to assess publication bias. SMD, standard mean difference.
Discussion
Main results
Binocular therapy has recently been used as a promising option for the treatment of amblyopia. Several studies have reported that binocular gaming significantly improves VA,6 11 15 and may reduce interocular suppression.15 21 Nonetheless, one study has reported no improvement in BCVA.22
The objective of this study was to determine the efficacy of binocular therapy for amblyopia, and compare it versus that of patching in terms of change in BCVA and stereoacuity. A meta-analysis was also performed to estimate the overall effect of the six RCTs included in this study.
No heterogeneity detected in pretreatment BCVA. The severe heterogeneity noted in this study is explained by the diversity of binocular therapies and sample sizes. The mean difference indicated that the beneficial influence of the binocular therapy for amblyopia was significant. The test result for the combined effect was Z=3.01 (p=0.003), demonstrating that binocular therapy was effective. Meanwhile, patching group may be better significantly as shown in figure 2A. However, we did not observe improvement in stereoacuity or statistical significance between the two groups; this may be attributed to the limited raw data.
This finding is consistent with the results of a study conducted by Kelly et al6 that reported improved in VA (p<0.001) and stereoacuity (p<0.045), as well as reduction in the extent (p<0.005) and depth (p<0.003) of suppression from baseline to the week 2 visit. According to a study performed by Li et al23 including 50 children with amblyopia (aged 4–12 years; 25 per group), BCVA improved from 0.47 to 0.39 log MAR (p<0.08) after 4 weeks of game playing (4 hours per week; p<0.001) in comparison with the sham group in which there was no improvement. Moreover, BCVA was stable 3 months after cessation of treatment.11
This outcome is contrary to that reported by Holmes et al Among 138 participants with amblyopia (aged 7–12 years; 69 per group), BCVA improved by 0.026 log MAR (p<0.71) after 4 weeks of game playing (4 hours per week, p<0.001) in comparison with the spectacle group in which there was no improvement.22 These findings indicated that there was no benefit to BCVA or stereoacuity by the dichoptic binocular Dig Rush game. Notably, in the study conducted by Holmes et al, patients with prior treatment history would have less VA,22 and the limited treatment time of iPad gaming prevented the development of binocular vision in children.8 9 Moreover, it remains unclear whether poor treatment adherence was responsible for the low treatment response to binocular therapy. Li et al reported that a supervised, in-office treatment with movies resulted in a mean VA gain of 0.2 log MAR in merely 2 weeks with 9 hours of treatment.23 This suggested that better compliance with more appealing gaming and more frequent supervision may lead to larger VA gains. In contrast to the present study, binocular therapy has been shown to yield more robust VA improvements in adults with amblyopia. In a study conducted by Gao et al involving 115 participants with amblyopia (aged 8–35 years), VA improved by 0.06–0.12 log MAR from baseline in the active group and by 0.07–0.10 log MAR in the placebo group within 6 weeks.24 The binocular game used in that clinical trial did not improve visual outcomes more than the placebo video game, despite increases in fellow eye contrast during game play. A possible explanation for this may be that the mechanisms of the binocular therapies and patching were different. Hence, combining these two approaches may enhance the response to treatment.19 These binocular vision effects can be enhanced by non-invasive brain stimulation techniques, possibly by reducing the suppression of inputs from the amblyopic to the cortex.8 Previous studies reported improvement in stereoacuity and reduction in the extent of suppression.6 10 These effects may be attributable to the type of stereoacuity test used. Improvements may be detected more easily using the Frisby or contour tests rather than random dot tests.25
Strength and limitations
To the best of our knowledge, this is the first meta-analysis evaluating the efficacy of binocular iPad gaming versus patching for amblyopia in children. Our study included only RCTs to ensure the accuracy of data. This investigation has important implications for developing new binocular therapy as a supplementary method to patching for amblyopia in children.
Limitations of this study include the small sample of six trials,15–20 and lack of statistical analysis of masked data.25 Randomisation was inadequate in one trial.16 Therefore, we used a strict evaluation tool to avoid selecting low-quality articles.12 Several trials15 17 26 have demonstrated low adherence in binocular therapy groups, which may influence the final treatment outcome.
In conclusion, the study revealed a statistically significant difference in terms of change in BCVA between binocular therapy and patching; however, improvement in stereoacuity was not observed. Binocular treatment is effective in amblyopia therapy and could be used as a complementary method to patching for the management of strabismic, anisometropic or mixed amblyopia in clinical practice. Nevertheless, it remains unclear whether poor treatment adherence or inappropriate treatment duration is responsible for the observed minimal response to binocular therapy. Therefore, further RCTs with larger sample sizes and longer treatment durations are warranted to assess efficacy in treating amblyopia and disease recurrence.
Acknowledgments
The authors thank the investigators who contributed to discussions, as well as the writing and reviewing of the manuscript.
References
Footnotes
Contributors JY and CC contributed substantially to the conception and design of this paper. CC, YD and QZ conducted the literature searches and extracted the data from published papers. CC and QZ drafted the paper and carried out statistical analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.