Article Text

Abstract
Objective Vision loss has a significant impact on physical, mental and social well-being. Eye clinic liaison officers (ECLOs) have a crucial role in providing holistic care for patients with visual impairment. The aim of this study was to review the work of an ECLO over a period of 1 year at an NHS Trust to determine the volume of work and the areas of support provided by the ECLO.
Methods and analysis A secondary data analysis of the ECLO case notes for all patients reviewed by the ECLO at University Hospitals Birmingham (UHB) NHS Trust during the year 2019, was performed. Demographic data and certification of visual impairment (CVI) status were noted. The main outcome variable recorded was the categories of support provided by the ECLO. Case vignettes were chosen to illustrate the variety of support offered to individual patients.
Results A total of 1127 consecutive participants were reviewed by the ECLO at University Hospitals Birmingham (UHB) NHS Trust during the year 2019. Areas of support most commonly provided by the ECLO included aiding the process of registration for CVI, and assistance in accessing benefits,social support and low vision support. Severely sight impaired patients required significantly more areas of support than sight impaired patients (Χ2=52.7, p=2.16×10−6). Three case vignettes, chosen by the ECLO, highlighted the positive impact of the ECLO with respect to emotional support, practical advice and as a point of contact ensuring continuity of care, also during the COVID-19 pandemic.
Conclusions The ECLO at UHB NHS Trust provides a core patient service within the ophthalmology department by being a key source of practical and emotional support and the crucial link between healthcare, social care and voluntary services.
- low vision aid
- glaucoma
- macula
- rehabilitation
- vision
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this topic?
Visual impairment has a debilitating biopsychosocial impact on the affected individual.
Hospital eye services have a responsibility to ensure that holistic care is provided to patients with visual impairment.
Eye clinic liaison officers (ECLOs) provide this holistic care and form a link between healthcare, social care and voluntary eye services.
What are the new findings?
A quantitative and qualitative assessment of the impact of one ECLO in an NHS Trust.
The ECLO provides many categories of support including aiding the process of registration for certification of visual impairment (CVI), emotional support, and help with accessing benefits and social support.
How might these results change the focus of research or clinical practice?
With increased awareness of the positive contributions of the ECLO, there is hope that funding across NHS Trusts can incorporate such a valuable role.
The ECLO role has the scope to become an integrated part of every NHS ophthalmology service.
Introduction
Approximately 2 million people, in the UK, have significant visual impairment.1 This figure is projected to increase over the years as the prevalence of sight-threatening conditions, such as age-related macular degeneration and glaucoma, continue to rise in a growing, ageing population.2 3
It is well documented that sight loss can significantly reduce quality of life by limiting activities of daily living,4 affecting employment and financial status5 and potentially leading to social isolation. Furthermore, there is an increased risk of depression, suicide,6 cognitive decline7 and falls8 in those with visual impairment. Patients with sight impairment therefore require access to support services for help with all aspects of their well-being. The range of services available includes rehabilitation, mobility training, housing adaptations, access to low vision aids, emotional support and advice regarding benefit entitlement.9 There is considerable variation in the level of service provision across the UK and most patients receive inadequate information about the options available to them. Thus, it can be difficult for patients to navigate the various agencies independently, and those who are not proactive may be disadvantaged.10 It is the responsibility of the ophthalmology team to help patients access these support services since providing holistic care for this vulnerable group of patients is paramount and is the ethos of the Department of Health and Social Care who hold the certificate of visual impairment. Due to the pressure on the hospital eye services,11 however, this role is beyond the scope of the clinician and a dedicated eye clinic liaison officer (ECLO) with knowledge of community-based support is critical.
Prior to the development of the ECLO role, there was a disparity among referral pathways to support services in eye clinics across England and formal links with social support were lacking.12 The establishment of the ECLO role has now filled this gap and formalised a link service providing early emotional support and advice during the time of initial diagnosis for patients, families and carers, while also signposting and initiating referrals to other services. ECLOs form a bridge between healthcare, social care and voluntary services.9 The Department of Health and Social Care stated that it is ‘good working practice to have ECLOs in hospitals’ as they ‘create a good link between health and social care’ and ‘enhance joined up support for the patient’.13
Aim
The aim of the study was to review the work of an ECLO over a period of 1 year at an NHS Trust.
Methods
The written case records created by the ECLO of all patients seen by the ECLO in one NHS Trust from 1 January 2019 to 31 December 2019 were reviewed.
Demographic data and certification of visual impairment (CVI) status were recorded. The main outcome variable collected was the categories of support provided by the ECLO. These included help with accessing benefits, support regarding employment and housing, social support, emotional support, supporting registration (CVI) and low vision support. Any other categories not included in this list were recorded as ‘other’.
Subset analysis considered the effect of sight registration status on the distribution of support given. Cross tabulation with χ2 test of independence was used to assess whether there was an association between the number of categories of support provided by ECLO and the CVI status (sight impaired vs severely sight impaired).
Three case vignettes were chosen by the ECLO purely to illustrate the variety of support offered to individual patients. The first two cases were chosen from the audit period. The third case has been chosen to illustrate the support provided by the ECLO during the COVID-19 pandemic.
Patient and public involvement
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Results
A total of 1127 consecutive patients were reviewed and supported by the ECLO during 2019, including all patients newly registered as sight impaired or severely sight impaired. A total of 477 (42.3%) were men and 650 (57.7%) were women, and the age range was 18–96 years. Fifty per cent of cases seen were registered as sight impaired while 47.6% of the remaining cases were severely sight impaired and a small proportion (2.4%) were not registered.
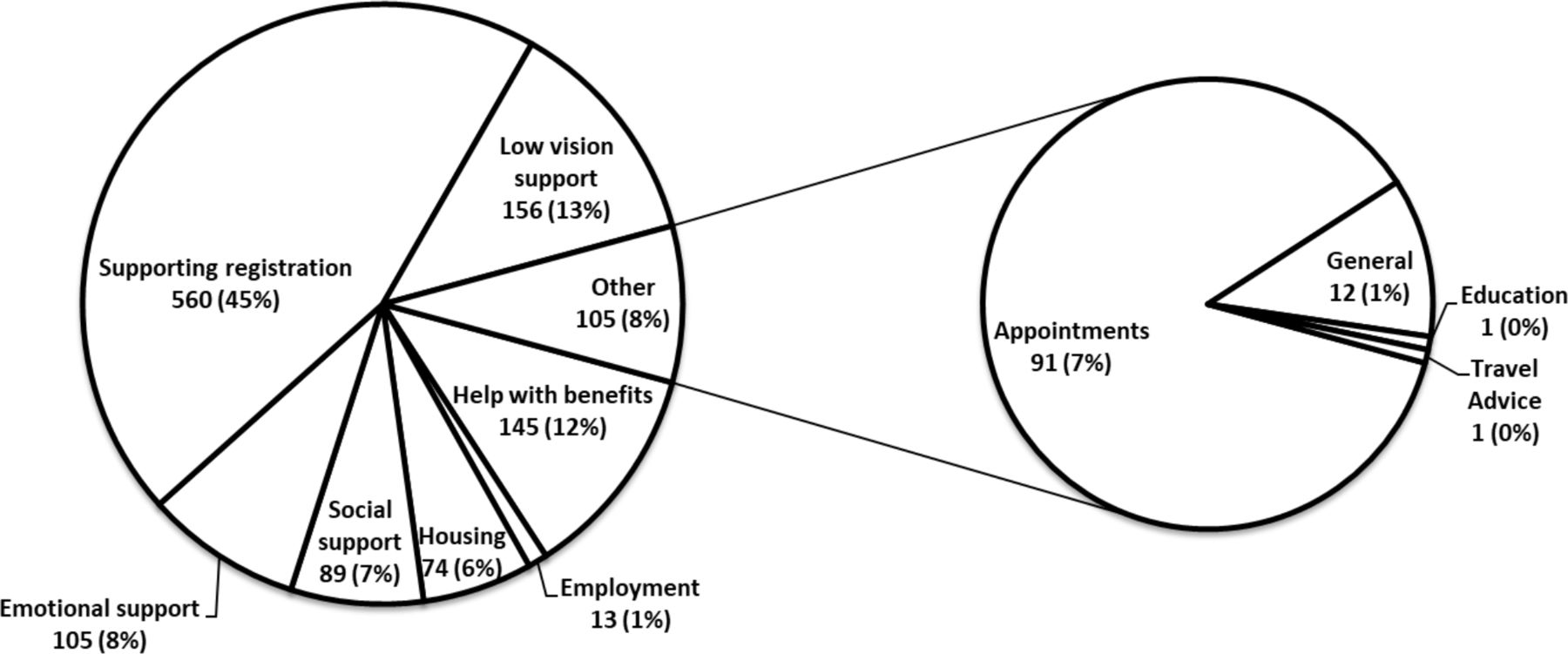
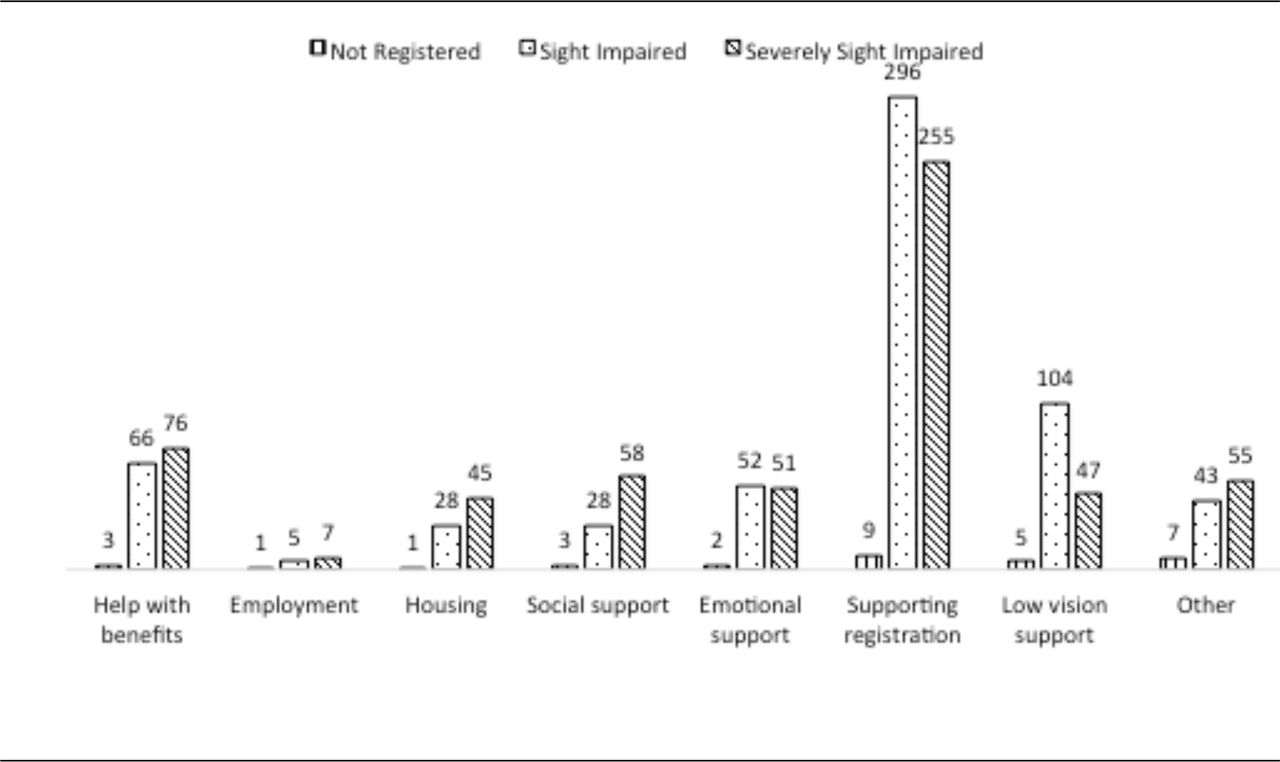
Figure 1 summarises the number of patients supported by the ECLO in the various domains (defined in table 1) and identifies supporting and facilitating the registration process as a key ECLO role. Figure 2 shows the distribution across the same domains of ECLO support based on CVI registration status. Patients who were not registered met the criteria for registration but declined registration, however, they still required support in other areas.

Support provided by ECLO (eye clinic liaison officer) in 2019 (n=1247).

{kind=link}
{kind=link}
Support distribution based on visual certification status (n=1247).
Definitions of categories of ECLO support
The χ2 test of independence showed a significant positive association between the number of domains of ECLO support and severe visual impairment, χ2 (14, N=1247)=52.7, p=2.16×10−6.
Three case vignettes have been included in order to further illustrate the input of the ECLO.
Case vignettes
Case 1
Ms A, registered sight impaired, was living in unsuitable accommodation, had financial difficulties, struggled to mobilise safely and was socially isolated. The ECLO addressed all of these issues by making a referral to the local housing department, providing advice on benefits and initiating an application for the personal independence payment benefit scheme. Furthermore, she referred Ms A for rehabilitation to ensure safe mobility, enrolled Ms A in a monthly social group and initiated grant applications for specialist equipment such as walking aids.
A further decline in vision resulted in the registration status being increased to severely sight impaired, and further support was provided by the ECLO.
Case 2
Mr B experienced severe visual loss of sudden onset and hence was referred to the ECLO to discuss registration. The ECLO felt that Mr B was very distressed, overwhelmed and unable to internalise the information given. Realising that Mr B needed time for reflection, the ECLO provided her contact details. Within 2 days, Mr B had contacted her, registration was completed, and additional services were offered. Referrals were made to various organisations for rehabilitation, a symbol cane, housing assessment and benefits advice. Furthermore, Mr B was referred to a weekly social group.
Case 3
During the COVID-19 pandemic, the ECLO provided telephone consultations for newly registered patients, and ongoing support and continuity of care for existing patients. Ms C, a sight-impaired patient, was concerned about a deterioration in her vision, and required an appointment, however, due to pandemic-related staffing issues, was unable to contact the clinical team. This was promptly addressed by the ECLO who arranged a consultation with the appropriate clinician.
Discussion
This study illustrates the significant impact of an ECLO on patient well-being and highlights the need for this crucial role within ophthalmology services.
The ECLO enabled patients to receive the holistic care that they required, by providing support in several different areas. Frequently provided support included streamlining the process for sight registration and thereby enabling access to social care services, benefits and low vision support services. The ability to delegate all of these important aspects of patient care to the ECLO, particularly with respect to facilitating and supporting the CVI registration process, serves to reduce clinician time per patient, thereby increasing productivity.
Not only did the ECLO provide support in several domains but also ensured that continuity of care was provided, as highlighted by the case vignettes. In case 1, ongoing support was provided when the patient experienced a further decline in vision. The importance of ensuring long-term access to support services for people with sight loss has been recognised, and individuals should be given many opportunities to review information about the help available as their needs change.14 Furthermore, ECLOs provide a point of contact to ensure that this support is continued after the patient is discharged from medical management.9
The third case highlights the importance of the ECLO during the COVID-19 pandemic. The WHO declared COVID-19 a global health emergency.15 16 Since face-to-face outpatient appointments were limited to urgent patients in order to reduce footfall in the ophthalmology department and, furthermore, many ophthalmology staff were redeployed, the role of the ECLO in providing telephone support for both newly registered and follow-up patients was crucial during this period.
The Royal National Institute of Blind People (RNIB) supports the ECLO role. This charity is responsible for ECLO training, continuing professional development and maintaining standards. A recent publication in association with the RNIB recognised and highlighted the importance of the ECLO role.9 Furthermore, in the 2013 publication on Age Related Macular Degeneration, the Royal College of Ophthalmologists identified the ECLO as an integral part of the team and specifically named the ECLO as a useful point of contact after the patient has received bad news about their vision.17 Despite such recognition of the importance of the ECLO role, the largest study on ECLO services in the UK to date found that service provision varies greatly across the region. In England, only 56 (37.3%) of the 150 busiest NHS Trusts have ECLO support and the remaining 62.6% do not.18
Strengths
This study is the first to assess the output of one ECLO over the period of a year and the number of patients supported. It has also highlighted the breadth of support provided by the ECLO in several domains of health and social care.
Limitations
The significant limitation of this study is that the data were collected retrospectively from the ECLO case notes and therefore is a secondary data analysis subject to inaccuracies. Furthermore, the case vignettes contain the subjective views of the ECLO regarding the feelings and emotions of the patient and their needs, as documented by the ECLO.
Conclusion
ECLOs are a core patient service within ophthalmology and have a significant impact on patients’ emotional and physical well-being and ultimately their quality of life. The ECLO role complements that of the clinical ophthalmology team, provides valuable additional capacity in the hospital setting and also much needed continuity of care as the needs of their patient group continue to change and evolve over time.
The study adds to the small current evidence base by gaining preliminary data at a local level. This is the first study to evaluate the impact of one ECLO on their patient population. Currently, ECLOs have not been fully incorporated into NHS care pathways across all hospitals, and the majority are reliant on RNIB and voluntary funding. The authors feel that the ECLO role should become an integrated part of every NHS ophthalmology service.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Footnotes
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors RB and MAB conceived the presented idea. VM and RB designed the study. VM and TT carried out the study and data collection. VM analysed the data and wrote the manuscript along with RB, in consultation with MAB. RB accepts full responsibility for the overall content as guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.