Article Text

Abstract
In humans, the lens is the organ with the ability to change morphology and refractive power, designated as accommodation, to focus light from various distances and obtain clear retinal image. The accommodative ability of the lens depends on its structure and biological parameters. The lens grows throughout the life, forming specific lens sutures and a unique gradient refractive index, and possesses regenerative ability under certain circumstances. Minimally invasive lens surgery that preserves endogenous lens epithelial stem/progenitor cells (LECs) can achieve functional lens regeneration in humans. The lens is the main source of intraocular aberration, especially intraocular higher-order aberrations (IHOAs) which is found to be binocularly symmetrical in phakic eyes. There is a compensation mechanism between corneal aberrations and lens aberrations. Therefore, the structure and the biological parameters of the lens, the binocular relationship of the lens and the correlation between the lens and cornea affect visual quality. This paper summarises the above findings and their current and potential applications in refractive surgeries, providing a comprehensive understanding of the lens as a strong determinant of visual quality in the optical system.
- lens and zonules
- vision
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The human eye is a dynamic, complex optical system. Accommodation, the mechanism by which an human eye increases refractive power, is produced by change in shape of the lens initiated by contraction of ciliary muscle.1 Accommodative ability of the lens allows us to see objects at different distances clearly.2 Accommodative ability of the lens is associated to its biological parameters.3 The lens grows throughout the life forming layer-by-layer structure, lens sutures and corresponding gradient refractive index (GRIN); therefore, its biological parameters are constantly changing with age.4 There is a balance between corneal positive spherical aberration and lens negative spherical aberration in young people.5 Understanding the lens and its role in accommodation and optimising visual quality is important in developing solutions when the lens is affected by ageing or disease.
The Structure of the Lens Defines Its Physiological Function
The anatomy and physiological function of the lens
The lens is an epithelial differentiated organ, which is elastic and transparent with a biconvex shape. It is located in the posterior chamber and supported by the vitreous body (figure 1A,B).

Slit-lamp microphotography and diagram of the structure of the lens. (A) Slit-lamp microphotography of the eye after mydriasis. The biconvex shape of the lens is clearly seen. (B) The diagram of the sectional view of the square part in the Panel A. (C) The cellular structure of the lens.
The lens consists of four parts (figure 1C): the lens capsule, the epithelial cells, the lens fibres and the zonules. Under normal circumstances, the lens is suspended on the ciliary body by the lens zonules, which are attached between the pars plana and the equatorial lens capsule.
The transparency of the lens allows light transmission with wavelengths up to 1200 nm.6 The prerequisites to maintain lens transparency include the tight and orderly arrangement of the lens fibre and the high solubility of lens proteins.7
The lens has the ability to accommodate to obtain clear retinal images of objects at different distances. Accommodation is accomplished by both the lens and the ciliary body.8 According to the Helmholtz accommodation theory, when looking at the distant objects, the ciliary muscles relax, so the lens zonules are in tension and the lens becomes flattened. On the other hand, for clear near vision, the ciliary muscle contracts and the lens zonules are relaxed, leading to the increasing convexity of the lens9 (figure 2 and online supplemental video).
Supplementary video

Diagram of the morphological and parametric changes of the lens during accommodation.
Dynamic changes of the physiological function of the lens: refraction and accommodation
The epithelial cells in the equatorial part of the lens continue to differentiation and grow throughout life, so the shape, weight and volume of the lens are constantly changing. The diameter of adult lens is about 9.0–10.0 mm, with an average annual growth of 0.023 mm and a thickness of lens is about 4.0–5.0 mm.10 Using different devices, many studies found that the anterior and posterior radius of curvature of the lens decreased significantly with age. Anterior segment optical coherence tomography (AS-OCT) and Scheimpflug imaging can provide sectional view of the ocular anterior segment including the lens. Dubbelman et al used Scheimpflug imaging technology to measure the radius of anterior lens surface curvature (RAL) and found that the RAL decreases 57 µm per year, and the radius of curvature of the posterior lens decreases 17 µm per year.11 Liu et al assessed the RAL measurements using AS-OCT and Scheimpflug imaging, RAL is found to decrease with age.12 Rosen et al measured the lens biological parameters of isolated eyes with different ages (20–99 years old) and found that the anterior curvature and thickness of the lens increased with age, but the posterior surface curvature of the lens changed little.13 However, the lenses are not held under force and the younger lenses will be in an accommodated form in in-vitro studies. Therefore, the research results cannot fully reflect the state of lens in vivo.
Dynamic change of the lens refractive power
The mean lens power in newborns is 45D, and it decreases to 25D at the age of 6 years.14 In Gullstrand model eyes, the refractive index of the lens cortex and nucleus are defined as 1.386 and 1.406, respectively.15 In fact, the lens has a more complex GRIN.16 Jones et al confirmed GRIN by using magnetic resonance imaging (MRI) to measure the sagittal refractive index distribution and age changes of human lens.17 Their results showed that the refractive index of the lens nucleus decreased significantly with age, while the refractive index of the lens cortex remained unchanged. The results show that with the increase of age, the overall refractive index of the lens decreases, resulting in decrease of the lens refractive power.
Accommodation and its age-related change
The accommodation ability of the lens greatly depends on its flexible surface curvature. The lens morphology and GRIN change with age and in the process of accommodation.18 19 The RAL decreases and the lens refractive power increases during accommodation.20 21 Kasthurirangan et al used MRI technique to observe the changes of the lens and the ciliary muscle in vivo of different ages under the accommodative stimulation of −4.8 to −6.9D.22 The results showed that the anterior chamber became shallower, the RAL decreased, the diameter of the equatorial part of the lens decreased and the diameter of the ciliary ring decreased. With the increase of age, the thickness of the lens and the equatorial diameter of the lens increased, but the radius of curvature of the posterior lens of the lens did not change. Furukawa et al recorded the dynamic process of the eye from accommodation to relaxation using the self-developed AS-OCT.23 When the lens is in the accommodation state, the anterior chamber becomes shallower, the lens thickness increases, and the radius of curvature of the anterior and posterior surface becomes smaller. Ni et al compared the changes of lens in the young group and presbyopia group under accommodation stimulation with a Scheimpflug camera.24 In the young subjects, the RAL significantly decreased and the lens thickness increased at −5D accommodation stimulation. However, there was no significant change in lens parameters in the presbyopia group. Some studies have shown that under accommodation stimulation, the lens nucleus becomes more convex, the central thickness increases, while the equatorial diameter decreases.25 Some studies have shown that GRIN changes little during lens accommodation.26–28 Generally, the above studies showed that with the increase of age, the accommodative latency gradually increased, and the overall biomechanics of the lens was not affected by age.
The embryonic development and specific suture formation of the lens
The growth of crystalline lens can be divided into two stages (figure 3): the formation of lens vesicles and the production of lens fibers.29 At the 22nd day of the embryo, the neural folds on both sides of the forebrain developed from the neural tube invaginate, forming the optic groove, which continues to form optic vesicle. The distal end of the optic vesicle continues to expand and form a double-layer cup-shaped structure, called the optic cup. After contact with the epidermal ectoderm, the optic vesicle induces thicken of epidermal ectoderm to form a lens placode, which is the primordium of the lens. The lens placode gradually detaches from the epidermal ectoderm to form lens vesicles.30

Embryonic development of the lens. (A) Transverse section of a neural tube-stage embryo where the OV reaches the epidermal ectoderm. (B) After contact with the epidermal ectoderm, the optic vesicle induces thicken of epidermal ectoderm to form LP, which is the primordium of the lens. (C) LP thickens and invaginates. (D) The distal end of the optic vesicle continues to expand and form a double-layer cup-shaped structure, called the OC. Lens placode separates from the head ectoderm to form the LV. (E) The anterior parietal cells of lens vesicles differentiated into LE, while the posterior cells gradually elongated to form primary LF. LE, lens epithelium; LF, lens fibres; LP, lens placode; LV, lens vesicle; OC, optic cup; OV, optic vesicle.
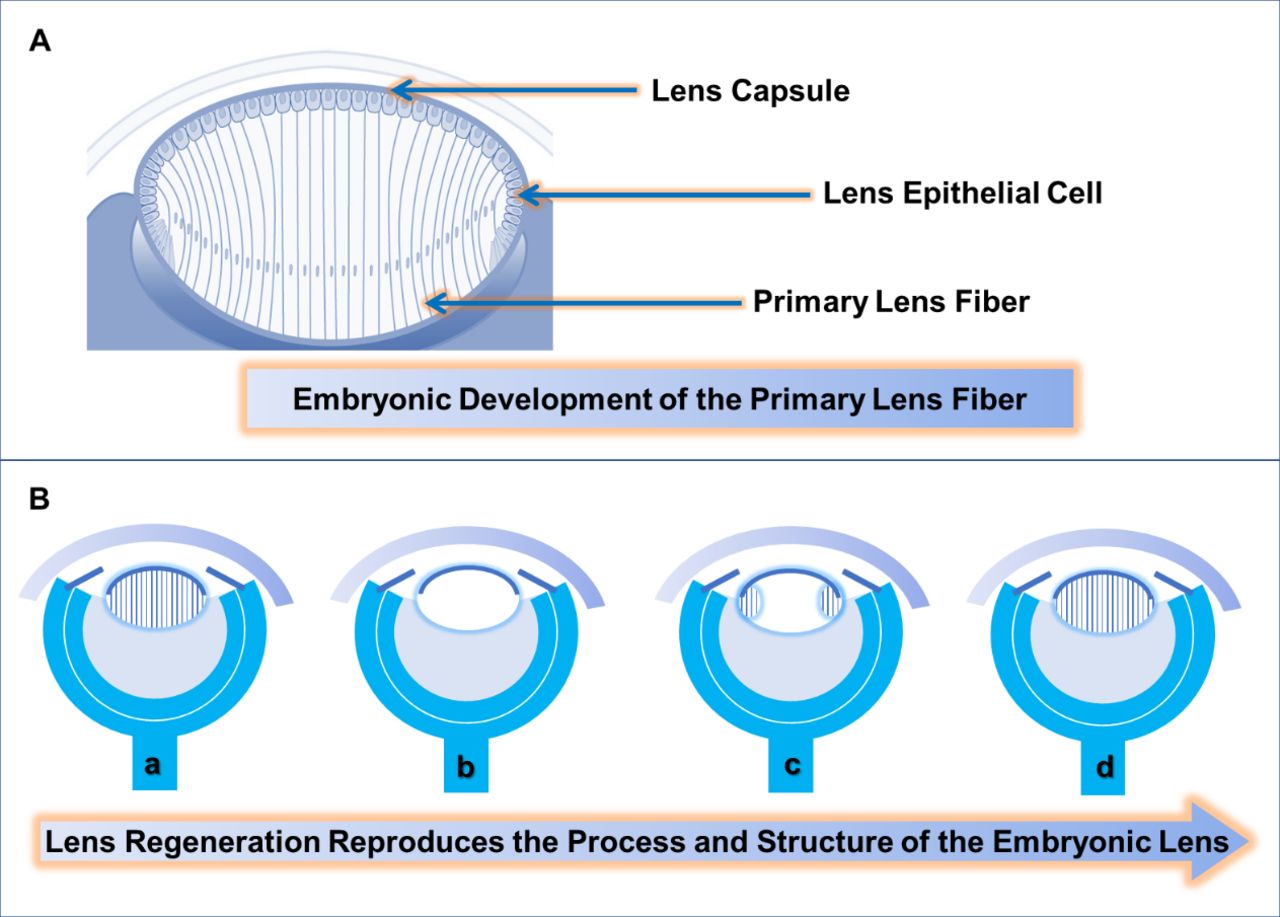
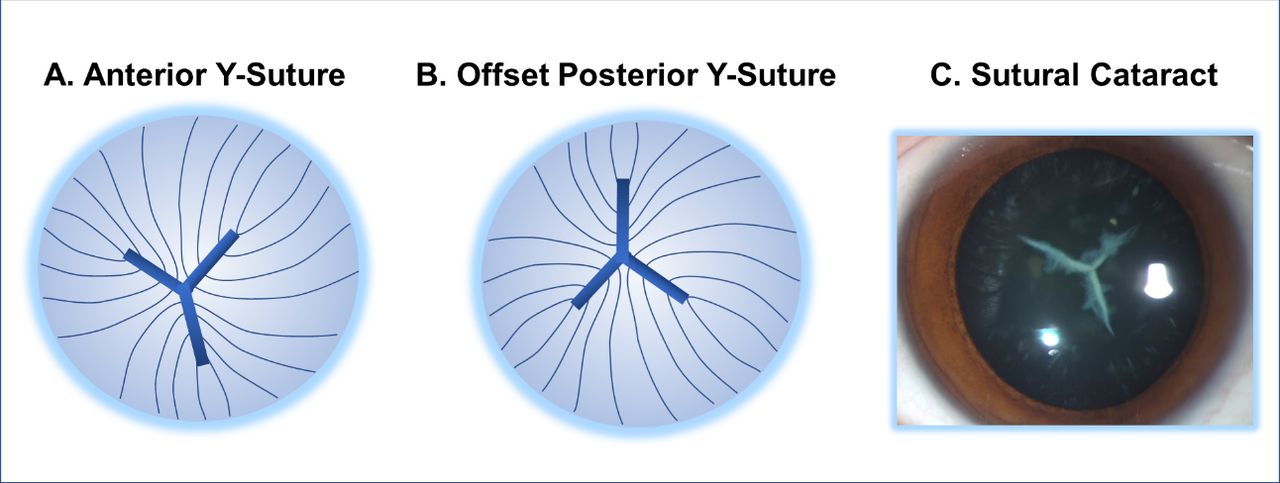
The anterior parietal cells of lens vesicles differentiated into lens epithelium, while the posterior cells gradually elongated to form primary lens fibres (figure 4A). The epithelial cells in the equatorial region of the lens continue to proliferate and grow, forming secondary lens fibers.31 The newly formed fibres surround the inner layer of fibres forming an onion-like structure. This process lasts for a lifetime but slows down with age. The ends of the fibres in each layer flatten and combine with each other to form a lens suture, with a Y-shaped suture in front of the nucleus and an offset Y-suture behind the nucleus (figure 5).

Lens regeneration in human may reproduce the normal structure of the lens. (A) Embryonic development of the primary lens fibres. (B Lens regeneration reproduces the process and structure of the embryonic lens. (a) A natural crystalline lens. (b) The lens content is removed and the lens capsule and the lens epithelium are preserved. (c) The regenerated lens fibres grow from the periphery to the centre. (d) The regenerated lens fibres elongate and refill the lens capsule.
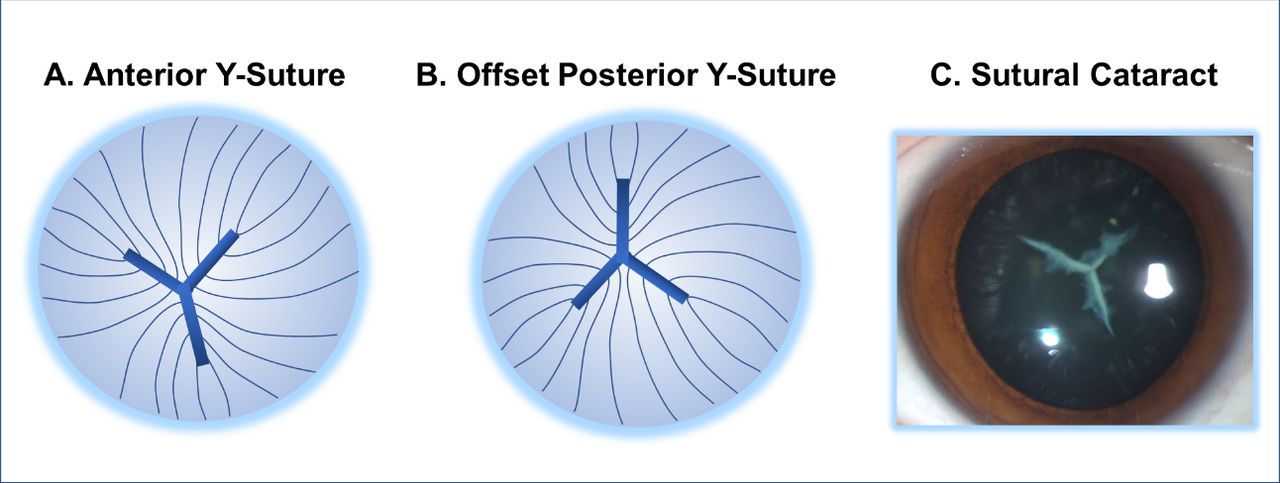
Anterior Y-suture and offset posterior Y-suture in humans. (A) The anterior ends of lens fibres are paired to form the Y-suture. (B) The posterior ends of lens fibres are paired to form an offset posterior Y-suture. (C) Sutural cataract is a morphological category of congenital cataract. The opacity located at the Y-suture makes the Y-shape clearly visible.
The highly organised arrangement and intercell connection with cellular gap junctions are crucial for maintenance of lens transparency.32 The solubility of intracellular high concentration of crystalline also greatly reduces light scattering.33–35 In the human embryonic stage, orderly arrangement and polarised growth begin to appear only when the secondary lens fibres appear, forming a growth layer, which marks the formation of lens suture.36 After birth, the suture of the human lens tends to be complicated and star-shaped sutures appear. Lens suture is the tissue structure principally responsible for lens aberration, such as astigmatism, spherical aberration, trefoil and so on, and the direction of lens suture is related to the axis of non-rotational symmetric aberration.37 Lens suture also plays an important role in accommodation.38 Kuszak et al found that accommodative ability of the lens is related to quantitative differences in fibre structure and suture organisation.39 For example, compared with birds, human lenses with surface discontinuous sutures have weaker accommodative ability.
Structure and function of the regenerated lens
Mammalian lens derives from the embryonic epithelial ectoderm which possesses the potential to regenerate after trauma or surgery. It has been found that if only the contents of the lens are removed and the lens capsule is preserved, the residual lens epithelial cells (LECs) can proliferate and regenerate lens materials.40–42 Lin et al removed the lens contents in New Zealand albino rabbits. On the seventh day after operation, the LECs on the posterior capsule elongated, changed from cubic to columnar and came into direct contact with the LECs under the anterior capsule, and the eosinophilic substance between the anterior and posterior capsule disappeared. This process reproduces the formation of primary lens fibres during embryonic development (figure 4B). However, researchers found that compared with natural lenses, the epithelial cells of the regenerated lenses had some morphological changes, including overly dense, indented nuclei, some oedematous mitochondria and an expanding endoplasmic reticulum.43
The optical quality of regenerated lens depends on its transparency, shape and elasticity, refractive power and aberrations. Some studies give qualitative statements. In the eyes of the rabbits that did not receive the implants, Gwon showed a picture of the fundus clearly visible.44 Lin et al studied lens regeneration in the New Zealand albino rabbits and found that the average refractive power of the regenerated lens was 15.6D at 15th month after operation, which was similar to that of the normal lens.42 Lin et al also analysed the function of the regenerated lens with a randomised clinical trial in 12 human cataractous infants receiving minimally invasive lens surgery versus 25 cataractous infants receiving traditional cataract surgery as control. It was found that the refractive power of the regenerated lens increased significantly from 1 week to 8 months after the operation and reached approximately 80% of that of the same age at 8 months after minimally invasive lens surgery. At the same time, the average accommodative response of the regenerated lens increased to 2.5D, which was much higher than that of the control group (p<0.001).
The Role of the Lens in Visual Quality
Effects of the lens on retinal imaging
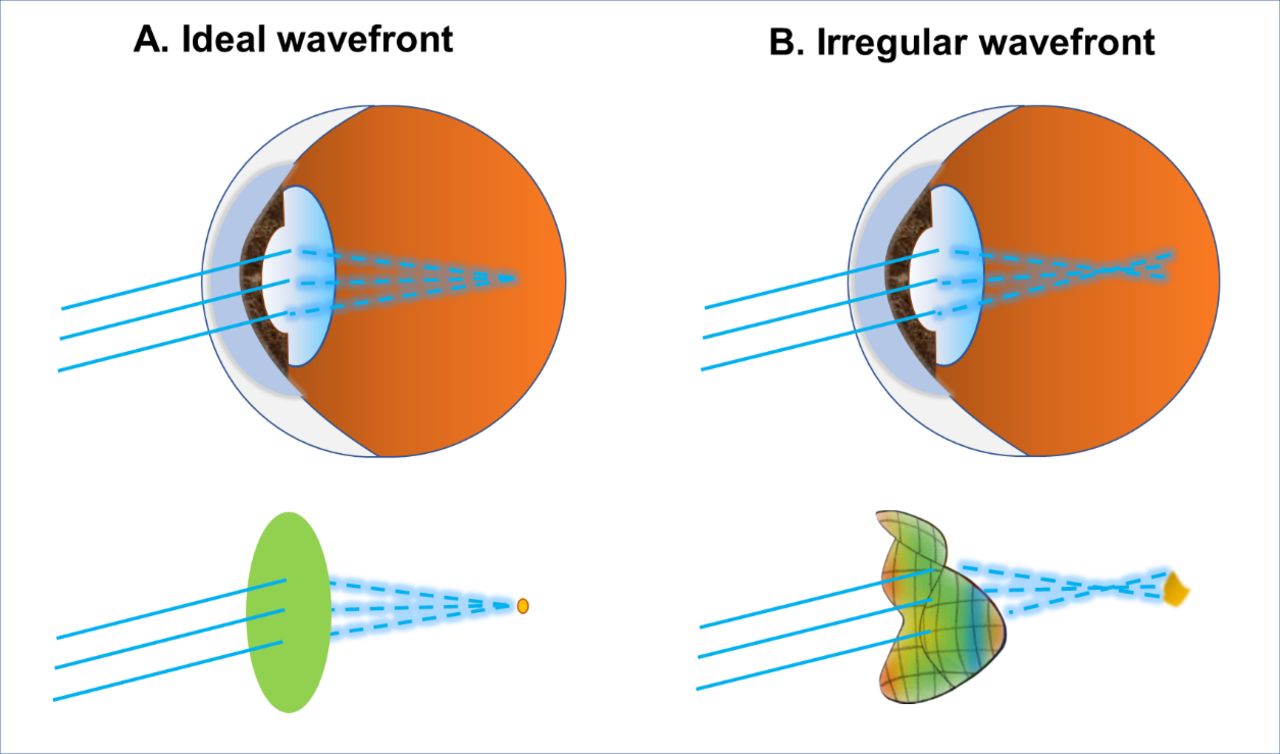
The ocular aberration refers to the position deviation between the ideal wavefront shape and the actual wavefront shape. Light is a travelling electromagnetic wave. When travelling through a medium, the surface formed by light emitting at the same time is define as wavefront. For an aberration-free eye, the infinitely distant point light source enters the eye through different areas of the pupil and focuses on the same point on the retina. However, in an aberrated eye, the point source does not focus on the same point on the retina and the retinal image of the point light source is hazy (figure 6).
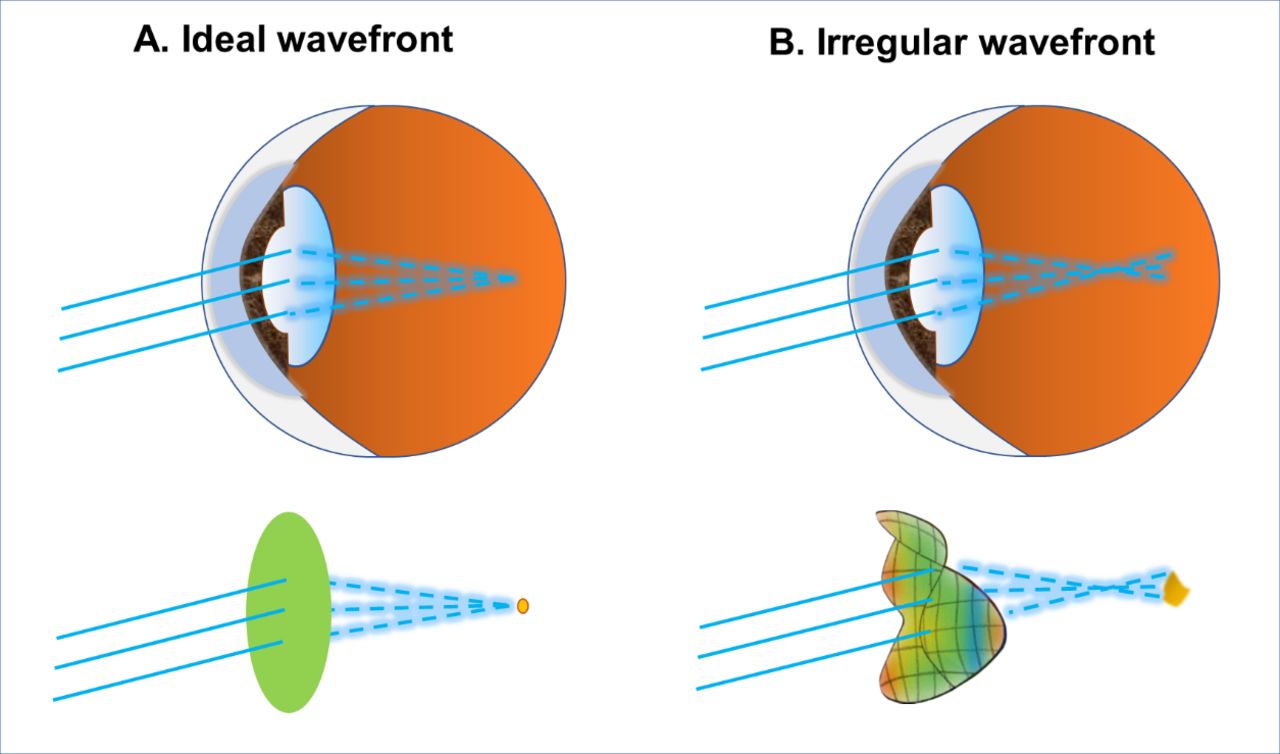
Diagram demonstrating the effects of irregular wavefront on the quality of retinal imaging. Light is a travelling electromagnetic wave. When travelling through a medium, the surface formed by light emitting at the same time is define as wavefront. (A) The infinitely distant point light source enters the optically ideal eye, which has a flat wavefront, and forms a clear point image on the retina. (B) The infinitely distant point light source enters the eye with aberrations, which has a distorted wavefront, and forms a hazy irregular image on the retina.
Ocular aberrations include low-order aberrations and high-order aberrations, in which low-order aberrations refer to defocus and astigmatism, and high-order aberrations include spherical aberration, coma, trefoil and so on. The low-order aberration accounts for a large proportion in human eye aberration, but it can be well corrected with glasses. Therefore, higher-order aberrations have become an important index to evaluate the visual quality after refractive surgery. The high-order aberrations of human eyes mainly come from the cornea and the lens, including spherical aberration and coma (including vertical and horizontal coma aberration). Previous studies have shown that the higher-order aberrations of the eyes increase with age, mainly due to changes in the lens.45 46 Under the condition of 6 mm pupil diameters, the intraocular spherical aberration (Z40) was positively correlated with age (r=0.382, p<0.001), and the intraocular coma aberration (Z41) was negatively correlated with age (r=0.459, p<0.001).
The age-related increase in lens-derived ocular aberrations results in decline of the modulation transfer function (MTF). Generally, the contrast of output image through an optical system is worse than that of input image. This variation of the contrast is closely related to the spatial frequency characteristics. The ratio of contrast between output image and input image is defined as MTF. Because the contrast of the output image is always less than that of the input image, the MTF value is between 0 and 1. MTF showed a turning point and decreased at the age of 40 years47
The higher-order aberrations of the lens also changed during the accommodation process.48 The results of Ke et al showed that higher-order aberrations change in gradually increased accommodation stimulus: Z40 decreases during −2D stimulation, and Z3-1, Z31, Z40, Z60 become negative during −4D stimulation and the negative change of Z31 is related to the change of anterior curvature of the lens during accommodation.49 Visual experience is considered to play an important role in regulating the axial growth of the eye, and humans also show transient changes in axial and choroidal thickness after short-term defocus exposure. Lau et al studied the relationship between high-order aberrations and axial growth in children in Hong Kong.50 The results showed that the total high-order aberrations and spherical aberration (the combination of Z40 and Z60) had a negative correlation with axial elongation, supporting the potential role of higher-order aberrations, including those from the lens, in childhood eye growth. Intraocular higher-order aberrations were mainly affected by the lens biological parameters. Zhang et al found similar results in children and young adults.51
Mutual compensation of ocular aberrations originated from cornea and the lens
It is found that in most young people, the corneal aberration alone is larger than the whole eye aberration, and there is mutual compensation between corneal and lens aberrations; the positive spherical aberration of the cornea can be compensated by the negative spherical aberration of the lens to maintain the balance of the overall aberration of the human eye to obtain better retinal imaging quality.52 In addition, asymmetric corneal aberrations, such as corneal astigmatism, can also be compensated by the lens, while corneal coma and lens aberrations mutually compensate to maintain the balance of ocular total aberrations. Corneal horizontal coma compensation varies with the amount of optical decentration. In patients with large Kappa angle, horizontal coma compensation is more obvious, which is common in hyperopia.53 The compensation effect of aberration decreases with the increase of age. In the elderly, the compensation effect of lens on corneal aberration obviously weakened or even disappeared.54
Effects of binocular symmetry of the lens on ocular aberrations
The symmetry of binocular optical system is the structural basis of the symmetry of binocular vision and aberration, which contribute to binocular depth perception and stereopsis.55 The symmetry of binocular optical system is reflected in the following aspects: (1) the corneal parameters of both eyes were highly symmetrical: there was a strong correlation among corneal thickness (R=0.90, p<0.001), corneal curvature (R=0.95, p<0.001) and posterior corneal surface height (R=0.72, p<0.001).56 (2) the lens parameters of both eyes were highly symmetrical: Wang et al found that there is a mirror symmetry relationship between the tilt size and direction of the binocular lens.57 The results of Li et al show that there is a symmetry in the thickness of the binocular lens.58
To define the normal range of binocular symmetry of each biological parameter of lens has important clinical opinion for guiding the parameter setting of refractive surgery.
Future Directions for Ocular Refractive Surgeries Involving the Lens
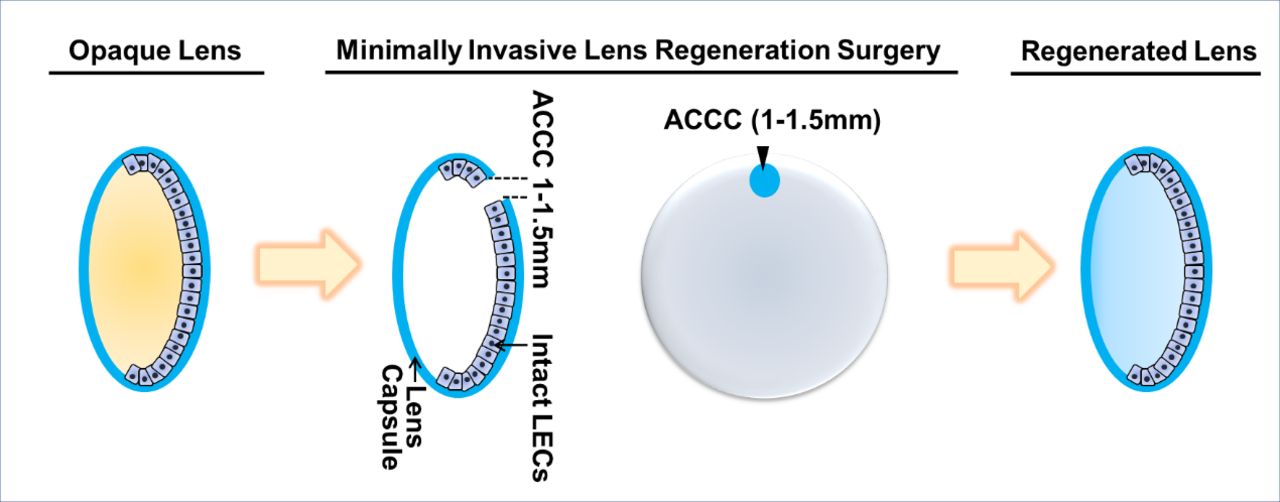
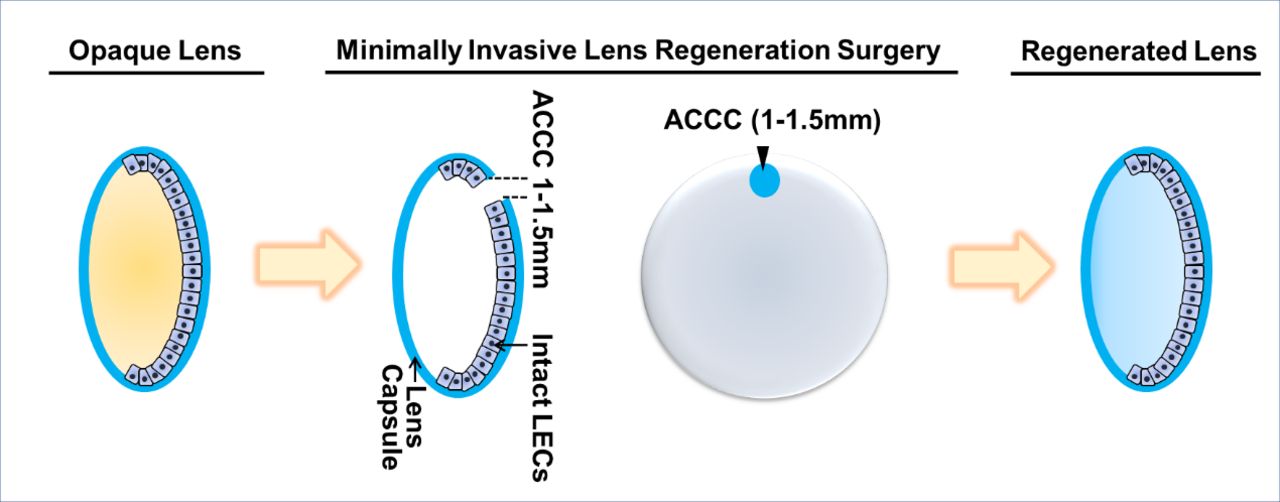
It is difficult to fully restore the physiological function of the lens by using intraocular lens replacement therapy, as the function of the lens, especially accommodation, greatly depends on the cooperation of various components including the lens material, the lens capsule, the zonules and the ciliary muscles. Lin et al have established a novel surgical strategy for infantile cataract designated as minimally invasive lens-content-removal surgery (MILS) for lens regeneration (figure 7).42 The 1–1.5 mm capsulorhexis opening located in the periphery of the anterior capsule of the lens is beneficial to the contraction and closure of the capsulorhexis opening in the early postoperative period and to reduce its influence on the shape of the regenerated lens. In this way, functional lens regeneration originated from the endogenous lens stem cells in 12 children with bilateral congenital cataract can be observed. The MILS provides a new strategy for the reconstruction of lens function. The advantages of the MILS lie in using the proliferation and differentiation ability of the endogenous lens cells to obtain orderly arrangement of lens fibres and transparent lens regeneration in situ.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagram of minimally invasive lens surgery.
However, the MILS is currently only applicable to infants and young children. Regenerative capacity of LECs in human adults is insufficient.59 Using Bromodeoxyuridine (BrdU) labelling, Lin et al found that the number of proliferative cells located at donor eyes’ lens capsule decreases with age.42 So, it is difficult to achieve orderly and transparent regeneration after lens removal in adults. In addition, the biological characteristics of accommodative components outside the lens vary with age and may impact the ability of the eye to accommodate. While Richdale et al reported that the intensity of ciliary muscle contraction induced by per dioptre stimulation is not related to age, Krag et al reported that the mechanical properties of lens capsule changes with age, resulting in decrease of lens flexibility.60–62 How to extend the indications of the MILS surgery to a wider age range warrants extensive basic and clinical research. We need to know about the quantitative changes in biological parameters of the lens and in biomechanical properties of the extralenticular part of the accommodative apparatus with age, so as to provide reference for the intervention or manipulation needed when using the MILS in different age groups of adults. With the rapid development in swept source AS-OCT, three-dimensional image reconstruction technology and algorithms in artificial intelligence, it is possible to build an age-based theoretical model reflecting the main physiological characteristics of the lens and the accommodation process.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was published. The title and level of section headings have been updated as per journal style.
Contributors XR and ZL wrote the first draft of the paper. ZL added clinical content and figures. YL and LL critically reviewed this draft. ZL and LL are the corresponding authors. All authors take responsibility for the content.
Funding This study was supported by the National Natural Science Foundation of China (81873675, 81770905) and the Construction Project of High-Level Hospitals in Guangdong Province (303020102).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.