Article Text

Abstract
Objective To investigate the incidence, clinicopathological characteristics and survival of ocular adnexal lymphoma (OAL) in the paediatric population.
Methods and analysis In this retrospective case series, the Surveillance, Epidemiology and End Results database was accessed to identify individuals with OAL ≤18 years of age, diagnosed between 1973 and 2015. OAL located in the eyelid, conjunctiva, lacrimal apparatus and orbit were included. Main outcome measures were the age-adjusted incidence rates (IRs) per 1 000 000 population at risk (calculated for the period 2000–2015) and descriptive statistics of demographic and clinicopathological features.
Results The IR of paediatric OAL was 0.12 (95% CI 0.08 to 0.16) per 1 000 000. Males (0.15; 95% CI 0.10 to 0.22) and blacks (0.24; 95% CI 0.13 to 0.42) had a higher tendency for OAL development. A total of 55 tumours in 54 children were identified. The majority were localised (78.4%), conjunctival (49.1%) lymphomas. Extranodal marginal zone lymphoma (EMZL, 45.5%, n=25) was the most frequent subtype, followed by diffuse large B-cell lymphoma (DLBCL, 9.1%, n=5), B lymphoblastic lymphoma (7.3%, n=4), follicular lymphoma (5.5%, n=3), Burkitt lymphoma (5.5%, n=3), anaplastic large cell lymphoma (ALCL, 3.6%, n=2), small lymphocytic lymphoma (1.8%, n=1), diffuse large B-cell lymphoma, immunoblastic (1.8%, n=1) and panniculitis-like T-cell lymphoma (1.8%, n=1). Localised, low-grade, conjunctival lymphomas were frequently treated with complete excision with or without radiation, while high-grade and distant tumours usually received chemotherapy. Only 29.1% of paediatric OAL cases were treated with radiation. Three out of five (60%) patients with DLBCL died of lymphoma at a median follow-up of 21 (range 10–86) months, and 1 out of 2 (50%) patients with ALCL died of lymphoma at 23 months from diagnosis.
Conclusion OAL in the paediatric population is rare. The majority of OAL are EMZL and are characterised by excellent prognosis. The histological subtype was found to be the main predictor of outcome with cancer-specific deaths observed in patients with DLBCL and ALCL.
- eye (globe)
- neoplasia
- pathology
- child health (paediatrics)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Ocular adnexal lymphoma is typically a disease of the elderly.
Data on the incidence, clinicopathological features and survival of ocular adnexal lymphoma in the paediatric population are limited.
What are the new findings?
Paediatric ocular adnexal lymphoma is a rare disease.
Extranodal marginal zone lymphoma consists the majority of cases.
Only a small percentage of cases in our cohort were treated with radiation.
Similar to adults, the histological subtype was identified as the major outcome predictor, with deaths observed in patients with diffuse large B-cell and anaplastic large cell lymphomas.
How might these results change the focus of research or clinical practice?
This is the first comprehensive analysis on paediatric ocular adnexal lymphoma.
Our findings can be a reference point for clinicians who encounter these cases, as well as for future multicentre investigations.
Introduction
Non-Hodgkin’s lymphoma (NHL) comprises a diverse spectrum of lymphoproliferative diseases and represents 4%–5% of new cancer cases each year.1 Primary NHL of the ocular region represents 1%–2% of all NHL and 5%–15% of all extranodal sites.2 3 It can be intraocular (vitreoretinal or uveal lymphoma), but most commonly develops in the ocular adnexal structures, including the eyelid, conjunctiva, lacrimal apparatus, and orbit.
Ocular adnexal lymphoma (OAL) predominantly affects the elderly, with a reported annual incidence rate of 2 per 100 000 in persons above 70 years of age.4 Most commonly, it is a low-grade lymphoproliferation, characterised by a prolonged, indolent course. Presenting symptoms can include proptosis, periorbital oedema, conjunctival ‘salmon patch’, visual changes and rarely pain from increased intraocular pressure.5–7 In children and adolescents, OAL is exceedingly rare and incidence is unknown.8
Current understanding of OAL epidemiology and outcomes in the paediatric population is predominantly based on case reports and data from series pertaining to the adult lymphoma literature.9–25 We hypothesise that significant differences exist between paediatric and adult OAL that have not yet been described. This study aims to investigate the incidence, as well as clinical, histological and survival characteristics of paediatric patients with OAL using data from a national population-based cancer registry. Similar to recent multicentre studies on OAL, a subtype-focused analysis was performed, in order to highlight clinical and survival features that are subtype-specific.5–7
Materials and methods
Data source
The cohort of patients was abstracted from the National Cancer Institute’s Surveillance, Epidemiology and End Results (SEER) database, incorporating data derived from 18 cancer registries and covering approximately 28% of the total US population based on the 2010 US census.26 The SEER 18 registries include: San Francisco, San Jose-Monterey, Los Angeles, the Greater California area, Atlanta (Metropolitan), rural Georgia, the Greater Georgia area, Connecticut, Detroit/Michigan, Hawaii, Iowa, New Mexico, Seattle-Puget Sound/Washington, Utah, Alaska, Kentucky, Louisiana and New Jersey.
Coding and study cohorts
The following inclusion criteria were applied: (i) tumour classified as NHL according to the International Classification of Diseases for Oncology, third edition (ICD-O-3), using morphology codes: 9590–9596, 9670–9726, 9728–9729, 9811–9837,27 (ii) tumour located in the eyelid, conjunctiva, lacrimal apparatus and orbit using ICD-O-3 topographic codes: C44.1, C69.0-C69.1, C69.3, C69.5-C69.827 and (iii) patient age ≤18 years. Exclusion criteria were: (i) tumour not histologically or cytologically confirmed and (ii) cases diagnosed from autopsy or death certificates.
Data extraction
Demographic, clinicopathological features and survival data were extracted using the SEER ‘case listing’ module. Tumour stage was recoded based on the SEER summary stage for OAL as follows: (1) localised, defined as lymphoma limited to ocular adnexa; (2) regional, defined as lymphoma extending to adjacent structures such as bone and brain and/or regional node (preauricular, submandibular, cervical) involvement and (3) distant, defined as non-contiguous involvement of other extranodal sites (parotid gland, submandibular gland, lung, liver, spleen, kidney, breast, etc) and/or diffuse or disseminated involvement of peripheral and central lymph node regions.28 The American Joint Committee on Cancer (AJCC) Collaborative Stage and AJCC tumour-node-metastasis (TNM) stage, seventh edition, were also reported for tumours diagnosed in 2004 or later and 2010 or later, respectively.29 30 Data regarding treatment selection (surgery, radiation and chemotherapy) were also obtained. Surgery was documented as complete excision, debulking procedure or enucleation.
Statistical analysis
For population analysis, incidence rates were determined in a two-step process using the SEER*Stat software. First, age-specific rates were calculated using census estimates for the population and the 42-year period of time studied (therefore adjusting for population increases). Consequently, age-specific rates were standardised to the age distribution of the US population as reported in the 2000 US census and expressed as per 1 000 000 population at risk. This step corrected for changes and variations in age distribution over time. We calculated IRs from 2000 to 2015 for two reasons: first, we aimed to include the largest cohort of patients, since only 9 registries had been included for the period 1973–2015, while all 18 SEER registries had been added after 2000; second we wanted to account for the misdiagnosis of OAL as reactive lymphoid hyperplasia prior to the routine utilisation of immunohistochemical techniques.31
In the cohort analysis, Stata V.15 (StataCorp) and Prism V.8 (GraphPad Software) were used for descriptive and survival statistics. Non-specified histology (9590/3: malignant lymphoma, NOS and 9591/3: non-Hodgkin’s lymphoma
, NOS) were listed as unknown. Categorical variables are presented as absolute number and percentages, and continuous outcomes as median and range. Kaplan-Meier curves were used to determine survival over time. Univariate survival analysis was executed using the log-rank test. For pairwise comparisons of multiple groups, post hoc analysis with Bonferroni correction was applied. The α level of significance was set at 0.05 and p values were two-sided.
Results
Population analysis
The age-adjusted incidence of primary paediatric OAL was 0.12 (95% CI 0.08 to 0.16) per 1 000 000 children aged 0–18 years (table 1). Paediatric males and blacks demonstrated a higher tendency for OAL development, although the results were not statistically significant: males 0.15 (95% CI 0.10 to 0.22), females 0.08 (95% CI 0.04 to 0.13), blacks 0.24 (95% CI 0.13 to 0.42), whites 0.10 (95% CI 0.06 to 0.14), Hispanics 0.10 (95% CI 0.05 to 0.18) and Asians 0.03 (95% CI 0.00 to 0.17).
Incidence rates (IRs) of paediatric ocular adnexal lymphoma in the US population for the period 2000–2015
Ocular adnexal lymphoma cohort analysis
Fifty-five primary OAL tumours in 54 children were identified. One patient was diagnosed with two primary ocular lymphomas (different histology), one of which was bilateral. No other preceding or subsequent malignancies were observed in our cohort. The median age at diagnosis was 13 (range 1–18) years and the median follow-up duration was 81 (range 0–418) months. A total of 36 (66.7%) patients were male. Twenty-five (46.3%) patients were white, 15 (27.8%) were black, 11 (20.4%) were Hispanic and 2 (3.7%) were Asian. Six (10.9%) tumours were bilateral. Overall, the conjunctiva was the most common primary site (conjunctiva 49.1%, orbit 38.2%, lacrimal gland 9.1%, eyelid 3.6%), and the majority of cases were diagnosed at an early SEER stage (72.7% were localised).
The following mature B-cell lymphoma subtypes were identified: 25 (45.5%) extranodal marginal zone lymphoma (EMZL) cases, 5 (9.1%) diffuse large B-cell lymphoma (DLBCL) cases, 3 (5.5%) follicular lymphoma (FL) cases, 3 (5.5%) Burkitt lymphoma (BL) cases, 1 (1.8%) small lymphocytic lymphoma case and 1 (1.8%) diffuse large B-cell lymphoma, immunoblastic (DLBCLI) case. The following mature T-cell lymphoma subtypes were identified: 2 (3.6%) anaplastic large T/null-cell lymphoma (ALCL) cases and 1 (1.8%) panniculitis-like T-cell lymphoma case. Finally, 4 (7.3%) B-cell lymphoblastic lymphomas were identified, one of which was Philadelphia translocation-positive. Of the 10 OALs with unknown histological subtype, one was of B-cell origin and one of NK-cell origin, but no further classification could be made. Table 2 summarises the clinicopathological characteristics of paediatric OAL by histological subtype.
Clinicopathological characteristics of paediatric ocular adnexal lymphoma by tumour histological subtype
B-cell lymphoma subtypes
Extranodal marginal zone lymphoma
Twenty-five (45.5%) patients were diagnosed with EMZL. The median age was 15 years (range 5–18), and 20 (80.0%) were male. Eight (33.3%) patients were white, 9 (37.5%) black, 6 (25.0%) Hispanic and 1 (4.2%) Asian. Twenty-two (88.0%) were located in the conjunctiva and 22 (91.7%) were localised at diagnosis. Five tumours (20.8%) were bilateral. Of the 20 patients with localised conjunctival tumours, 9 (45.0%) were treated with complete excision alone, 7 (35.0%) with excision and radiation, 1 (5.0%) with radiation only and 1 (5.0%) with chemotherapy only (table 3). Two patients with localised orbital tumours were treated with complete excision and excision plus radiation, respectively. Surgery combined with radiation was also used for a patient with conjunctival primary OAL and distant disease, while a patient with orbital EMZL and metastases was treated with chemotherapy. The median follow-up was 70 months (range, 7–213), and during this time, no deaths were observed.
Management of paediatric ocular adnexal lymphoma by tumour location, histological subtype and stage
Diffuse large B-cell lymphoma
Five (9.1%) patients were diagnosed with DLBCL. The median age was 15 years (range 2–17). Three patients (60.0%) were male, four (80.0%) were white and one (20.0%) was black. Three cases (60.0%) originated in the orbit, one (20.0%) in the conjunctiva and one (20.0%) in the lacrimal gland, and all tumours were unilateral. Stage was localised for two patients (66.7%) and distant for one patient (33.3%). All patients received chemotherapy regardless of tumour location, except for the patient with the lacrimal tumour, for whom treatment was documented as none/unknown (table 3). Three patients (60.0%) died of lymphoma at 10, 21 and 86 months from diagnosis, and two (40.0%) were alive at their last visit 92 and 154 months from diagnosis.
Lymphoblastic B-cell lymphoma
Four (7.3%) patients were diagnosed with precursor B-cell lymphoblastic lymphoma, one of whom displayed Philadelphia translocation. The median age was 5 (3–7) years. All patients were white females and were diagnosed with unilateral orbital tumours. Two of the three patients with Philadelphia-negative B-LBL had localised disease. One of them received chemotherapy and the other chemotherapy plus ‘debulking’ surgery (table 3). The third patient with Philadelphia-negative B-LBL was diagnosed with metastatic disease and was treated with chemotherapy. The patient with Philadelphia-positive B-LBL had distant disease at diagnosis and was treated with chemotherapy. All patients were alive at a median follow-up of 91.5 (range 46–178) months.
Follicular lymphoma
Three (5.5%) patients were diagnosed with FL. The median age at diagnosis was 13 (range 10–15) and all patients were male. One patient (33.3%) was white and two (66.7%) patients were black. A patient with bilateral, localised conjunctival FL was treated with surgery alone (table 3). Since this patient was diagnosed in 2015, no follow-up visits are documented. A patient with distant eyelid lymphoma was treated with chemotherapy. The third patient was diagnosed with a localised, left lacrimal gland FL and a localised, bilateral, conjunctival EMZL. No cancer-directed surgery or radiation was performed for the FL, but it is unknown if the patient received chemotherapy. Both patients with documented follow-up were alive 80 and 130 months from diagnosis.
Burkitt lymphoma
Three (5.5%) patients were diagnosed with BL. The median age was 11 (range 1–11) and all patients were male. Two (66.7%) were whites and one (33.3%) was of Hispanic origin. Two patients with unilateral orbital BLs and metastases were treated with chemotherapy (table 3). A patient with unilateral, localised, lacrimal gland BL was treated with tumour excision plus chemotherapy. All patients were alive at 195, 156 and 157 month follow-up from diagnosis, respectively.
Small lymphocytic lymphoma
A boy aged 17 years was diagnosed with localised SLL of the right orbit, which was treated with radiation (table 3). Sixty-nine months after diagnosis he died of ‘accidents and adverse effects’.
Diffuse large B-cell lymphoma, immunoblastic
A girl aged 8 years was diagnosed with localised DLBCLI of the left orbit, and received a combination of surgery, radiation and chemotherapy (table 3). She was alive 311 months after diagnosis.
T-cell lymphoma subtypes
Anaplastic large T/null-cell lymphoma
A white boy aged 17 years was diagnosed with regional ALCL, anaplastic lymphoma kinase-positive (ALK+) of the right orbit. An excisional biopsy was performed accompanied by radiation and chemotherapy (table 3). The patient died of lymphoma 23 months after diagnosis. A white girl aged 15 years was diagnosed with distant ALCL, ALK+ of the left orbit. The patient was treated with enucleation and chemotherapy but died 3 months after diagnosis due to ‘cerebrovascular diseases’.
Panniculitis-like T-cell lymphoma
A white girl aged 9 years was diagnosed with localised PTCL of the right orbit. The patient underwent complete excision and chemotherapy (table 3) and was alive 32 months from diagnosis.
Survival analysis
For the whole paediatric cohort, the 5-year overall (OS) and cancer-specific (CS) survival was 92.1% (95% CI 80.3% to 97.0%) and 93.9% (95% CI 82.2% to 98.0%), respectively (figure 1A). Final OS and CS was 86.1% (95% CI 71.1% to 93.7%) and 90.4% (95% CI 75.6% to 96.4%), respectively (figure 1A). Six (11.1%) children died at a median follow-up of 22 (range 3–86) months. Three children with DLBCL died of lymphoma at a median follow-up of 21 (range 10–86) months and a patient with ALCL, ALK+ died of lymphoma at 23 months from diagnosis. DLBCL histology (Bonferroni-corrected p<0.001 OS and CS, log-rank test; figure 1B), ALCL histology (Bonferroni-corrected p<0.001 for OS and CS, log-rank test; figure 1B), orbital involvement (p=0.02 for OS and p=0.07 for CS, log-rank test; figure 1C) and advanced stage (p=0.06 for OS and p=0.03 for CS, log-rank test; figure 1D) were significantly associated with higher mortality.
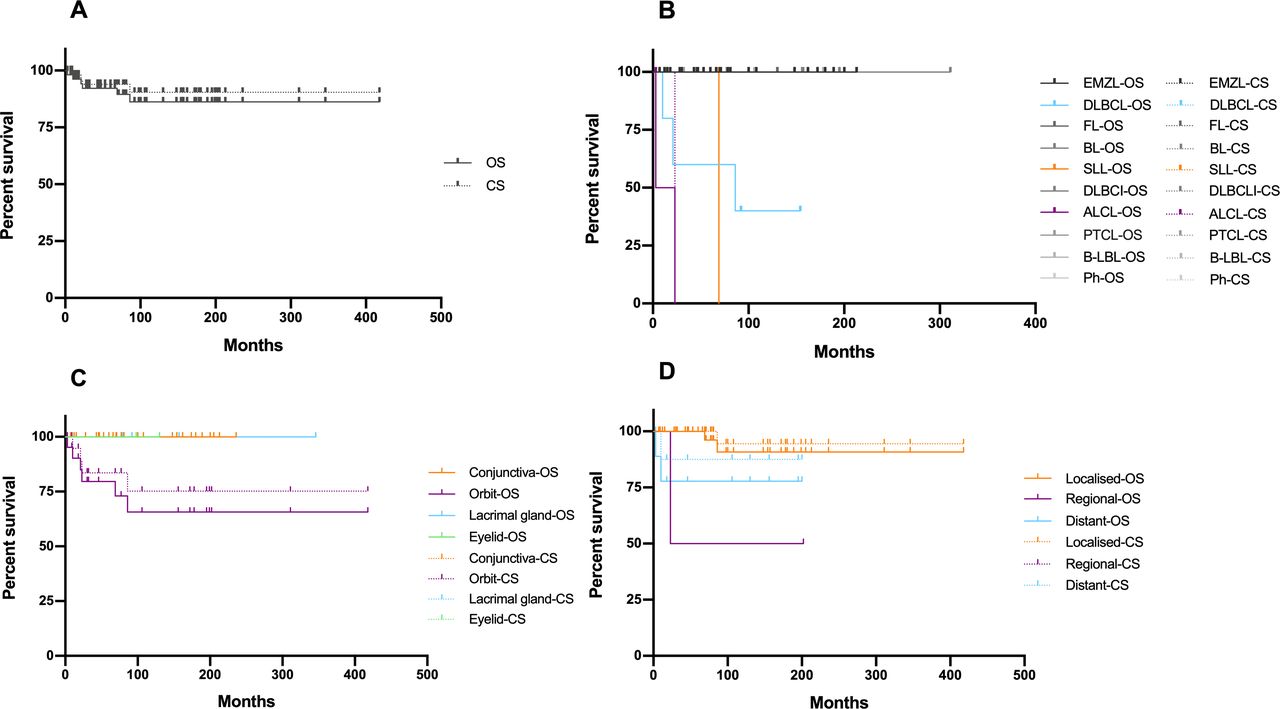
OS and CS of children with ocular adnexal lymphoma (A) as a whole, and stratified by (B) tumour histological subtype, (C) tumour location and (D) tumour stage. CS, cancer-specific; OS, overall survival; ALCL, anaplastic large T/null-cell lymphoma; B-LBL, lymphoblastic B-cell lymphoma; BL, Burkitt lymphoma; DLBCL, diffuse large B-cell lymphoma; DLBCLI, diffuse large B-cell lymphoma, immunoblastic;EMZL, extranodal marginal zone lymphoma; FL, follicular lymphoma; Ph, lymphoma with Philadelphia translocation; PTCL, panniculitis-like T-cell lymphoma; SLL, small lymphocytic lymphoma.
Discussion
This study represents a population-based description of primary OAL in the paediatric population in the USA, using data available from the SEER registry. The histological spectrum was broad with EMZL accounting for nearly half of paediatric OAL cases.4–7 32–35 While still rare, the percentages of BL and T-cell lymphomas were higher compared with adult OAL cohorts, whereas FL was less commonly observed.5–7 36 None of the T-cell lymphomas originated on the eyelids, which is the highest-risk area for T-cell OAL development.6
While lymphoblastic lymphoma generally develops from immature T-cells, lymphoblastic OAL in children was of B-cell origin in all specified cases. Our findings are in line with the large cohorts in the literature showing that B-LBL of the ocular adnexa is primarily a disease of children and young adults. In a study by Jenkins et al, all four lymphoblastic lymphomas in a cohort of 192 patients with ocular adnexal lymphoma were diagnosed in children, three of which demonstrated a B-cell phenotype.34 Similarly, in a multicentre study by Olsen et al, three out of four B-LBLs in a cohort of 797 patients with orbital lymphoma were diagnosed in children aged 12 years or less.7 In a study by Sjö et al, two out of three B-LBLs in a cohort of 228 ophthalmic lymphomas were seen in children,4 while in a cohort of 353 OALs, the one lymphoblastic lymphoma diagnosed in a child was a precursor B lymphoblastic lymphoma.32
The conjunctiva was by far the most common location of paediatric EMZL, as opposed to adults, where the orbit is the most frequently involved anatomical structure.4 32 33 35 37 It is possible that orbital tumours may have been underdiagnosed in the paediatric age group, due to the less frequent use of neuro-imaging techniques in children, which require anaesthesia. However, aggressive histological subtypes, such as DLBCL, BL, T-cell lymphomas and B-LBLs, demonstrated a predilection for the orbit. While the conjunctiva was most frequently affected, it is important to note that most conjunctival lesions in children are benign. In a large series reporting on conjunctival tumours observed in 262 children, only 3% were malignant and only 1.5% represented a lymphoid proliferation.38
In contrast to adult OAL, which is characterised by equal gender distribution or a slight female predominance,32 39 40 males in the paediatric population demonstrated higher risk for OAL development. Moreover, while in the USA the risk of OAL is higher in the white population,41 black children in our study exhibited a higher tendency towards OAL development.
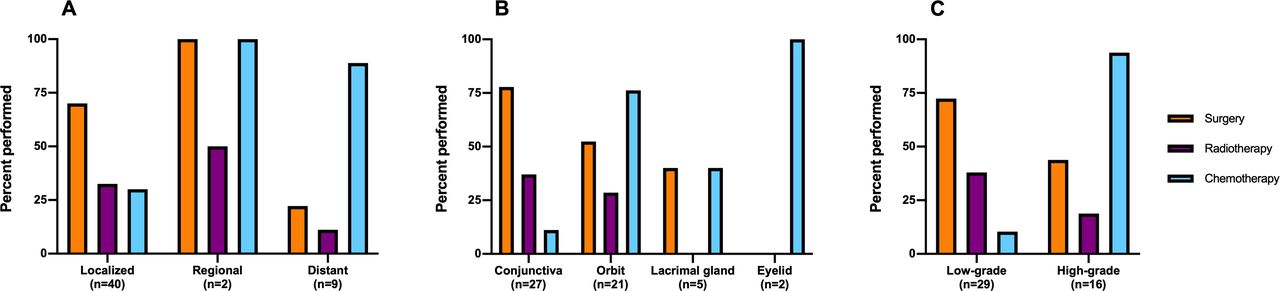
Radiotherapy, the most commonly used therapy for localised adult OAL, was less frequently used in the paediatric population, possibly owing to its side effects, which can be detrimental in children—namely cataract formation, dry eye, keratitis, retinopathy, facial bony deformities and the life-long risk of secondary malignancies. Similar to adult OAL,39 42 chemotherapy was the preferred treatment for advanced stages and more aggressive histological subtypes in our cohort (table 3 and figure 2). Excision of the tumour alone was performed mainly in the case of localised, low-grade, unilateral tumours, particularly of the conjunctiva (table 3 and figure 2), in accordance with case reports and other reports on paediatric ocular adnexal lymphoma and lymphoma in general.13 17 18 43–46 During the follow-up period that lasted for up to 35 years from diagnosis, no second primary malignancies were observed in our cohort. More focused multicentre studies are needed to establish these patients’ risk for second malignancy development and association with radiation therapy and chemotherapy.
{kind=link}
{kind=link}
Treatment of paediatric ocular adnexal lymphoma according to (A) tumour stage, (B) tumour location and (C) tumour grade.
Overall and subtype-specific survival rates were comparable to survival in adults. The histological subtype was the primary predictor of outcome, with DLBCL and ALCL demonstrating higher mortality.36 47 Orbital involvement and advanced stage seem to also contribute to prognosis; however, this may be explained by the fact that these high-grade lymphomas were frequently located in the orbit and were commonly advanced at diagnosis. Similar to the 90%–96% disease-specific survival of ocular adnexal marginal zone lymphoma,37 no deaths were witnessed among patients with EMZL in our cohort. Similarly, no deaths were also documented among the patients with FL.48
The rarity of OAL in children and adolescents hampers the feasibility of large-scale investigations. Our data were derived from a large, population-based cancer registry that spans over four decades. To our knowledge, this is the first study investigating this rare entity. Our findings can be a reference point for clinicians who encounter these cases.
Limitations of our study include its retrospective design and missing data on chemotherapy and use of rituximab, radiation dose, immunodeficiency, patient symptomatology, tumour recurrences, immunohistochemistry and the presence of multifocal disease. Moreover, due to the rarity of paediatric OAL, the sample size may not be adequate for subgroup analyses and for achieving statistical significance in IR differences. Finally, in this study, staging categorisation was largely based on the SEER summary stage, rather than the TNM-based staging which is frequently used in clinical practice.48–51
In summary, our study provides insight on the clinicopathological features and survival of paediatric OAL per histological subtype. EMZL comprised the majority of tumours. Radiotherapy may be less frequently used in children. Future studies should supplement our data with the radiation doses and chemotherapeutic regimens used in this patient group.
Acknowledgments
The authors would like to thank Gerasimos Tsilimidos, MD (Department of Medicine, Lausanne University Hospital, Lausanne, Switzerland) for his insight and for reviewing the manuscript.
References
Footnotes
Contributors GAM conceptualised the study, searched the literature, analysed the data, wrote and revised the manuscript; AKT provided statistical feedback and revised the manuscript; MEA revised the manuscript; DGV conceptualised the study, revised the manuscript, earned funding for the study and supervised the whole work.
Funding This study was supported by the Yeatts Family Foundation (DGV); Monte J. Wallace (DGV); 2013 Macula Society Research Grant Award (DGV); a Physician Scientist Award (DGV); unrestricted grant from the Research to Prevent Blindness Foundation (DGV); National Eye Institute (NEI) R21EY023079-01/A1 (DGV); Loeffler Family Fund (DGV); R01EY025362-01 (DGV); ARI Young Investigator Award (DGV); Foundation Lions Eye Research Fund (DGV).
Competing interests DGV is consultant to Olix Therapeutics and Valitor and co-founder of The Therapeutics.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval This study was approved by the Massachusetts Eye and Ear Institutional Review Board & Partners Human Research (Protocol #: 2019P001227). Our study and data accumulation were in conformity with all country, federal or state laws, and the study adhered to the tenets of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository;