Article Text

Abstract
Objective To evaluate objective and subjective outcomes after bilateral implantation of two different multifocal intraocular lenses, which correct pseudophakic presbyopia in an adequate and homogeneous population court.
Methods and analysis Fifty patients were evaluated at 3 months after bilateral implantation, at the Eye Clinic of University of Verona and at the Carones Ophthalmology Center Milano, as follows: Tecnis Symfony (25 patients), Alcon PanOptix (25 patients). Main outcomes were uncorrected and best-corrected distance visual acuity (UDVA and BCVA) at 4 m, 60 cm (best distance corrected intermediate visual acuity (BDCIVA) and uncorrected intermediate visual acuity), 40 cm (best distance corrected near visual acuity (BDCNVA) and uncorrected near visual acuity (UNVA)), objective refractive outcome, defocus curve, contrast sensitivity (Modulation Transfer Function (MTF) cut-off), optical quality (Strehl ratio), aberrometry (root mean square RMS 4 mm), subjective quality of life (National Eye Institute Refractive Error Quality of Life score (NEI-RQL-42 score) test).
Results Symfony and PanOptix showed BCVA and UDVA comparable results. Symfony presented significant better outcomes at BDCIVA (p=0.001), while PanOptix showed better performances at BDCNVA and UNVA (p=0.01). Symfony achieved better results in RMS 4 mm (p=0.024) and in MTF cut-off (p=0.041). In the questionnaire NEI-RQL-42, PanOptix presented better scores in ‘near vision’ and ‘spectacles independence’, whereas Symfony in ‘symptoms’ and ‘clarity of vision’.
Conclusion Both intraocular lenses are valid options to avoid pseudophakic presbyopia, even though they present different features which make them unique. Symfony allows patients to achieve a better objective and subjective quality of vision and contrast sensitivity; PanOptix provides better outcomes in near vision and spectacles independence requirements.
- optics and refraction
- visual perception
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
In literature there is no consensus on Symfony and Pan0ptix performances in intermediate distance distance visual acuity anda quality of vision outcomes. Non-concordant data are due to the small and to different conditions in the quality of vision evaluation.
What are the new findings?
This prospective study is the first which gatered the largest and well-balanced cohort of patients, to shed the light on these two presbyopia-correcting intraocular lenses (IOLs), focusing on visual acuity at intermediate and near distances and on the quality of vision.
How might these results change the focus of research or clinical practice?
This study allows the surgeon and the patient to customise the surgical intervention choosing the specific implant compatible with patient's need, proving that Pan0ptix IOL would be an optimal choice for patients who wish to see optimally at near range, while Symfony IOL is suitable for those who need good intermediate vision.
Introduction
Multifocal intraocular lenses (MIOLs) were designed to improve spectacle independence, but this advantage was balanced with a low quality of vision at near and far distances due to the presence of contrast sensitivity (CS) function deterioration and subjective symptoms such as halos and glare.1–3 Currently, the majority of new generation MIOLs improve these defects and present a diffractive platform that splits lights to the retina, in order to obtain a good quality image at several distances and achieve a good spectacle independence.4 5 Nowadays, modern MIOLs obtain multifocality, thanks to two different diffractive technologies which are extended range of vision (ERV) that is used by Tecnis Symfony and Enlighten technology (Enlighten Optical Technology) that is exploited by PanOptix.6 7 Several studies have been carried out on these MIOLs, but the literature present discordant results on visual acuity at intermediate distances, defocus curve and on the quality of vision.8–12 The aim of the study is to compare these modern MIOLs (Tecnis Symfony ERV ZXR00 IOL and Acrysof IQ PanOptix TNFT00) in order to obtain objective and subjective analysis which provides clarity, thus helping the surgeon to choose the most appropriate IOL for the patient.
Materials and methods
Study design
This prospective observational comparative clinical study included patients after bilateral implantation of Tecnis Symfony or Acrysof IQ PanOptix for routine clinical practice. All patients were included at the Department of Neurosciences, Biomedicine and Movement Sciences, Eye Clinic, University of Verona, Verona, and at the Carones Ophthalmology Center, Milano, Italy. The calculation of the sample size was based on the primary outcomes of Best Corrected Distance Intermediate Visual Acuity (BCDIVA) at 60 cm under photopic condition and Best Corrected Distance Visual Acuity (BCDVA) at 40 cm.
The sample size of 50 subjects (25 for each group) reaches a power equal to 95% capable of detecting a difference between the averages of BCDIVA equal to 0.006 with SD 0.04 in the Symfony group and 0.07 in the PanOptix group with an alpha significance level of 0.05 using the T test for independent sample.8–12 The sample size was calculated with PASS V.14 software, in order to obtain a valid statistical analysis.9–11 13 14 Twenty-five consecutive patients were prospectively recruited the day after the implantation of the second eye with the Tecnis Symfony IOL (Symfony group) and 25 consecutive patients were prospectively enrolled the day after the implantation of the second eye with the Acrysoft IQ PanOptix IOL (PanOptix group), being careful to enrol patients who respected inclusion criteria and in order to create two homogeneous group for age and ocular parameters with a randomisation of 1:1. For routine clinical practice, each patient underwent surgery in the second eye 1 week after the first. All patients enrolled in the study were informed and written informed consent was obtained. The study adhered to the tenets of the Declaration of Helsinki and was notified to the local ethical committee (Department of Neuroscience, Biomedicine and Movement Sciences, University of Verona).
Only the investigators carrying out the follow-ups were masked to the implanted IOLs. Neither surgery treatment nor outcomes were masked.
Patient and public involvement statement
This study was done without patient or public involvement. Patients were not invited to discuss on the study design or interpret the results. Patients were not asked to contribute to the writing or editing of this paper.
Patients’ choice
Inclusion criteria for the study were patients with bilateral IOL implantation (Tecnis Symfony IOL, or Acrysoft IQ PanOptix IOL) with a pre-existing corneal astigmatism within 1.00 D and axial length between 22.0 mm and 24.5 mm before surgery. Exclusion criteria included patients with intraoperative complications, previous ocular surgery including corneal, retinal or refractive surgery, previous ocular trauma, and any ocular disease such as amblyopia, chronic or recurrent uveitis, acute ocular disease, diabetes mellitus with retinal changes, glaucoma, pseudoexfoliation syndrome or zonular laxity, optic nerve atrophy, keratoconus, alteration in colour perception and corneal endothelial dystrophy. All patients were evaluated at the baseline (1 day after the surgery), 1 week, 1 month and 3 months after the baseline, but all results reported refer to the 3-month follow-up visit.
Surgical technique
All included patients previously underwent a standard sutureless phacoemulsification surgery without any intraoperative complications. The surgery was performed by two experienced surgeons (EP, FC). In all cases, topical anaesthesia was administered and pharmacological mydriasis was induced using a combination of cyclopentolate 1.0% and phenylephrine 0.1%. IOL power and predicted postoperative refraction were calculated with a Lenstar Optical Biometer (Haag-Streit, USA), using SRK/T biometry for all eyes (between 22.00 mm and 24.5 mm). IOL dioptric power was selected targeting emmetropia, using the IOL power corresponding to 0 or to the negative (myopic) predicted refractive outcome closest to 0. At baseline all patients received the same postoperative medication, which was a combination of topical netilmicin 0.3% and dexamethasone 0.1% four times a day for 2 weeks and then tapered off by one drop per week. Likewise, non-steroidal anti-inflammatory diclofenac 0.1% drops were prescribed three times a day for 4 weeks to prevent macular oedema.
Intraocular lens (IOL)
Tecnis Symfony ZXR00 is an ERV IOL that is distributed by Johnson & Johnson (Johnson & Johnson, New Brunswick, New Jersey, USA). It is a UV blocking hydrophobic acrylic, single piece IOL, aspheric in the anterior surface and achromatic diffractive in the posterior one. Unlike diffractive MIOLs which split the light in different discrete foci, Symfony technology elongates the depth of focus, thanks to echelette design, and it is characterised by a typical continuum range of foci that induces a defocus curve with a single large peak. Moreover, Symfony technology includes a compensation for positive corneal spherical aberration which allows to achieve a better quality of vision. In this IOL it has been calculated that light transmission to the retina reaches 92%.6
Acrysof IQ PanOptix TNFT00 is a tri-quadrifocal IOL that is distributed by Alcon (Alcon Laboratories, Inc, Fort Worth, Texas, USA). It is a hydrophobic acrylic, single piece, aspheric non-apodised diffractive IOL. PanOptix design presents four focal points (40 cm, 60 cm, 120 cm and infinity) even if this quadrifocal technology is modified, so the light energy for intermediate focal point (120 cm) is redistributed to the infinity focal point, in order to obtain better performances in the distance (Enlighten Optical Technology). For this reason, patients with PanOptix IOLs could only use three focal points: at distance, at 60 cm and at 40 cm. Light entering the eye is distributed 50% for far distance focus, 25% for near distance focus and 25% for intermediate distance focus, with a total transmission of 88% of light to the retina with a pupil diameter of 3.0 mm.7
Outcomes
Monocular visual acuity, corrected for distance and uncorrected were measured using the corresponding Early Treatment Diabetic Retinopathy Study (ETDRS) chart under photopic conditions (683 lm/W) and 100% contrast (ESV-3000 ETDRS System, Vectorvision, Inc) at 4 m.
To obtain the defocus curve, binocular visual performances were tested under photopic conditions (683 lm/W) and 100% contrast (ESV-3000 ETDRS System, Vectorvision, Inc) at 4 m. Each patient was corrected for distance acuity in both eyes and additional lenses were added sequenced over the range of +1.00 to −4.00 D in 0.50 D steps, recording visual acuity for each step. In order to avoid memory effects presenting letter sequences were randomised and patient’s eyes were occluded between each lens presentation, so that the subject was not aware of which lens had been inserted and whether the letter on the chart had been changed or not.8
Intermediate and near visual acuity were measured monocular, respectively, at 60 cm and 40 cm using ETDRS near acuity charts (Sloan ETDRS format near vision, precision vision) with 100% contrast and photopic condition (683 lm/W).
Objective quality of vision was measured with objective CS (MTF cut-off) and objective optical quality (Strehl ratio), calculated with Optical Quality Analysis System (OQAS, Visiometrics SL, Terassa, Spain).
Aberrometry (root mean square, RMS 4 mm) was calculated with Hartmann-Shack aberrometer (Topcon, Tokyo, Japan).
Last, the subjective quality of vision was evaluated using the National Eye Institute Refractive Error Quality of Life score test (NEI-RQL-42 score), and in particular we focused our attention on subscales of ‘clarity of vision’, ‘near vision’, ‘dependence on correction’ and ‘symptoms’.
Statistical analysis
Data analysis was performed using SPSS for Windows software (V.19.0, IBM Corporation, Armonk, New York, USA). Normality of data samples was evaluated using the Kolmogorov-Smirnov test. When parametric analysis was possible, the Student’s test for unpaired data was used for comparison between IOLs, whereas the Mann-Whitney test was used when parametric analysis was not possible. A p value <0.05 was considered statistically significant.
Results
The study comprised 50 patients (100 eyes) of whom 25 patients had Symfony IOLs and 25 patients had PanOptix IOLs implanted. There were no preoperative statistically significant differences between the two groups in terms of age, corneal keratometry and pupil diameter (photopic and scotopic conditions, table 1). No patient was lost during follow-up period, there were no postoperative complications or adverse effect.
Preoperative patient’s characteristics in the two IOL groups
Visual acuity
Symfony and PanOptix groups showed comparable results in objective refraction: postoperative SE was −0.02 (±0.48) D in the Symfony group and –0.1 (±0.42) D in the PanOptix group, without any statistically significant difference between the two groups. Mean uncorrected distance visual acuity (UDVA) measured at 4 m was 0.00 (±0.09) logMar for the Symfony group and −0.02 (±0.09) logMar for the PanOptix group. Mean best distance corrected visual acuity (BDCVA) measured at 4 m was −0.09 (±0.05) logMar for the Symfony group and −0.08 (±0.06) logMar for the PanOptix group. No statistically significant difference in mean values was found between groups both concerning UDVA (p=0.272) and BDCVA (p=0.489, table 2).
Visual acuity at several distances at 3 months after bilateral implantation
Mean monocular uncorrected intermediate visual acuity (UIVA) measured at 60 cm was 0.10 (±0.03) logMar for the Symfony group and 0.12 (±0.04) logMar for the PanOptix group. Mean best distance corrected intermediate visual acuity (BDCIVA) measured at 60 cm was 0.07 (±0.03) logMar for the Symfony group and 0.10 (±0.03) logMar for the PanOptix group. No statistically significant difference in mean values was found between groups both concerning UIVA (p=0.058), however the difference in BDCIVA achieved statistical significance (p=0.001) with the better outcome in favour of the Symfony group.
Mean monocular uncorrected near visual acuity (UNVA) and mean monocular best distance corrected near visual acuity (BDCNVA) measured at 40 cm were, respectively, 0.26 (±0.08) logMar and 0.26 (±0.05) logMar for the Symfony group, whereas 0.14 (±0.045) logMar and 0.14 (±0.04) logMar for the PanOptix group. The difference both in mean UNVA and mean BDCNVA between groups achieved statistical significance (respectively p=0.001 and p=0.001) with the better outcome in favour of the PanOptix group.
Defocus curve
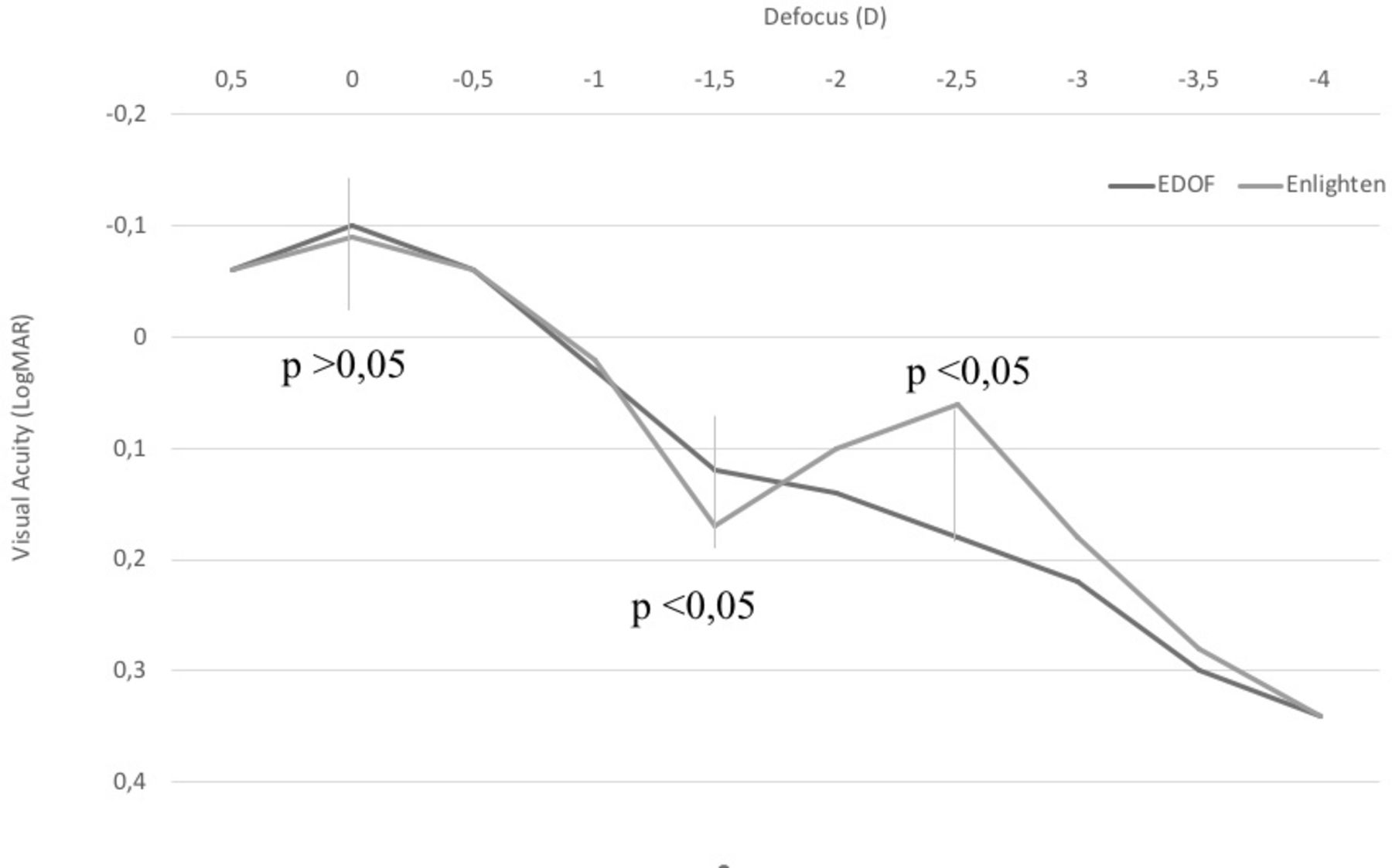
Both groups showed a reduction in visual acuity as negative defocus increased. Both groups showed similar mean BDCVA without statistically significant differences (p=0.489). The Symfony IOL showed a ‘softer’ decrease in visual acuity as negative defocus increased when compared with the PanOptix group that showed a ‘bifocal’ defocus profile (figure 1). The difference in mean BDCVA acquired statistical significance at −1.50 D defocus threshold (p=0.006) with better outcomes in Symfony group and an opposite condition is pointed out at −2.50 D defocus threshold (p=0.001).

{kind=link}
Defocus curve. The defocus curve, according to visual acuity at several distances, presented significant differences at −1.50 D and at −2.50 D.
Objective quality of vision and CS
To assess objective quality of vision Strehl ratio, internal RMS and MTF cut-off at pupil size of 4 mm have been used (table 3).
Objective postoperative quality of vision
Mean Strehl ratio was 0.17 (±0.05) for the Symfony group and 0.15 (±0.08) for the PanOptix group. No statistically significant differences were found between groups (p=0.258). Mean internal RMS at 4 mm was 0.15 (±0.06) for the Symfony group and 0.18 (±0.06) for the PanOptix group, with a statistically significant difference between the two groups (p=0.024). CS was assessed by means of mean MTF cut-off evaluation: the Symfony group mean MTF cut-off was 34.25 (±11.8) c/deg, whereas PanOptix group had a mean MTF cut-off of 27.41 (±0.06) c/deg. Statistically significant difference was present between groups (p=0.041) with Symfony IOLs having the better results.
Subjective quality of vision
Subjective quality of vision was calculated from the NEI-RQL-42 score. Main outcome endpoints were the items ‘clarity of vision’, ‘near vision’, ‘dependence on correction’ and ‘symptoms’ (table 4).
Subjective quality of vision by means of NEI-RQL-42 score
Clarity of vision mean score for Symfony IOLs was 92.01 (±10.41), whereas PanOptix IOL achieved 88.75 (±18.53). Near vision mean score was 86.11 (±15.89) for Symfony IOLs and 90.81 (±16.00) for PanOptix IOLs. Dependence on correction mean score for Symfony IOLs was 62.96 (±35.37), while PanOptix IOLs scored 95.00 (±9.21). Symptoms’ score was 79.73 (±19.99) for Symfony IOLs and 75.75 (±16.09) for PanOptix IOLs. No statistically significant differences were reported between mean scores for the two groups of patients concerning any of these evaluation parameters.
Discussion
Many patients undergoing cataract surgery demand a spectacles independence in daily activities. In the ‘refractive cataract era’ a customised surgical intervention is suggested and many diffractive MIOLs are now available in order to solve pseudophakic presbyopia. In this paper both modern MIOLs (Symfony and PanOptix) have been studied with the largest and balanced cohort of patients, comparing them with a comprehensive analysis of objective and subjective parameters at 3 months outlining all different outcomes secondary to Symfony and PanOptix MIOLs implantations permitting the surgeon to lead a customised and aware choice. According to literature,9–12 no statistically significant difference was recorded between two groups when taking into account 4 m uncorrected and best-corrected distance visual acuity, with both groups achieving good results in terms of visual acuity and of postoperative spherical equivalent (SE), and better results in UNVA and BDCNVA were found in favour of PanOptix group. In literature there is no consensus in outcome results at intermediate and quality of vision; the aim of this paper is to clarify the IOLs’ behaviour with a comprehensive study having numerous and balanced sample of patients.
As for the intermediate vision at 60 cm some authors agree with this study finding better results for Symfony IOL,10–12 but not all of these authors find statistical significance between the groups, probably for the small and inhomogeneous sample of patients. In this paper that presents the most numerous, homogeneous and appropriate sample of population, patients implanted bilaterally with Symfony have a significantly better BDCIVA.
Monaco et al in 2017, found better results in the intermediate vision (both BDCIVA and UIVA) for PanOptix IOL, with statistical significance in UIVA.13 This finding disagrees with the existing literature and it is important to emphasise that author performed the intermediate visual acuity at 67 cm, which corresponds to the PanOptix intermediate focus. The remaining literature performed this evaluation at 60 cm, which is the distance universally used for the evaluation of the intermediate visual acuity.
Knowledge of the behaviour of MIOL is essential to choose the specific implant compatible with patient’s needs: PanOptix IOL would be an optimal choice for patients who wish to see optimally at near range, while Symfony IOL is suitable for those who need good intermediate vision such as those who often use electronic devices such as computers, smartphones and tablets. The study of the defocus curve confirms the behaviour of these MIOLs and their main indications. Regarding the quality of vision (objective and subjective) both lenses achieve high levels of image quality with minimal disturbances. Comparing two groups, the Symfony IOL emerged as the best CS (cut-off MTF) and aberrometry (internal RMS 4 mm). Most of the existing literature reported no difference in CS and quality of vision using both objective and subjective evaluation methods,9 10 13 in particular Mencucci and Andrè Lins De Medeiros found significantly better results in CS for Symfony IOL.11 14 In this study, having the largest and most homogeneous population sample, an objective assessment of CS was used and the MTF cut-off and RMS were found to be statistically better for the Symfony IOL. Furthermore, it has already been shown that Symfony IOL performs CS in a way comparable to the monofocal.15 Discordant results were also found by Monaco et al in RMS at 5 mm, where quality of vision was higher for the PanOptix group.13 However, the author used a dynamic schiascopy difficult to compare with a Hartmann-Shack system and moreover he considered a 5 mm diameter instead of 4 mm of our sample. The objective outcomes were also confirmed in the NEI-RQL-42 scores where ‘clarity of vision’ and ‘Symptoms’ showed differences (although not statistically significant) in favour of the Symfony IOL group. Nevertheless, the superiority of Symfony IOLs in quality of vision does not guarantee the same results in ‘dependence of correction’ and ‘near vision’, where PanOptix IOLs achieved better subjective scores. To conclude, this study proves that every IOL has its different field of application that needs to be matched with each patient’s expectations and lifestyle to achieve the best satisfaction. A study with an adequate and homogeneous population court is essential to clarify the functioning of these IOLs.
Footnotes
Contributors All authors read and approved the final manuscript. PT, EB, FS, AG, AB contributed to the acquisition, analysis and interpretation of the data. FS and PT performed the statistical analysis. PT, EB, AG wrote the manuscript. GM, EP, FC and ADG designed the project, revised the work and made the final approval.
Funding This study was funded by Università degli Studi di Verona.
Competing interests FC is a consultant at Johnson & Johnson and Alcon Laboratories, Inc.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.