Article Text

Abstract
Objective Intraocular lens (IOL) opacification may cause severe visual impairment. The pathogenesis remains unclear. The aim of this study was to analyse opacification patterns in different IOLs. Therefore, this multicentre, retrospective, observational study was conducted at Ludwig-Maximilians-University, Munich, Germany and University-Hospital Basel, Switzerland.
Methods and analysis In this study, 75 opacified IOLs were identified and classified after extraction. Macroscopical photo documentation, light and electron microscopic analysis were done.
Results 68 acrylic-hydrophilic single-piece-IOLs, 1 acrylic-hydrophilic 3-piece-IOL, 6 acrylic-hydrophobic 3-piece-IOLs were extracted. The dataset comprised IOLs known for opacification and IOLs not having been reported yet. 67 IOLs showed a fine-granular and 8 IOLs a crust-like opacification pattern. According to literature, 62 of the fine-granular opacified IOLs were graded into type 1 (processing/packaging-induced primary opacification) and 13 into type 2 (secondary opacification of unknown aetiology). The anterior surface of the IOLs was affected in all 75 IOLs, the posterior surface only in 23 cases. Of all 67 fine-granular IOLs, 43 had a central defect and 21 had a zone without opacification (clear islet).
Conclusion In our series, the morphology of IOL opacification did not follow the existing pathogenetic classification that strictly discriminates between primary and secondary causes. Fine-granular IOL opacification occurs with similar patterns in both type 1 and type 2 IOL opacification, while a crust-like pattern was only detected in type 2 IOL opacifications. Consequently, susceptibility of an IOL to opacification is caused by a multifactorial combination of material and processing properties as well as individual (pathological) conditions of the patient.
- lens and zonules
- optics and refraction
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Until now intraocular lens (IOL) opacification patterns were strictly classified into primary (type 1) and secondary (type 2).
IOL opacifications were believed to be an event occurring in specific IOL types.
What are the new findings?
In our series, type 1 and type 2 showed identical opacification characteristics; thus, new pathogenic mechanisms of IOL opacification have to be identified.
How might these results change the focus of research or clinical practice?
By analysing IOL opacifications our study helps to understand the mechanisms for IOL opacifications and to identify new contributing factors.
Introduction
Intraocular lenses (IOL) need to be explanted because of various complications such as IOL dislocation/decentration, incorrect IOL power, glare/optical aberrations, IOL damage, uveitis-glaucoma-hyphaema syndrome, corneal decompensation and IOL opacifications.1–4
IOL opacification is a rare condition, although it can lead to severe visual impairment, reduced contrast sensitivity and glare.5 6
Up to now, IOL opacifications are described in different IOL materials and designs such as silicone, poly-methyl-methacrylate, hydrophilic acrylic, hydrophobic acrylic and hydrophilic acrylic with hydrophobic coating lenses.7
Different ocular and systemic diseases are likely to be associated with IOL opacifications. These include coexisting ocular pathologies such as asteroid hyalosis, uveitis and systemic metabolic diseases like diabetes.6 8 9 Furthermore, surgical interventions that is, pars plana vitrectomy (ppv), Descemet’s Stripping (Automated) Endothelial Keratoplasty, injections of air, gas or silicon oil and intraoperative or secondary manoeuvres such as, the use of different adjuvants, for example, viscoelastics or medications, for example, recombinant tissue Plasminogen Activator (rtPA) were found to cause IOL opacifications.10 Another explanation is that an increased inflammation with release of cytokines and interleukins and alteration of the pH of the aqueous humour and with breakdown of the blood-aqueous barrier (BAB) causes an increased concentration of calcium in the anterior chamber leading to calcium phosphate deposits on the lens surface, causing opacification.11 12 Other propositions are problems in the IOL manufacturing process, such as contaminations, sealing, packaging and storage problems. As previously described by Neuhann et al,13 the opacification patterns of our IOL set were classified into primary (type 1) opacification and secondary (type 2) opacification. We did not further concentrate on false-positive diagnosis of IOL calcification defined as type 3.
The aim of this study was to identify and analyse explanted IOLs with opacifications and investigate opacification patterns in IOLs explanted as referred to type 1 and type 2.
Methods
This multicentre, retrospective, observational study was performed at the Department of Ophthalmology, University Hospital, LMU Munich, Germany and the Eye Clinic, University Hospital Basel, Switzerland between November 2010 and March 2018.
All IOL explants were screened for opacifications by matching the explants with the clinical diagnosis in our patient database. The patient database (SAP Deutschland SE & Co. KG, Walldorf, Germany) was filtered by four search criteria: (1) clinical diagnosis, (2) clinical diagnosis code (International Statistical Classification of Diseases and Related Health Problems, 10th revision, German Modification), (3) surgical procedure, (4) surgical procedure code (Diagnosis Related Group (DRG) code).
Patients that were identified having had an IOL explantation due to IOL opacification were included in this study. The subjective symptoms in the medical history that led to IOL explantation included reduced objective and/or subjective best-corrected distance visual acuity, reduction in contrast sensitivity or other subjectively perceived disorders such as glare. All patients had undergone a full preoperative clinical examination with best-corrected distance visual acuity (BCDVA), Goldmann tonometry, biomicroscopy and funduscopy after pupil dilation. As a routine, patients with IOL opacifications were photo documented preoperatively with slit lamp photography (Haag-Streit IM 900) and retro-illumination in most cases. The IOL exchange was performed through a clear cornea incision or a sclero-corneal tunnel. A secondary IOL was implanted and fixated in one of the following positions: the capsular bag, the ciliary sulcus, retro-pupillary or sclera. All explanted IOLs were rinsed with Alcon BSS sterile solution directly after explantation to wash up remnants of the capsular bag. In rare cases, residues of the capsular bag could not completely be removed by rinsing. They were left adherent to the IOL in order not to manipulate the IOL material. The IOLs were then archived in a dry and sealed form. A full postoperative evaluation including BCDVA, Goldmann tonometry and biomicroscopy were performed in all patients 1 hour after the surgery.
IOL photography
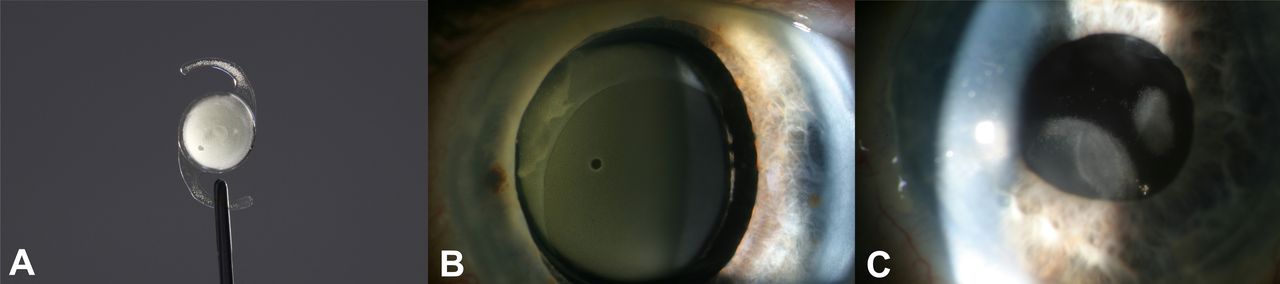
After surgery, the explants were macroscopically photographed by a professional photographer in a standardised manner (figure 1A). A Canon EOS 5D Mark II photo camera with a 100 mm Canon Makro EF 1:2.8 IS USM prime lens and a Canon Makro Ring Lite MR 14 EX II flash were used (Canon, Tokyo, Japan). The setting was illuminated using a conventional desk light with an Osram 7 W 12 V GY6.35-socket halogen bulb (Osram Licht, Munich, Germany). The IOLs were held at one of their haptics with anatomical forceps and then photographed with trans-illuminating light. This allowed whole mount images of the explanted IOLs in order to identify the IOL type (table 1) and highlight the opacifications on the lens surface. A representative of each explanted IOL type is displayed in online supplemental figure 1. The respective IOL manufacturers were informed prior to publication of this study.
Supplemental material
Supplemental material
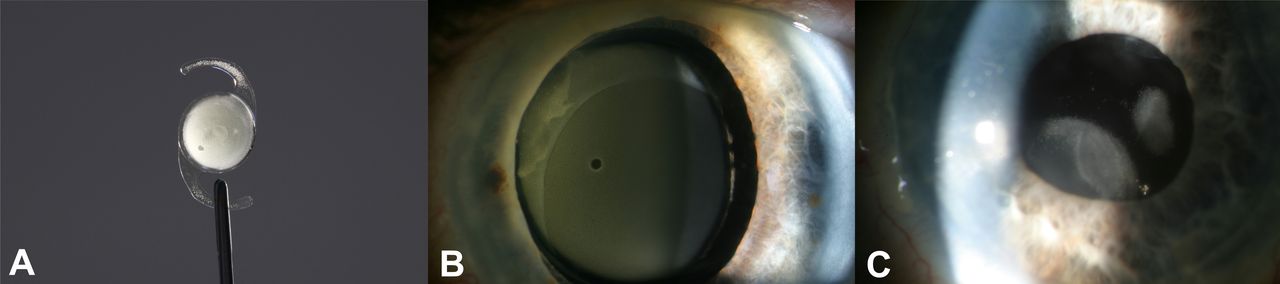
(A–C) Photo documentation.
Patients’ characteristics
Three-dimensional digital high dynamic range microscopy
Microscopy was performed with a high precision digital microscope, Keyence VHX-5000 (Keyence, Osaka, Japan). The images were taken from the anterior and posterior optic and the haptics according to a predefined scheme. A three-dimensional and a high dynamic range image was taken at 30×, 100× and 500× magnification.
Scanning electron microscopy
For further analysis, one IOL was sent to the University of Regensburg (Germany) for scanning electron microscopy using a FEI/Philips XL-30 device (Philips Research Headquarters, Eindhoven, The Netherlands) with the following magnification levels: 52×, 110×, 150×, 250×, 500×, 1000×, 1280×, 1450×, 1580×, 5040×, 10 230×. Having scanned the surface of the IOL, the IOL was then cut vertically with a razor blade and a scan was recorded of the cutting area. The photographs were reviewed by two independent investigators (MM and DRM) and characteristics of the IOL opacification were documented. The morphology of the opacification (localisation, extension and pattern) was hereby assessed.
Statistical analysis
All obtained data, including clinical data of patients, such as general comorbidities, ophthalmic conditions, details of the cataract surgery and the IOL exchange, intraoperative and postoperative complications, additional intraocular procedures and medications were categorised using Microsoft Excel (Microsoft, Redmond, Washington, USA). Statistical analysis was performed using IBM SPSS (V.22 for MacOS, IBM, Armonk, New York, USA) for MacOS. Normal distribution of the data was tested using the Kolmogorov-Smirnov test implemented in the SPSS software. As none of the tested variables was normally distributed, a Wilcoxon signed rank test was chosen to evaluate if selected variables showed a statistically significant difference pre-IOL/post-IOL exchange. If there was a statistically significant difference effect size r was calculated.
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Results
In total 75 opacified IOLs of 66 patients were analysed. Patients’ demographics are listed in table 2.
Functional outcomes
Most of the explanted opacified IOLs were Oculentis LS-312Y. Online supplemental figure 2 shows the time of cataract surgery and the implanted IOLs. Retrospective analysis revealed diabetes mellitus as relevant general medical history in 19 (29%) patients with a mean age of the study population of 75 years (table 1). The overall prevalence of diabetes mellitus increases with age.14 15 The age-matched gender-combined diabetes prevalence in Germany ranges from approximately 21% to 25% which quite well matches the overall diabetes prevalence of our study population of 29%.15 Associated ophthalmic pathologies were present in 25 (33%) eyes including uveitis, glaucoma, vitreous haemorrhage, synchysis scintillans and epiretinal fibrosis (table 1). A long-term therapy with topical medications 11 (15%) eyes (table 1). Previous ophthalmic interventions were found in eight (11%) eyes including intravitreal injections, vitrectomies with silicone oil and gas tamponade, synechiolysis, cyclophotocoagulation, neodymium-doped yttrium aluminium garnet (Nd:YAG) laser posterior capsulotomy. Some eyes had multiple interventions (table 1).
Supplemental material
In 73 (97%) eyes, a secondary IOL was implanted and 2 (3%) eyes were left aphakic. During IOL exchange the following IOLs were implanted (online supplemental figure 3). Anterior vitrectomy was performed intraoperatively in 39 (52%) eyes. There were no details regarding the initial IOL implantation during cataract surgery and the intraoperative and postoperative complications as this was performed ex domo. Functional visual acuity outcomes are displayed in table 2.
Supplemental material
Overall opacification (n=75)
When analysing the IOLs microscopically, two types of opacification were identified in our multicentre set of explanted IOLs (table 3). A fine-granular opacification pattern was found in the majority of cases (n=67; 89.3%) and a crust-like pattern was present in 8 (10.7%) IOLs. The colour and structure of the opacification varied as shown in figure 1B,C.
List of explanted opacified IOLs and opacification characteristics
Morphological classification: fine-granular (n=67) versus crust-like (n=8)
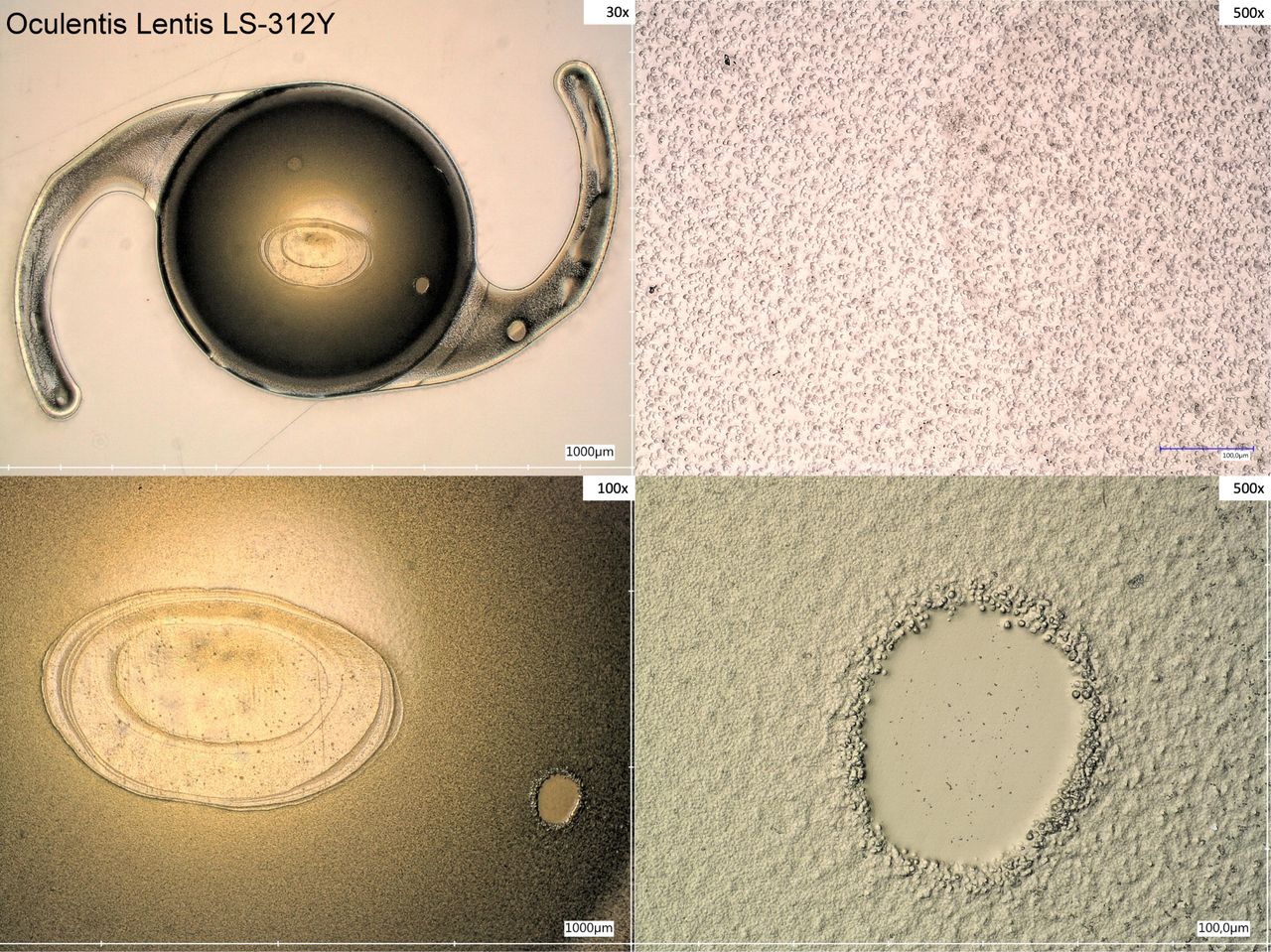
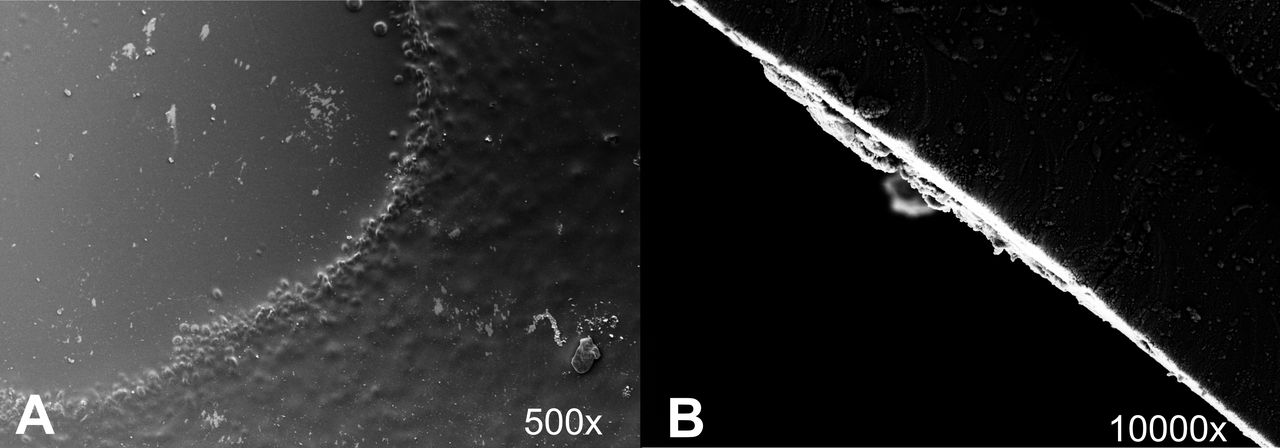
The 67 IOLs with the fine-granular opacification showed a similar pattern (table 3): all showed opacifications on the anterior lens surface and in 19 (28%) cases the posterior lens surface was also affected (figure 2 and online supplemental figure 4). The haptics of 59 IOLs (88%) showed the same opacification type (figure 2 and online supplemental figure 4). The opacification did not always present as homogenous surface but showed in 21 (31%) cases a small round zone in the mid-periphery of the optic, which was not opacified and is referred to as ‘clear islet’. This clear islet was characterised by a deposit of accumulation at the rim of this clear zone (figure 2 and online supplemental figure 4). Furthermore, a defect within the IOL optic was present in 43 (64%) cases (figure 2, online supplemental figure 4, table 3). Electron microscopy in a 500× magnification of one lens with this fine-granular pattern showed the described ‘clear islet’ with accumulation of granular material at the rim (figure 3A). Moreover, the opacification was accumulated only in the superficial layer of the IOL (figure 3B).
Supplemental material

Fine-granular opacification pattern—Oculentis intraocular lens.

(A, B) Scanning electron microscopy (SEM).
Twenty-one (28%) eyes of 16 patients of the fine-granular IOLs revealed diabetes mellitus as relevant general medical history. Associated ophthalmic pathologies were present in 13 (19%) eyes: 1 uveitis, 7 glaucoma and 7 vitreoretinal pathologies: epiretinal membrane, 5 vitreous haemorrhages, 1 synchysis scintillans. A long-term therapy with topical medications was administered in seven (10%) eyes. Previous ophthalmic interventions were found in 19 (28%) eyes: 2 intravitreal ranibizumab and 18 YAG laser capsulotomies. Sixty-two (93%) of the 67 fine-granular opacified IOLs were classified as type 1 IOLs. The remaining five fine-granular IOLs were type 2 IOLs (table 3).
The other eight opacified IOLs presented with a crust-like pattern with a different morphological appearance (figure 4), found in various IOL types (table 3). All of the eight crust-like IOLs were classified type 2. Examples of this opacification pattern can be found in different magnifications (30×, 100×, 500×) in figure 4 and online supplemental files 1; 6; 7. None of the crust-like opacified lenses showed the previously mentioned clear islet and no defect in the IOL optic. In three (38%) cases, diabetes mellitus could be identified (Acri.Smart, Tecnis, Quatrix). Associated ophthalmic pathologies were present in six (75%) IOLs: two uveitis (Tek-Lens, Tecnis), four glaucoma (Acri.Smart, Quatrix, Tecnis) with a long-term therapy with topical medications. Previous ophthalmic interventions were found in seven (88%) cases: one intravitreal dexamethasone implant, two intravitreal bevacizumab, three vitrectomies with silicone oil (Quatrix, Tecnis, Domicryl), one vitrectomy with gas (Tecnis), one synechiolysis and one cyclophotocoagulation, four YAG laser capsulotomies.
Supplemental material
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Crust-like opacification pattern.
Pathogenetical classification: primary (type 1) (n=62) versus secondary (type 2) (n=13)
The primarily opacified (type 1) IOLs are characterised by an opacification that occurs due to irregularities of the IOL material or the packaging of the IOL, mostly independent of patient characteristics.5 The type 1 opacified IOLs of our set consisted of 62 (83%) IOLs and showed a fine-granular opacification pattern (table 3). Eighteen (29%) of the type 1 IOLs had previous interventions (1× intravitreal medical treatment (IVT), 18× YAG-laser posterior capsulotomy) and six (10%) were under continuous topical therapy. Median age at explantation of type 1 IOLs was 78 years of age.
IOLs that are not known for their tendency to opacify and for which no history of opacification exists to date were classified secondary opacified IOLs (type 2). Secondary IOL opacification is defined by opacification due to comorbidities of the patient or other unknown causes not primarily related to IOL material failures.
Our set of 13 type 2 opacified IOLs consisted of 7 three-piece and 6 single-piece IOLs (table 3). The affected lenses were implanted between 2010 and 2011. Two IOLs were associated with diabetes mellitus in the general medical history. Associated ophthalmic pathologies were present in two eyes: one glaucoma and one vitreous haemorrhage. A long-term therapy with topical medications was administered in one eye. Previous ophthalmic interventions had been performed on one eye (intravitreal ranibizumab).
The mean period between implantation and explantation was for type 1 IOLs 52 months with a 95% CI (48 to 56) and for type 2 82 months with a 95% CI (41 to 123). The performed Mann-Whitney U test (p=0.01) showed a statistically significance between type 1 and type 2 opacified IOLs.
Discussion
IOL opacification is still a frequent reason for IOL exchange surgery.3 16 Neuhann et al defined three types of IOL opacifications due to precipitates consisting of calcium and phosphate complexes on the IOL surface and subsurface, respectively.13 Calcium bicarbonate (CaHPO4) and hydroxyapatite (Ca5(PO4)3(OH)) are among the possible complexes that form the opacification.9 17 Protein precipitates seem to play a minor role (type 3, ‘pseudocalcification’13).4 Primary IOL opacification—herein referred to as type 1—are supposed to be caused by the IOL itself and usually occur in distinct IOL types or distinct production series. Secondary IOL opacification is herein referred to as type 2.13 18 There are various factors discussed to contribute to IOL opacification.
Previous ophthalmic interventions
Asteroid bodies in eyes with asteroid hyalosis or after posterior capsulotomy might contribute to the opacification, especially of the posterior IOL surface.9 19 20 Additionally, leftover fragments of the phakic cataract lens after phacoemulsification might trigger IOL opacification.17 Moreover, repeated intravitreal antivascular endothelial growth factor injections are discussed to trigger IOL opacification.21 Very high incidence seems to occur after DMEK surgery requiring intracameral air tamponade a ppv using gas or air endotamponade.18 22–27 It is assumed that direct contact with gas or air alters the material integrity of the IOL facilitating opacification. Usually, the haptics of an IOL are not prone to exposure of gas or air. However, the process of opacification by gas or air tamponade may be triggered in a central area of the lens and continues to spread to peripheral IOL parts such as the haptics. In our study, the majority of haptics were opacified (64, 85%) and this process seems to be independent on previous interventions. We could further note that in 23 (31%) cases IOL opacifications were found on the anterior as well as on the posterior surface of the IOL, and a single-side affection was found in 52 (69%) of all IOLs. Interestingly, there was no IOL with a posterior surface-only affection. Of the 23 IOLs with both-sided opacification, only 9 (39%) have had previous interventions: 3 (13%) vitrectomies (1× gas, 2× silicone oil) and 6 (26%) posterior YAG-laser capsulotomies. Of the 52 (69%) IOLs with an anterior surface-only affection, none has had intraocular gas or air tamponade. In our opinion, this is an indication that the influence of air or gas tamponade during vitrectomy on IOL opacification might be of less importance.12 In our cohort, the opacification pattern did not seem to be dependent on secondary procedures in the anterior or posterior segment.
Alteration of aqueous humour pH
The complexed calcium and the free, ionised calcium (Ca2+) are diffusible. The protein-bound (mostly albumin-bound) calcium fraction is not diffusible.28 A more alkaline pH increases binding of Ca2+ to proteins and, at the same time, decreases levels of ionised Ca2+.28 Furthermore, a more alkaline pH goes along with an increase of HCO32− ion levels which results in increased levels of complexed calcium in form of calcium bicarbonate (CaHCO3) and decreased levels of free, ionised Ca2+.28 Consequently, a more alkaline pH increases CaHCO3 and protein-bound calcium levels. Hence, the diffusible calcium fraction does rather decrease than increase. A more acid pH as it is present in inflammatory processes might consequently increase the diffusible calcium fraction and therefore promote increased calcium levels within the aqueous humour.
Blood-aqueous barrier breakdown
BAB breakdown is supposed to happen in patients having had complicated intraocular surgery, patients with degenerative diseases such as diabetic retinopathy and inflammatory diseases like uveitis as well as in children with persistent hyperplastic primary vitreous.29 BAB interruption is discussed to ease calcium diffusion from the blood into the aqueous humour. According to literature, human blood serum contains a level of calcium of 2.2–2.7 mmol/L.28 Literature about aqueous humour calcium concentration ranges 1.4–2.5 mmol/L.30 31 Consequently, increased diffusion of complexed and ionised calcium into the aqueous humour due to BAB interruptions seems to be possible if a significant diffusion gradient is present.
Increased aqueous humour calcium concentration
In order to increase calcium levels within the aqueous humour, the systemic formation of ionised and complexed calcium (within the blood) must be increased and diffusion must be facilitated. Alternatively, calcium levels could be increased locally within the aqueous humour, for example, by applying eye drops. It has been shown that calcium and other electrolytes contained in eye drops can cause corneal calcifications and the electrolytes are able to penetrate the anterior segment and accumulate on the IOL.32 Especially after complicated, invasive surgery these eyes usually undergo more intensified postoperative treatment with eye drops.33–36 This might explain differing grades of IOL opacifications.
IOL material and packaging properties
If IOL material properties allowed easier access of the physiologically present calcium into the IOL, opacification might be possible without electrolyte disorders. Moreover, IOL packaging containing silicone molecules seems to favour calcium phosphate adherence to the IOL surface, especially in interaction with long saturated fatty acids that are physiologically present within the aqueous humour.9 Furthermore, IOL surface configuration might play a role in susceptibility to opacification deposits. Hydrophobic acrylic IOLs were found to have a smoother surface configuration than hydrophilic IOLs.37 This is shown to help prevent posterior capsule opacification.37 A regularity, smoothness might also be a preventing factor for calcium phosphate deposits on the IOL surface. However, it is still controversial whether IOL opacification occurs more often in hydrophilic IOLs as most of the series report hydrophilic IOL opacifications. However, no robust data are obtainable to clearly support this conclusion. While our dataset documents a large number of hydrophilic acrylic lenses and hydrophilic-hydrophobic co-polymers, we also found six (8%) hydrophobic lenses with opacifications. Our data demonstrate that opacification patterns usually identified in type 1 may also be found in type 2 opacifications. In our dataset, five type 2 opacified IOLs of two different manufacturers (Argonoptics, Johnson & Johnson) showed both macroscopically and microscopically identical opacification patterns like the IOLs by Oculentis classified as type 1. In 21 (28%) (18 type 1 and 3 type 2) IOLs, we found a central spot without opacification (‘clear islet’). To our understanding, the reasons for this non-opacified zone remain unclear. However, as the clear islet is found in type 1 and type 2 IOL opacifications of different manufacturers, a reason independent from the IOL processing is supposed to play a significant role.
Implanted period
In general, it is assumed that the longer the IOL stays in the eye (implanted period (IP)) the higher the risk for opacification caused by degradation of the IOL material, inflammation, ultraviolet light exposure, ophthalmic interventions.6 Compared with type 1, we could note that type 2 opacified IOLs in our study had stayed significantly longer within the eye before explantation. Hereof, one might conclude that type 2 opacification shows milder symptoms or needs longer to become clinically apparent to the patient. However, patients as well as ophthalmic surgeons might be hesitant towards IOL exchange in complex cases with high risk of complications and low predicted visual gain, even though IOL opacification might be impairing. Pros and cons of an IOL exchange should be traded off to reliably identify patients that might benefit from surgery. If this is done carefully, visual acuity can be rehabilitated or significantly improved by IOL exchange surgery, as could be shown in this study (table 1). Postoperative visual gain might be limited by existing ocular pathologies such as macular oedema under intravitreal injection therapy, epiretinal fibrosis, glaucoma and diabetes mellitus (table 2).
This study bears several flaws. First of all, the study design is not prospective. Consequently, we cannot exclude that there may be opacification patterns which result in minor symptoms being under-reported in our study. Moreover, the retrospective study design does not allow any further examination modalities that would have been of interest such as puncture of the anterior chamber with analysis of the aqueous humour. Additionally, there might be cases with severe IOL opacifications but reduced visual acuity prognosis after IOL exchange because of the complexity of the surgery. IOL opacification in eyes that require silicone oil tamponade are under-reported in our study as well as in other studies. Furthermore, our study was not able to refer to standard postoperative care, as the majority of these patients were previously operated in outpatient private clinics, undergoing varying topical postoperative treatments and medications.
In summary, our study demonstrates that IOL opacifications occur in both hydrophilic and hydrophobic copolymer IOLs. We confirm previous studies that differentiate between type 1, type 2 opacifications, however identified patterns observed in type 1 and type 2 opacifications show similarities. This leads us to conclude that borderline types exist and that IOL opacification is a process that occurs gradually and affects different types of IOLs. This might imply that other risk factors for IOL opacifications than the ones that are discussed up to now may exist.
Acknowledgments
The authors would like to thank the colleagues from University of Regensburg (Germany) for their uncomplicated help with scanning laser electron microscopy (SEM).
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
MM and DRM contributed equally.
Presented at Presented at the XXXV Congress of the ESCRS, October 2017, Lisbon, Portugal.
Contributors MM: concept and design; data acquisition; data analysis; drafting manuscript; critical revision of manuscript; supervision final approval. DRM: concept and design; data acquisition; data analysis; drafting manuscript; critical revision of manuscript; statistical analysis; supervision final approval. EV: critical revision of manuscript; supervision final approval. CD: data acquisition; critical revision of manuscript; supervision final approval. DG: data acquisition; critical revision of manuscript; supervision final approval. MS: critical revision of manuscript; supervision final approval. PWH: data acquisition; critical revision of manuscript; supervision final approval. SP: critical revision of manuscript; supervision final approval. AW: concept and design; data acquisition; data analysis; drafting manuscript; critical revision of manuscript; supervision final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Approval was obtained from the institutional review board (IRB). This study adheres to the tenets of Declaration of Helsinki. Written informed consent regarding the IOL exchange was provided and signed by each subject.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.