Article Text

Abstract
Objective To introduce a special subgroup, retinal artery occlusion (RAO) with multiple emboli, which is highly associated with ipsilateral carotid artery occlusion disease (CAOD).
Methods and analysis This is a cohort study. Cases of RAO with multiple retinal emboli were consecutively enrolled. All patients underwent at least one of the carotid/cerebral evaluations: carotid arteriography, orbital/carotid colour Doppler ultrasonography and CT angiography to demonstrate haemodynamic changes and to discuss possible mechanisms and pathways of the emboli.
Results Among 208 RAO eyes, 12 eyes (5.7%) in 11 patients had multiple emboli were recruited in this study. Eleven eyes (91.6%) had ipsilateral carotid plaques and atherosclerosis with high-grade stenosis; among them, five were total carotid occlusion. Haemodynamic changes were found in nine patients with RAO (81.8%) with carotid stenosis 60% or greater. Most compensatory intracranial circulations were re-established via the circle of Willi with antegrade ophthalmic flows, but the direction of ophthalmic flow reversed in three eyes indicating the recruitment of external collaterals. Two cases underwent carotid stent successfully.
Conclusion RAOs with multiple emboli are rare but highly associated with severe CAOD with haemodynamic flow changes, warning critical condition in carotid/cerebral circulations. Either direct embolism from the carotid or cardiac lesions or indirect embolism via the collateral pathways is the mechanism of pathogenesis. Immediate action should start to manage these patients to prevent further deterioration.
- retina
- imaging
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Around 16%~35% patients with retinal artery occlusion (RAO) were reported to have ipsilateral flow-limiting carotid stenosis; however, retinal embolus and type of RAO are poor predictors of haemodynamically significant carotid artery occlusion disease (CAOD).
What are the new findings?
RAO with multiple emboli is rare but highly (91.6%) associated with severe CAOD and flow changes.
How might these results change the focus of research or clinical practice?
Embolism may arise from either the carotid lesions directly or via the collateral pathways indirectly as an important warning of haemodynamic changes of severe CAOD.
Immediate action should start to manage these patients.
Summary statement
Cases of retinal artery occlusion with multiple emboli are rare but highly associated with severe carotid artery occlusion disease and haemodynamic flow changes. Embolism may arise from either the carotid lesions directly or via the collateral pathways indirectly. Immediate action should start to manage these patients.
Introduction
Retinal artery occlusion (RAO) is an emergent ocular disorder that frequently results in profound and permanent loss of vision. Embolism originating from carotid or cardiac lesion is the most common cause. In the literature, RAO served as a significant marker for carotid artery occlusion disease (CAOD) and a predisposing factor of cerebrovascular accident (CVA).1–6 Most patients with RAO had ipsilateral carotid lesions, atherosclerotic plaque or stenosis; and in a few cases (16%~35%), the carotid stenosis was flow-limiting or even totally occluded with haemodynamically significant intracranial flow changes.2–6 In the literature, investigators had attempted to find out what clinical features of RAO were related to haemodynamically significant CAOD. However, they concluded that ocular symptoms and findings including retinal embolus and type of RAO are poor predictors of haemodynamically significant CAOD.6–10
In recent years, great advances in the development of carotid/cerebral imaging and flow studies, more timely clinical information and evidence can be collected and surveyed to facilitate the understanding of relationships between RAO and CAOD. During review of our cases at a single medical centre (Changhua Christian Hospital), we found a special subgroup, RAO with multiple retinal emboli, was highly associated with ipsilateral haemodynamically significant CAOD. Herein, we introduce these cases with findings of carotid/cerebral evaluations to discuss the association and the possible mechanisms and pathways of retinal emboli as a preliminary report. Issues about the retinal manifestations of this special subgroup will be discussed in the subsequent report.
Patients and methods
We conducted a retrospective cohort study of carotid/cerebral/ophthalmic flow evaluations in cases of acute RAO with multiple retinal emboli found at Changhua Christian Hospital. All patients had the typical clinical presentations of RAO including sudden onset of visual loss, retinal whitening and visible retinal emboli. At least one of the carotid/cerebral evaluations including carotid/cerebral arteriography, colour Doppler imaging (CDI), CT angiography (CTA) and magnetic resonance angiography (MRA) was performed to find out the presence of plaque, the degree of vascular stenosis at common carotid artery (CCA), internal carotid artery (ICA) and external carotid artery (ECA), and if possible, to determine the supply of compensatory flow and the pattern of collateral pathways for the intracranial circulation. Additional orbital CDI was also performed for these cases to detect blood flow signals parallel to the optic nerve to find out the flow velocity and the direction of ophthalmic blood flow. Haemodynamically significant COAD is defined as flow-limiting carotid stenosis with decreased cerebral blood perfusion and/or the presence of responsive compensatory flow to redistribute the intracranial circulations.
Patient and public involvement
Patients were not directly involved in the design of this study.
Result
From January 2004 to December 2017, among a total of 208 eyes of acute RAO, 12 eyes (5.7 %) in 11 patients with multiple retinal emboli were consecutively enrolled in this study. Patients’ age, gender, visual acuity at presenting and results of carotid evaluation were recorded as shown in table 1.
Demographic characteristics data and results of carotid/cerebral evaluations
There were two female and nine males, the average age was 66.0±11.9 years (range 50–88 years). All these RAOs were non-arteritic. Most associated systemic condition was arterial hypertension. Two cases (#7, #9) underwent ipsilateral neck radiotherapy for neoplasm 10 years ago. Prior to the RAO attack, CT and CDI for case 7 demonstrated already-occluded CCA and high-grade ICA stenosis as a result of therapeutic embolisation with balloons to occlude the left carotid aneurysm. Except case 7, all other patients were full ambulatory when visiting our hospital. Most cases had no neurological deficit, only case 2 reported transient limb weakness and case 11 presented with persistent slurred speech. Eight cases were afflicted in the right eye while two cases (#7, #11) in the left eye. One case (#2) had visual loss successively in his both eyes within an interval of 1 day (table 1).
Fundus features
All RAO eyes had acute retinal ischaemia manifested by retinal whitening in the posterior pole (figure 1A). Two cases presented as branch RAO (figure 2) and nine cases presented as central RAO with a cherry-red spot. In six eyes, an embolus was seen impacted on the optic disc, while in all RAO eyes, smaller emboli were present in the peripheral retinal arteries, at the bifurcation or the terminals. There were emboli with corresponding retinal opacities while some emboli dispersed in normal coloured retina. The number of emboli were 5 or less in three eyes, and exceeded to 10 in nine eyes of this survey (table 1).

Case 9 with right retinal artery occlusion (RAO) and internal carotid artery (ICA) occlusion. (A) Montage fundus photograph of right RAO with retinal whitening and an embolus impact on the optic disc and some emboli at the bifurcations. At the superior and nasal retina, there are emboli without corresponding retinal opacities. (B) Colour Doppler imaging (CDI) of right ICA demonstrates occluded vessel with diminished flow signal. (C) CDI of left ICA demonstrates highly increased flow (456.9 cc/min).
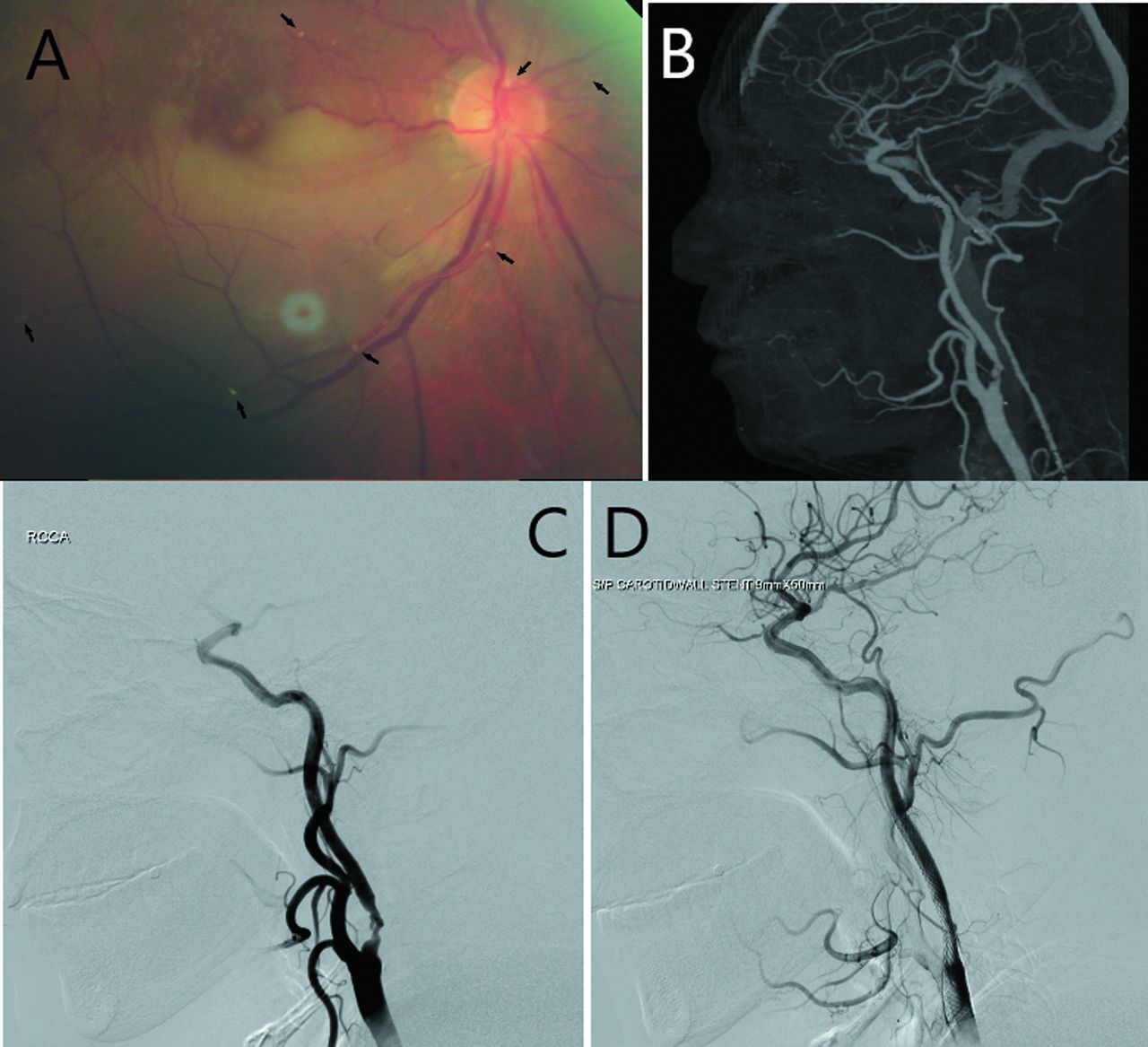
Case 5 with right retinal artery occlusion (RAO) and internal carotid artery (ICA) occlusion. (A) Fundus photograph reveals retinal whitening of inferior macula with emboli on the disc and in peripheral retinal arteries (arrow). There are collaterals and shunts at superior macula as remnants of previous branch retinal vein occlusion (BRVO). (B) CT angiography (CTA) demonstrates right ICA stenosis with calcified ulcerative plaque. (C) Arteriography prior to carotid stenting. (D) Arteriography after carotid stenting.
Results of carotid and cerebral evaluations
All patients underwent at least one of the carotid/cerebral evaluations. Most evaluations were performed within 1 month (online supplementary table). For case 2, thrombolysis therapy under carotid arteriography was performed immediately but the thrombolysis was not done due to the finding of bilateral carotid occlusions. The thrombolysis therapy was also suggested for other cases but was not accepted after detailed explanations of this invasive procedure. Non-invasive studies, CTA and CDI, were more acceptable for all patients. CDI was arranged as the primary evaluation in eight cases. In two cases (#4 and #5), CTA was performed first, CDI was arranged as follow-up evaluation for poststent condition. Case 7 with already-occluded CCA underwent CDI and CTA prior to the RAO attack.
Supplemental material
Carotid artery: summary of CTA and CDI data revealed that, among 12 RAO eyes with multiple emboli, 11 eyes (91.6%) had ipsilateral carotid plaques and atherosclerosis, of which 6 had high-grade carotid stenosis (58%–95%) and the other five had total carotid occlusion (online supplementary table). Case 3 had no carotid plaque nor stenosis. Case 2 suffered from bilateral RAO, had bilateral ICA occlusions. Carotid evaluations for the non-RAO side revealed no stenosis in two case (#3, #7), and low-grade stenosis (<50%) in the others. Case 6, with multiple carotid plaques and 58% stenosis, had normal ICA flow for the intracranial circulation. Flow studies demonstrated decreased or diminished carotid/cerebral flow where ICA stenosis was 60% or more (figure 1B). There were increased compensatory flows from the contralateral ICA in most cases (figures 1C and 3A).
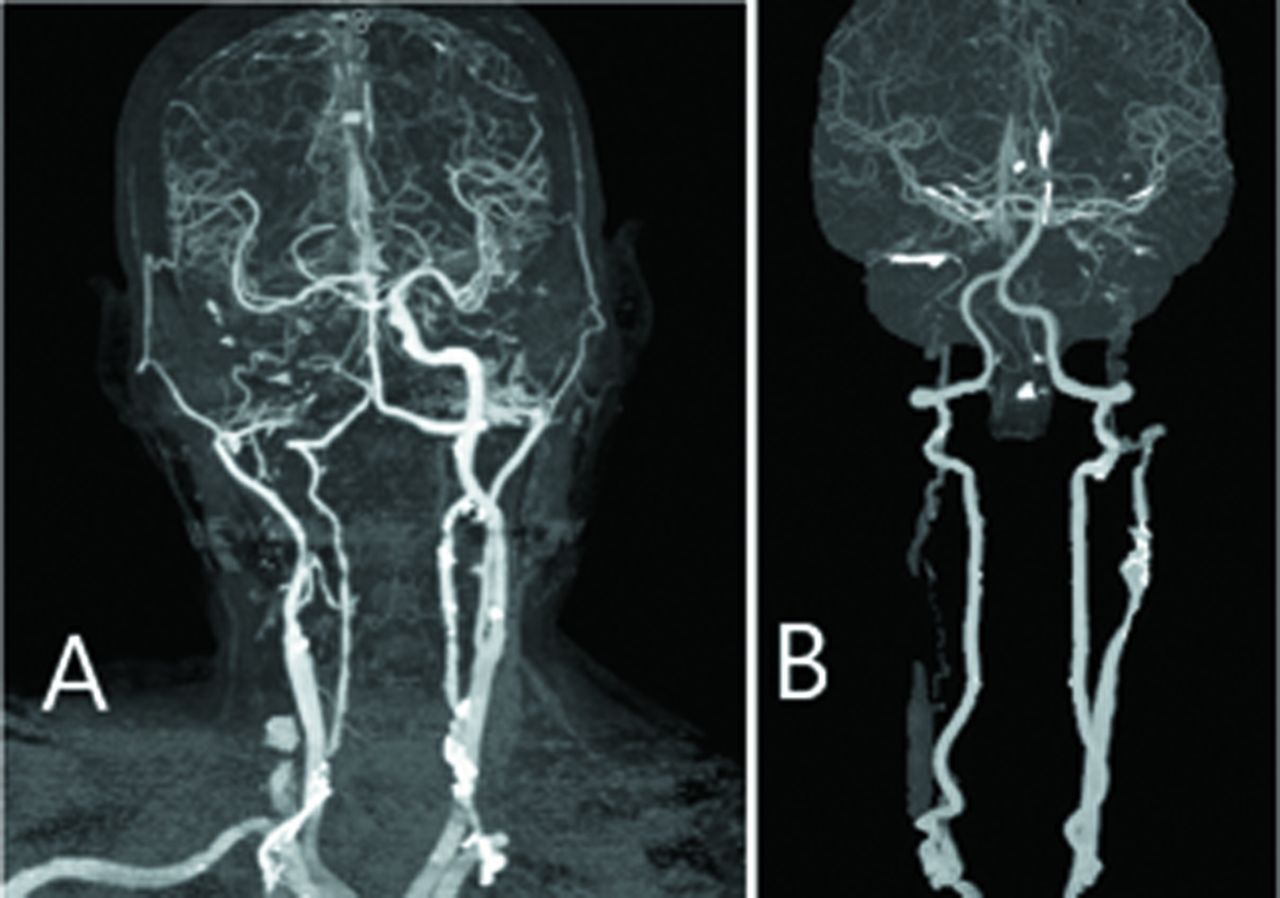
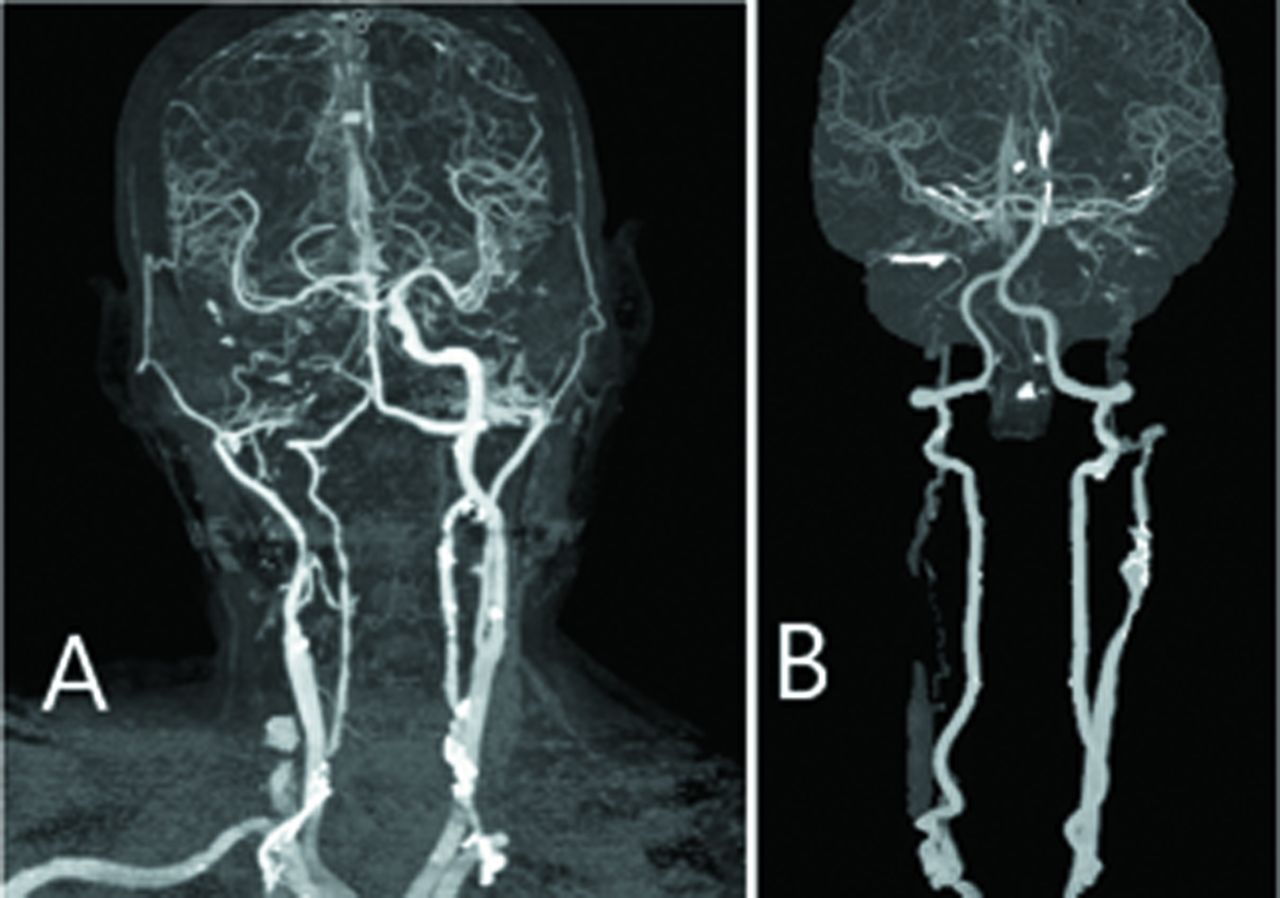
CT angiography (CTA) demonstrates severe carotid artery occlusion disease (CAOD) with compensatory flows. (A) CTA of case 9 shows right internal carotid artery (ICA) occlusion with high compensatory flow from left ICA. (B) CTA of case 2 shows long irregular stenosis of right common carotid artery (CCA) and total occlusion of bilateral ICA without carotid flow for the brain. There are compensatory flows from bilateral vertebral arteries posteriorly perfusing to anterior cerebral territories.
CTA and CDI both revealed haemodynamic changes in the vertebral artery. Increased vertebral flow may contribute to compensate the intracranial circulation (figure 3B). CDI demonstrated relatively high vertebral flow (>100 mL/min) bilaterally in three cases (#2, #8, #11), and unilaterally in five cases (#1, #6, #7, #9, #10) (online supplementary table).
Orbital CDI may reveal the flow velocity and direction of ophthalmic artery. There were antegrade ophthalmic flows in most RAO eyes, but the ophthalmic flow direction reversed in three eyes of two cases (#2, 10) (figure 4).

Orbital colour Doppler imaging (CDI) of case 2 demonstrates reversed flow of right ophthalmic artery.
Significant haemodynamic changes as decreased carotid/cerebral blood perfusion and/or responsive compensatory flows for intracranial redistributions were found in nine patients with RAO (81.8%) with carotid stenosis 60% or greater. Case 6 with ICA stenosis (58%) had normal carotid flow (online supplementary table). Most intracranial circulations were re-established via the circle of Willi by compensatory flows from the non-RAO side ICA laterally or from the vertebral artery posteriorly. Reversed ophthalmic flows, noted in three eyes, indicate compensatory flow arise from external carotid/ophthalmic anastomosis in poor function of Willisian collaterals. More retinal emboli in number seems highly related with CAOD and marked haemodynamic changes (table 1).
All patients with RAO were referred to neurology department for further evaluation and treatment. A few weeks later, three cases (#4, #5 and #11) underwent carotid stenting under arteriography which was performed successfully in two cases (figure 2D), but failed in case 11 due to reattack of ischaemic infarction with slurred speech during the procedure. During the follow-up, unfortunately, two patients passed away, case 2 after 8 months and case 7 in 6 weeks.
Discussion
Embolism originating from carotid or cardiac lesion is the most common cause of RAO while haemodynamically significant CAOD may also result in retinal ischaemia in fewer RAO cases.10 Both embolic and haemodynamic mechanisms can coincide in a RAO episode in special case.11 In a large cohort study, carotid Doppler/angiography showed ipsilateral ICA had >50% stenosis in 31% of non-arteritic CRAO and plaques in 71% of non-arteritic CRAO as the source of emboli.9 10 However, retinal embolus can be found under fundus photography in a few RAO eyes.12 13 Most causative emboli of RAO are not visible in the eye because the embolus may have migrated and disappeared or it is actually impacted in the proximal part, especially where CRA pierces the dura mater of the optic nerve sheath, the narrowest lumen of the artery.10 Asymptomatic emboli can be detected within the retinal artery in 0.4%–3.0% of adults and the elderly, and are associated with hypertension, smoking, vascular disease and increased stroke-related mortality.14–20 In the literature, the association of retinal emboli and increased risk of cerebrovascular disease has been well described.14–23
RAO is an emergent ocular vascular occlusive disorder that frequently results in profound loss of vision, and these patients are at risk of a cerebrovascular accident. In past decades, investigators had attempted to find out the association between RAO and CAOD, and what clinical features of RAO were related to haemodynamically significant CAOD. Merchut et al6 found the type of RAO, whether branch or central, was not predictive of severe CAOD and no clinical features of RAO were significantly associated with a flow-limiting carotid stenosis. Sharma et al7 noted haemodynamically significant CAOD in only 18.7% of patients with acute RAO. McCullough et al8 found that amaurosis fugax, Hollenhorst plaques and venous stasis retinopathy demonstrated moderate predictive value, whereas RAO and all other ocular findings demonstrated no predictive value in identifying CAOD. They all concluded that ocular symptoms and findings including retinal embolus and type of RAO are poor predictors of haemodynamically significant CAOD.6–10
In recent years, with the development and application of high-resolution carotid imaging studies including carotid arteriography, Duplex ultrasonography, CTA and MRA, more timely clinical information and evidences can be collected and surveyed to facilitate the understanding of relationships between RAO and CAOD. During review of our cases, we found a very special subgroup, RAO eyes with multiple retinal emboli, is strikingly correlated with ipsilateral CAOD. In this subgroup, 11 RAO eyes (91.7%) had ipsilateral carotid plaques with high-grade stenosis; among them, 5 were total carotid occlusion. In nine cases (81.8%), significant haemodynamic changes as decreased carotid/cerebral blood perfusion were found (table 1). Compensatory flows from the contralateral ICA or the vertebral arteries contribute to the redistribution of intracranial circulation via the circle of Willi in most cases (figure 3).
RAO eyes with presence of multiple emboli and severe CAOD is not a new disease entity. Sporadic cases have been reported since 1970s,24 but little is discussed about the pathogenesis of multiple emboli in the condition of totally occluded and severely stenotic carotid arteries on the same side. The pathogenesis of RAO with multiple emboli and ipsilateral CAOD may be more complicated than we previously learnt. Embolism is the most common cause of RAO; carotid plaques or cardiac lesions are usually the source of embolism, and there are three main types of embolic findings in RAO that include cholesterol, calcium and platelet-fibrin emboli.9 10 In our case series, an embolus was seen impacted on the optic disc in six eyes, while numerous microemboli were present in the peripheral retinal arteries, at the bifurcation or the terminal in all RAO eyes (figures 1A and 2A). These microemboli may result from different pathogenesis and pathways. A classic way of multiple emboli formation is that blood flow through a stenotic vessel or diseased valve may cause turbulence with part of an unstable plaque dislodged from the vessel wall; and it may possibly act like a comet with a major nuclei associated with many minor meteoric dust flaked off in the same time. However, this mechanism is possible only for part of our cases whose carotid arteries were stenotic, but not for those cases with totally occluded arteries.
In addition to the mechanism of direct embolism from carotid or cardiac lesions, indirect embolism from collaterals during haemodynamic changes of severe CAOD also plays an important role. There are two collateral pathways: from the intracranial or the external collaterals (figure 5). First, during haemodynamic changes of severe carotid stenosis, the compensatory flows from contralateral ICA perfused via the circle of Willis may have flow in abnormal direction and thus raise some dust or cell debris forming microemboli in the vessel. Most probable site for emboli formation during haemodynamic changes, we suspect, is the ipsilateral distal ICA where they collapse with reduced perfusion immediately at the onset of proximal ICA occlusion and later become re-opened by the compensatory flows from intracranial communicating vessels downwards and then feeding the ophthalmic territories (figure 5A). Since most of our cases showed no neurological deficit, these microemboli are benign in the cerebral territories but may be visible in the eye and result in retinal infarctions with visual symptoms. This mechanism is possible for cases who has compensated intracranial circulations with antegrade ophthalmic flow as observed by orbital CDI in most of our reported cases.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
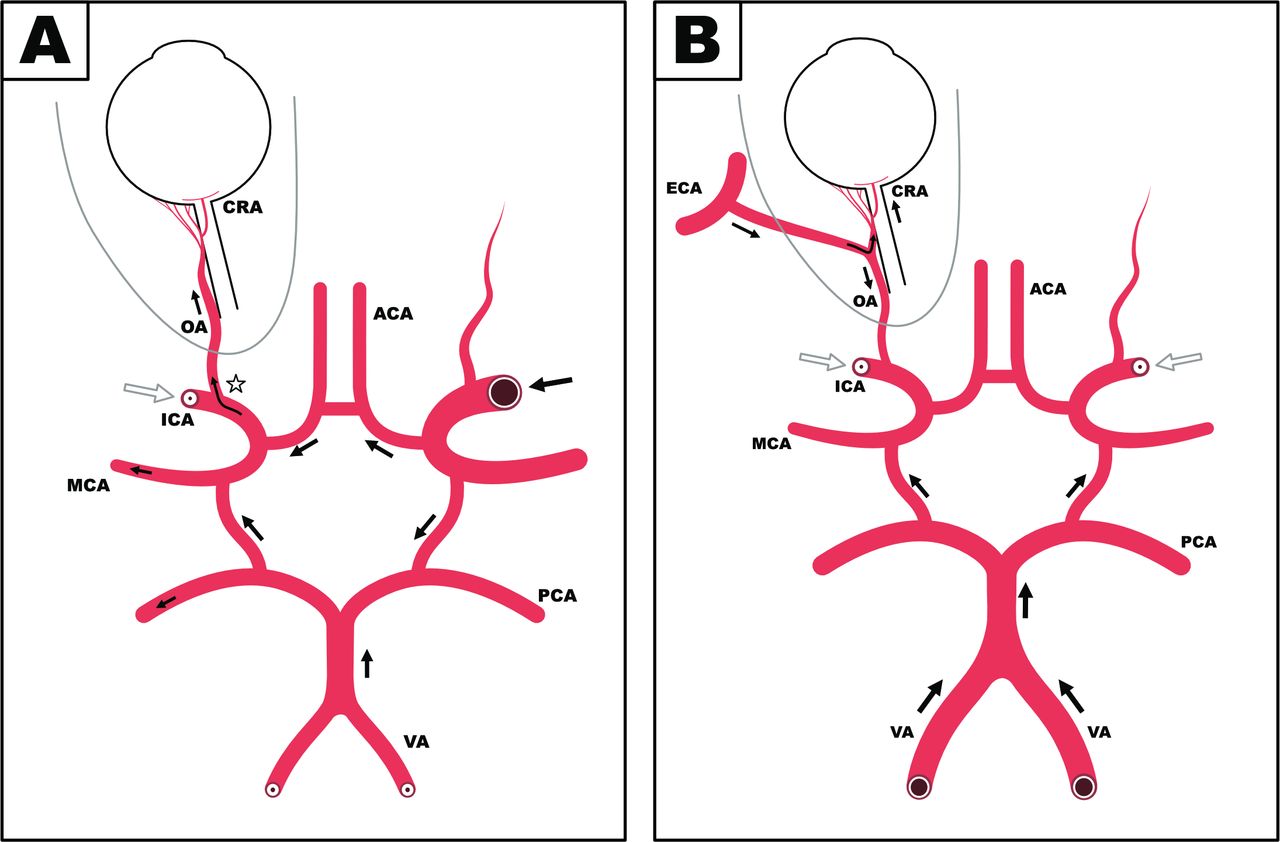
Schematic diagrams of the collateral pathways for haemodynamically significant carotid artery occlusion disease. (A) In the status of unilateral carotid occlusion, compensatory flows perfuse from contralateral ICA may have flow in abnormal direction in the circle of Willis. Most probable site for emboli formation is the ipsilateral distal ICA (star) where they collapse at the onset of proximal ICA occlusion and later become re-opened by the compensatory flows. The ophthalmic flow is antegrade in the orbit. (B) In the status of bilateral carotid occlusion with poor function of Willisian collaterals, compensatory flows from the vertebral arteries are not sufficient to the eye. The source of blood supply is then from branches of the ECA. The ophthalmic flow becomes retrograde in the orbit. ACA, anterior cerebral artery; ECA, external carotid artery; ICA, internal carotid artery; MCA, middle cerebral artery; MMA, middle meningeal artery; PCA, posterior cerebral artery; OA, ophthalmic artery; VA, vertebral artery.
The second pathway of emboli is from the compensated flow originated from ECA/ophthalmic anastomosis in poor function of Willisian collaterals (figure 5B). CTA of case 2 demonstrated bilateral carotid occlusion with intracranial compensatory flow only from the vertebral circulation (figure 3B). It may be fair for the brain but not sufficient to the eye and will lead to the recruitment of external collaterals with reversed ophthalmic flow noted by orbital CDI (figure 4). The major source of blood supply to the ophthalmic artery is then from branches of the ECA.10 The enlargement of an anastomosis and flow direction changes of the compensatory circulation may facilitate debris scaling off the vessel wall and become emboli in the fundus. Reversed ophthalmic flow is also noted in ocular ischaemic syndrome secondary to chronic CAOD. But retinal whitening and emboli are seldom found in such cases.
The circle of Willis is the major collateral pathway that can rapidly compensate for decreased cerebral perfusion pressure. External collaterals through the ophthalmic artery is recruited when compensatory flow via the circle of Willis is inadequate for the brain or to the eye.25 Thus, during attack of severe CAOD, haemodynamic changes will response with compensatory flows to redistribute the intracranial circulations in order to restore enough blood perfusion for the brain to prevent neurological deficits and stroke. All the haemodynamic changes in collaterals, including dilatation of collateral vessels, flow direction changes in communicating vessels, reopening of collapsed carotid artery and enlargement of an anastomosis, could contribute to the formation of emboli (figure 5). We believe that indirect emboli from collaterals could be the answer for pathogenesis of multiple emboli in cases of CAOD with haemodynamic changes. Thus, the presentation of RAO with multiple emboli is highly correlated with haemodynamically significant CAOD as a sign marking that compensatory flows for redistribution has already re-established.
Multiple emboli were rarely found in all RAO eyes, only 5.7% of our survey. Multiple emboli may also form during invasive carotid procedures. Sequelae of carotid arteriography and endarterectomy, such as RAO or CVA may have occurred during or after the procedure.26 27 Retinal emboli can be asymptomatic and happen more often than we would expect. Hayreh mentioned that ‘during carotid endarterectomy, in which showers of multiple, moving emboli kept appearing and disappearing without any permanent residual embolus seen later on in the retinal arteries, or visual loss’.10 With distal embolic protection device to occlude ICA temporarily during carotid angioplasty and stenting to prevent embolic stroke, ipsilateral RAO and retinal embolisation could still occur.28–30 The passage of debris through the collaterals poses a significant risk as flushing debris through the orbital branch of ECA to ophthalmic artery may lead to retinal embolisation (figure 5B).29 Transient blindness in patients with a fully occluded ipsilateral ICA also unequivocally indicates the collateral pathway to be a mechanism for retinal embolisation. The retina provides a unique observatory for the study of emboli, which may occur either directly or indirectly via collaterals to the ophthalmic artery.28
The finding of a retinal embolus is considered a grim prognostic sign for survival of RAO cases as they are of higher risk of CVA.14–23 With experiences of the presenting cases in this report, we recognised the fact that, although most patients are fully ambulatory without neurological deficits, cases of RAO with multiple emboli are in a critical condition as amaurosis fugax and transient ischaemic attacks (TIAs) and are at increasing risk of neurological morbidity and mortality. It is an important warning that, prior to the attack of neurological deficit signs of CVA, there already exist haemodynamically significant CAOD with circulatory redistribution. It could be an inevitable result of severe CAOD. However, this subgroup is small in number and is often missed clinically or obscured in large cohort study. Thorough carotid/cerebral evaluations and adequate treatment should be arranged and performed earlier as possible to prevent the occurrence of impending cerebrovascular accident.
In conclusion, RAOs with multiple emboli are highly associated with severe CAOD. Either from the carotid or cardiac lesions directly or via the collaterals indirectly could be the pathway of embolism. Multiple emboli may represent existence of haemodynamic changes as a result of severe CAOD that compensatory flow to redistribute the intracranial circulation has established and perfuse again to the eye with emboli. The presentation of RAO with multiple emboli is emerging as an alarm of an incoming stroke more definitely, a critical sign as amaurosis fugax and TIA, alerting physicians to start actions to manage these patients with thorough evaluations and treatments to prevent further deterioration.
Acknowledgments
We thank Chen-wei Huang for schematic diagram (Figure 5) drawing.
References
Footnotes
Contributors J-FH, JH and S-LW planned the study. S-NC conducted a survey. J-FH submitted the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.