Article Text

Abstract
Objectives Dry eye is common when external beam radiation is used for the treatment of choroidal melanoma (CM). As meibum structure and composition have been related to dry eye, we determined if plaque bachytherapy for CM alters meibum composition.
Design 1H-NMR spectroscopy was used to measure the lipid composition of meibum.
Setting The University of Louisville, Kentucky, USA.
Participants All 13 participants had CM and one participant had iris melanoma.
Main outcome measures Cholesteryl ester (CE) to wax ester (WE) ratio, amount of meibum esters (ME) and meibum lipid saturation were measured.
Results ME decreased by 80%±18% (±99% CI) in 11 eyes that were treated compared with the contralateral untreated eye. ME increased by 181% in two eyes that were treated compared with the contralateral untreated eye. The mole % CE/WE for meibum was significantly (p<0.0001) 67% lower in eyes that were irradiated compared with control eyes from donors without CM and were not treated. Plaque brachytherapy induced the de-esterification of CE. The intensity of the meibum cis double bond resonances did not change significantly (p>0.05).
Conclusion Eyes that had plaque brachytherapy had a lower amount of expressible meibum and a lower CE/WE ratio compared with meibum from the contralateral eye that received no treatment and eyes that did not have uveal melanoma. Both the quality and quantity of meibum should be considered in designing a therapy for dry eye after plaque brachytherapy.
- eye lids
- ocular surface
- pathology
- tears
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Dry eye is common when external beam radiation is used for the treatment of choroidal melanoma.
Meibum structure and composition have been related to dry eye in patients that did not have plaque brachytherapy.
What are the new findings?
The amount of expressed meibum in eyes that had plaque brachytherapy was 80% lower in 11 of 14 eyes compared with the contralateral eye.
Both the total cholesterol moieties and cholesteryl ester were lower relative to wax ester in meibum from eyes that had plaque brachytherapy compared with the contralateral eye that received no treatment and eyes that did not have uveal melanoma.
The intensity of the meibum cis double bond resonances did not change with plaque brachytherapy.
How might these results change the focus of research or clinical practice?
Meibomian gland dysfunction should be considered when treating patients for dry eye after plaque brachytherapy.
Both the quality and quantity of meibum should be considered in designing a therapy for dry eye after plaque brachytherapy.
Introduction
Uveal melanoma is the most common primary intraocular malignancy in adults. It most commonly originates in the choroid (90%) followed by the ciliary body (6%) and then iris (4%). Enucleation was the primary modality of treatment for uveal melanoma in the 1970s prior to the Colloborative Ocular Melanoma Study.1 This large multicentre trial demonstrated the safety of plaque brachytherapy with respect to long-term mortality and tumour control.1 Iodine-125 is the most commonly used radioisotope, and the American Brachytherapy Society recommends 0.60–1.05 Gy/hour over three to seven consecutive days.2
Dry eye is very common, 47%, when external beam radiation is used for the treatment of uveal melanoma.3 The incidence of dry eye was 24% when proton beam radiotherapy was used to treat uveal melanomas.4 Clinical dry eye is much less common with plaque brachytherapy in view of the localised radiation and the posterior location in choroidal melanoma. Dry eye was reported in 8.3% of patients at an average of 20.7 months after treatment.5 With respect to iris melanoma, only 2 out of 23 patients treated with ruthenium plaque had clinical dry eye. Even with the anterior location, the dry eye incidence was low, and it was postulated that the reason was that lacrimal gland and conjunctival goblet cells were not included in the field of irradiation, in contrast to proton beam therapy or stereotactic radiation.6 In contrast to this clinical study, histopathological evaluation of the conjunctiva following plaque brachytherapy suggested that epithelial stratification and distributional changes in ocular mucins could lead to development of dry eye.7
Meibomian glands, which are sebaceous in nature, are more sensitive to irradiation and are more permanently altered than other sebaceous glands like glands of Zeis.8 Following external beam radiation, irreversible structural damage to the meibomian glands have been documented in patients with orbital lymphoma.9 Meibomian gland dysfunction (MGD) contributes to dry eye.10–15 The meibomian gland, located in the eye lids, produce meibum, the major source of tear film lipid layer (TFLL).16 The TFLL contributes to tear film stability.15 1H-NMR spectroscopy has been used to measure general meibum composition.17–26 The relationships between meibum composition, structure and tear film stability determined using a spectroscopic approach has been reviewed.27 Donors with dry eye due to MGD have a lower ratio of cholesteryl ester (CE) to wax ester (WE) compared with donors without dry eye.26–28
In the current study, 1H-NMR spectroscopy was used to measure the amount and general composition of meibum from patients who had plaque brachytherapy to treat uveal melanoma. The goal of the study was to determine if plaque brachytherapy induces changes in the meibum. It would also aid in understanding the pathophysiology of dry eye following radiation, to determine if it primarily aqueous deficiency or evaporative dry eye due to MGD.
Methods
CDCl3 was obtained from Sigma-Aldrich (St. Louis, Missouri, USA).
Collection and processing of human meibum
Meibum was collected from 14 patients who underwent plaque brachytherapy for uveal melanoama at the Department of Ophthalmology, the University of Louisville. Written informed consent was obtained from all donors. All procedures were in accord with the Declaration of Helsinki. Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Meibomian glands were gently expressed by pressing the eyelid with a fingertip with strict attention to avoid touching the eyelid margin during expression. All four eyelids were expressed, and approximately 0.5 mg of meibum lipid was collected per individual for direct spectroscopic study. The expressate was collected with a platinum spatula under a slit lamp, and the pool of meibum was immediately dissolved into 0.8 mL of CDCl3 in a 9 mm microvial with a Teflon cap (Microliter Analytical Supplies, Inc, Suwanee, Georgia, USA). Argon gas was blown over the samples to prevent oxidation. The sample in the vial was capped and frozen under argon gas until analysis. Each eye sample was collected separately. Analyses were performed within 3 weeks of collection of the sample. The samples never came in contact with any plastic to avoid plasticisers. Control CDCl3 spectra were measured to ensure no impurities were present.
NMR measurement
Spectral data were acquired using a Varian VNMRS 700 MHz NMR spectrometer (Varian, Lexington, Massachusetts, USA) equipped with a 5 mm 1H{13C/15N} 13C enhanced PFG cold probe (Palo Alto, California, USA). Spectra were acquired with a minimum of 250 scans, 45° pulse width and a relaxation delay of 1.000 s. All spectra were obtained at 25°C. The tetramethylsilane resonance was set to 0 ppm.
Commercial software (GRAMS 386; Galactic Industries Corp, Salem, New Hampshire, USA) was used for phasing, curve fitting and integrating.
Results
Of the 14 patients who underwent plachytherapy for choroidal melanoma, 9 (64 %) were male, 13 (93 %) were Caucasian and 1 was Hispanic. The patients ages ranged from 51 to 77 years, averaging 61±9 years with a median age of 56 years. All patients had choroidal melanoma with the exception of one patient who had undergone radiotherapy for iris melanoma.
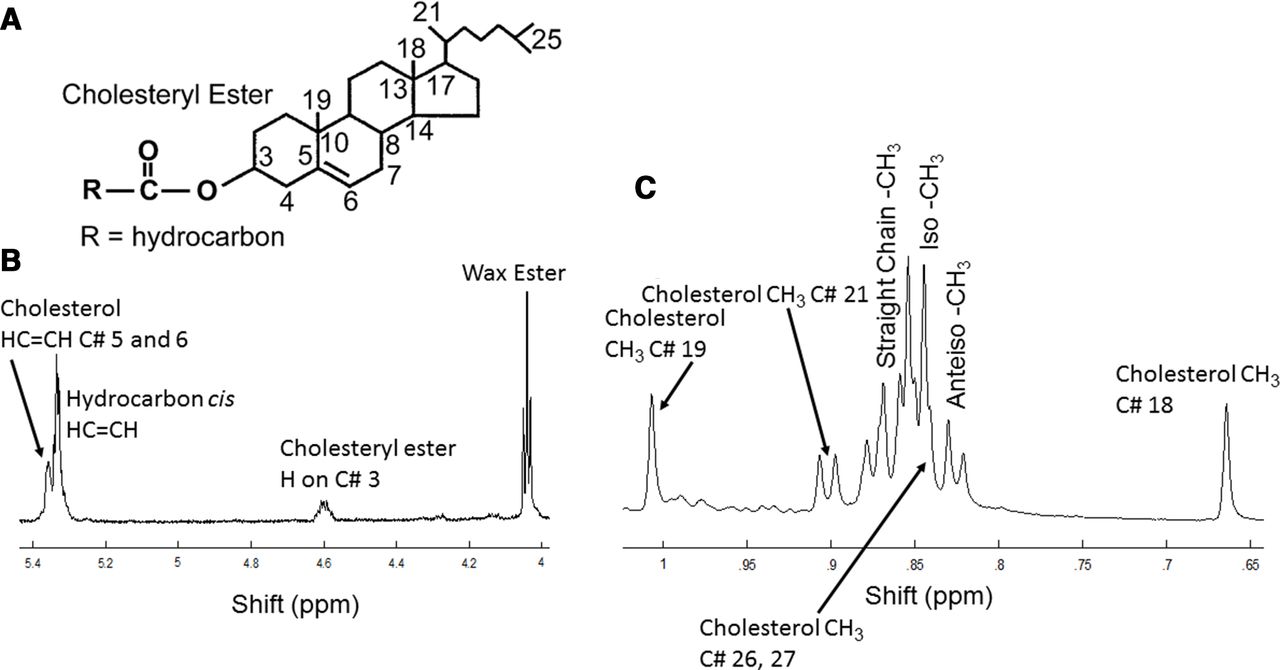
1H-NMR resonances, characteristic of human meibum,26 27 were resolved in the spectra of meibum from eye treated with radiation (figure 1). The total amount of meibum esters decreased by 80%±18% (±99% CI) in 11 eyes that were treated compared with the contralateral untreated eye. The total amount of meibum esters increased by 181% in two eyes that were treated compared with the contralateral untreated eye. The molar % CE/WE for meibum was significantly (p<0.0001) 67% lower in eyes that were irradiated compared with control eyes from donors without choroidal melanoma and were not treated26 (figure 2A). The molar % CE/WE for meibum was significantly (p=0.023) 21% lower in eyes that were irradiated compared with the contralateral eye eyes that did not have uveal melanoma and was not treated (figure 2A). The molar % (cholesterol plus CE)/WE for meibum was significantly (p=0.0008) 38% lower in eyes that were irradiated compared with control eyes from donors that did not have uveal melanoma26 (figure 2A). The molar % (cholesterol plus CE)/WE for meibum was not significantly (p>0.05) different in eyes that were irradiated compared with the contralateral eye eyes that did not have uveal melanoma and was not treated (figure 2B). The intensity of the meibum cis double bond resonances near 5.4 ppm (figure 1) did not change significantly (p>0.05) relative to the WE resonance times 3 at 4 ppm plus the cholesterol resonances at 1 and 0.66 ppm (figure 1) in irradiated eyes compared with the contralateral untreated eyes 0.30±0.03 and 0.28±0.05, respectively.
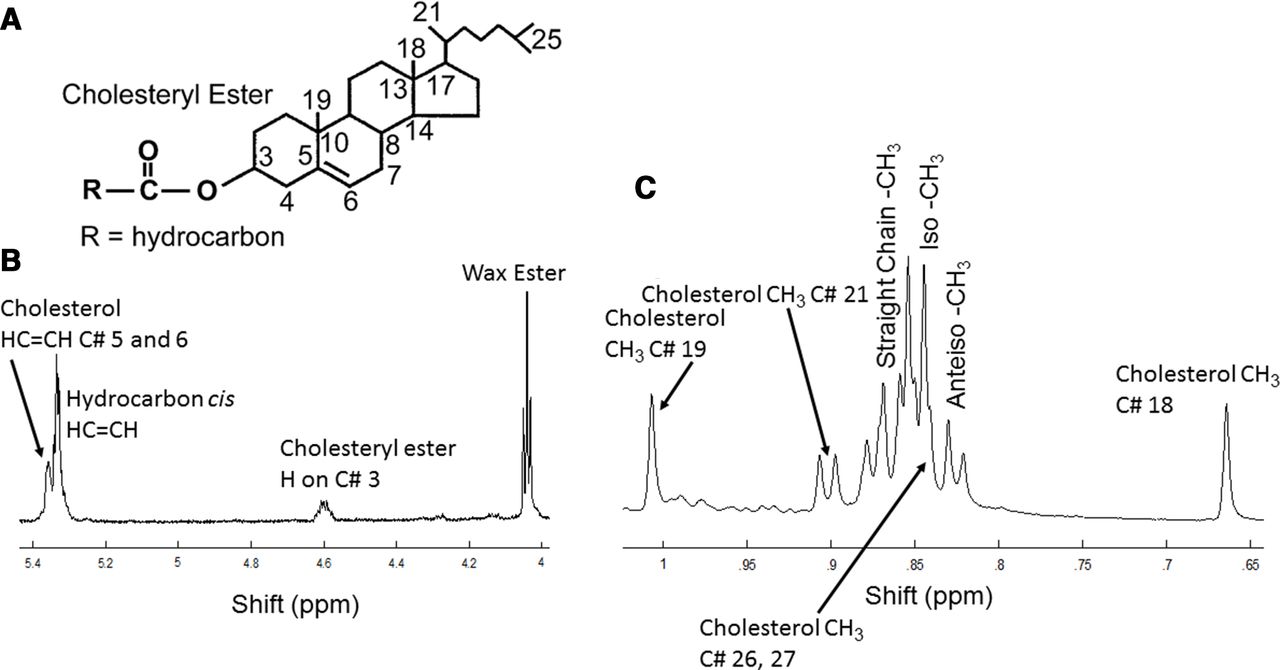
(A) Numbering used in B and C associated with cholesteryl esters. (B and C) Typical 1H-NMR spectrum of meibum from a donor treated with radiation. The resonance due to wax esters near 4.0 ppm is a triplet. The resonance due to cholesterol #C21 is a doublet. Resonances for straight chain CH3 and anteiso CH3 moieties are composed of two major resonances, and the iso-CH3 moieties are composed of two major and one minor (left shoulder) resonance. The resonances due to cholesterol C#26 and 27 are not resolved but buried under the straight chain resonances.

{kind=link}
{kind=link}
Meibum composition. (A) Mole % cholesteryl ester/wax ester calculated from the intensity of the 4.6 ppm and 4 ppm resonances assigned to cholesteryl esters and wax esters, respectively. (B) Mole % cholesterol/wax ester calculated from the intensities of the 1 and 0.66 ppm resonances assigned to cholesterol moieties (see figure 1) and the 4 ppm resonance assigned to wax esters. Data are the mean±SE of the mean. Numbers above bars are the number of eyes. Centre bar is from ref.26
Discussion
Statement of principal findings
The two major findings of this study are: the amount of expressed meibum in eyes that had plaque brachytherapy was 80% lower in 11 of 14 eyes compared with the contralateral eye, and both the total cholesterol moieties and CE were lower relative to WE in meibum from eyes that had plaque brachytherapy compared with the contralateral eye that received no treatment and eyes that did not have uveal melanoma.26
Strengths and weaknesses of the study
The advantages and disadvantages of using a spectroscopic approach to study meibum compositional, and tear film structural and functional relationships have been reviewed.27 As meibum quantity and composition have never been measured in relationship to brachytherapy, the strengths and weaknesses in relation to other studies and important differences in results cannot be discussed. Future studies could be designed to determine the relationships between meibum composition and structure in relationship to the type of radioactive plaques (iodine-125, ruthenium-106, palladium-103 and so on) doses and dose rates and plaque position.
Meibum quantity
The amount of meibum on the eye lid surface reservoir may not be important to tear film stability and dry eye because for donors with meibomian seborrhoea or MGD, the amount of meibum on the eye lid surface was significantly higher as measured using infrared spectroscopy29 or a meibometer.30 Meibum quantity was discussed in a review article15 concluding that the uniformity of the spread film across the ocular surface is a far more reliable indicator than the quantity of meibum. The uniformity of the spread film can be estimated as the ratio of mean thickness to the thickness SD (based on the lipid layer thickness heterogeneity across the eye). Support for this idea comes from a study31 where the central tear film lipid layer thickness range was 120–180 nm (range 60 nm) for healthy individuals, while 185–330 nm (range 145 nm) for dry eye patients.
The thickness of the TFLL may also not be important to tear film stability and dry eye because TFLL thickness is not related to increased tear film breakup time or a decreased thinning as discussed below. The TFLL thickness of patients with seasonal allergic conjunctivitis was thicker than controls, yet the stability of their tear film and breakup time decreased, opposite of what one would expect.31 Furthermore, there was no correlation between TFLL thickness and non-invasive tear break-up time for 29 young32 and 86 older33 subjects without dry eye and 110 patients with dry eye.34 Although the thinning rate and TFLL was significant in one study, the correlation was rather low (r about 0.3).35
The amount of meibum expressed from the meibomian glands, as measured in the current study, could be important to tear film stability. Eyes treated with plaque brachytherapy had 80% less meibum compared with the contralateral eye. It is reasonable to speculate that with such a low amount of meibum in the gland, expression of meibum on blinking could be hindered resulting in a very thin or absent TFLL that could destabilise the tear film. It has been suggested that one needs the absence of a TFLL to observe an increase in the rate of tear evaporation.36–38 Future studies are planned to test this idea.
Meibum quality
The amount of CE was much lower in treated eyes, 0.16 CE/WE (mole/mole), and was lower compared with the amount of total cholesterol moieties ((cholesterol and CE)/WE), 0.31 mole/mole. This indicates that plaque radiation may have de-esterified the CE. In this study, both the total cholesterol moieties and CE alone were lower relative to WE in meibum from eyes that had plaque treatment compared with the contralateral eye that received no treatment and eyes that did not have choroidal or iris melanoma. It is interesting that patients with dry eye due to MGD also have lower CE/WE ratios.26–28 It is attractive to suggest that lower ratios of CE/WE contribute to an unstable tear film and dry eye or perhaps cause the eyes to be more susceptible to dry eye. However, there are a few patients that have normal CE/WE ratios and have dry eye and a few patients that have no dry eye but lower levels of CE/WE.26–28 The degree to which a low level of CE/WE contributes to dry eye or susceptibility to dry eye is under investigation. It is likely that in addition to lower levels of CE/WE, changes in the amount of other moieties such as saturation38 39 and/or proteins,40 41 phospholipids and (O-acyl)-ω-hydroxy fatty acids42 43 contribute to tear film stability.27 Controlled biophysical experiments studying the WE/CE impact on the properties of meibomian films are a worthy direction for further study.
In conclusion, eyes that had plaque brachytherapy had a lower amount of expressible meibum and a lower CE/WE ratio compared with meibum from the contralateral eye that received no treatment and control eyes that did not have a melanoma. Both the quality and quantity of meibum should be considered in designing a therapy for dry eye after plaque brachytherapy.
References
Footnotes
Contributors DB was responsible for collecting and analysing data, writing and submitting the article and funding support. SFA was responsible for collecting and analysing data and editing the manuscript. AR was responsible for designing the study, collecting samples and editing the manuscript.
Funding This work has received support from the National Institute of Health R01EY026180 and an unrestricted grant from Research to Prevent Blindness Inc. New York, New York, USA, GN151619B.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Protocols and procedures were reviewed by the University of Louisville Institutional Review Board # 11.0319, August 2016. All procedures were in accord with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.