Article Text

Abstract
Objectives Compare the detection rates of the 2013 Philippine Academy of Ophthalmology (PAO) guidelines for retinopathy of prematurity (ROP) screening and the 2005 PAO-Philippine Pediatric Society guidelines in identifying infants who develop ROP in the 5-year study period in the Philippine General Hospital (PGH). Secondary objectives include determination of ROP prevalence; correlation of gestational age (GA), birth weight (BW) and other risk factors to ROP; and identification of the most common intervention.
Methods and analysis Retrospective cross-sectional study of ROP records between 1 December 2013 and 30 November 2018 from the Medical Retina Service of the Department of Ophthalmology and Visual Sciences of the institution was studied. Variables with p value <0.05 were considered significant. STATA V.14 was used for all analysis.
Results Only 851 of 898 infants screened for ROP were included in the study. Of these 698 would have been screened based on 2005 guidelines. All 118 infants with ROP were identified by both guidelines. Detection rate was higher using the 2005 than the 2013 guidelines (16.9% vs 13.3%, p value=0.0496). ROP prevalence was 9.7%. Among those with ROP, 70% have at least one identified risk factor, topped by sepsis, pneumonia, hyaline membrane disease, blood transfusion and oxygen supplementation. Only 8% required intervention consisting of laser, anti-vascular endothelial growth factor injection, surgery or in combination.
Conclusion In PGH, no infants with ROP were missed using the 2005 recommendations. There was no added benefit of increasing threshold for BW and GA as recommended by the 2013 PAO guidelines. Screening guidelines should, however, be tailored to institutional needs, requirements and experience.
- child health (paediatrics)
- epidemiology
- neovascularisation
- retina
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Screening for retinopathy of prematurity (ROP) helps prevent blindness from ROP.
In 2013, the Philippine Academy of Ophthalmology, after documenting that indeed bigger and older babies can get ROP, revised its (2005) existing guidelines to include bigger and older preterm babies.
Periodic reevaluation is needed by different centres to identify if existing guidelines are sufficient or needs to be modified to reduce the risk of blindness from ROP.
Increasing the threshold for age of gestation and weight for ROP screening will reduce the risk of missed ROP babies, but may entail increasing the number of unnecessary ROP evaluations that can cripple an already burdened health system.
Increasing vigilance about risk factors for developing ROP will increase the detection rate of ROP screening criteria even with lower threshold for age of gestation and birth weight.
Key messages
What are the new findings?
The older 2005 ROP screening guidelines in the Philippines had a higher detection rate than the 2013 guidelines in the Philippine General Hospital (PGH).
No infants with ROP were missed by the 2005 screening guidelines, implying there was no need to increase the threshold for screening in terms of age of gestation and birth weight.
Identified risk factors for ROP included sepsis, pneumonia, hyaline membrane disease, blood transfusion and oxygen supplementation.
How might these results change the focus of research of clinical practice?
A multicentre trial following the protocol used in this study will be undertaken to evaluate if the results of the PGH will be repeatable in centres that increased their threshold for age of gestation and birth weight following the 2013 recommendations. The results of this evaluation can affect the country’s policy recommendations as regards ROP screening.
Existing as well as additional risk factors for ROP developing could be a focus of future research and could be incorporated in existing guidelines as its third criterion, that is, those identified by attending paediatricians to be at risk for developing ROP.
Introduction
Background
Retinopathy of Prematurity (ROP) is a potentially blinding condition affecting premature infants. Published data from developed countries reported 5.5%–20% of childhood blindness were due to ROP.1–5 The American Academy of Ophthalmology estimated this number to be approximately 50 000.1 Development of ROP was attributed to a myriad of factors with low birth weight (BW) and low gestational age (GA) as the most significant risk factors for this condition. ROP leads to disorganised proliferation of the retinal blood vessels causing retinal haemorrhage, scarring and retinal detachment.2 3 Advancements in neonatal care have increased the survival rate of preterm or low BW infants through oxygen supplementation, antenatal steroids, resuscitation and proper nutrition of these infants.3 As more preterm infants survive due to improved management, so does the possibility of developing ROP and potential childhood blindness.
Most international ROP screening guidelines which were revisited stated that infants screened must meet one or more of the following criteria: (1) BW of 1500 g or less, or (2) GA of 30 weeks or less, or (3) infants who are older than 30 weeks or heavier than 1500 g with a complicated postnatal course, or identified by neonatologist as being at risk for developing ROP, especially in the presence of the following risk factors: necrotising enterocolitis, intraventricular haemorrhage, sepsis or bronchopulmonary dysplasia.6 7 While recent publications noted that prevalence and severity of the disease have been decreasing among developed countries,1 the opposite was observed in developing countries including the Philippines, wherein, presence of ROP was reported to occur in neonates with higher BW and later GAs.2 8 In 2017, a call for re-evaluation regarding the practice of retinopathy screening and management was initiated by Clare Gilbert, emphasising individualised management catering to the locality.9
In a local study done by Del Mundo and Chua (2019),6 the investigators found that the leading treatable cause of blindness among children was ROP (47.7%) and cataract (5.8%).7 Effectively screening and treating infants who may be at risk for developing ROP is of utmost importance to prevent blindness.
A local study by Corpus et al8 showed that in a cohort of 105 infants diagnosed with ROP, when only GA and BW in the Philippine Academy of Ophthalmology (PAO)-Philippine Pediatric Society (PPS) 2005 screening criteria were applied (without the third criterion), 16.2% or 17 infants with GA of 33–36 weeks and BW >1500 g would have been missed. Of the 17 missed infants, mean GA was 34 weeks with the oldest at 36 weeks, while mean BW was 1858 g, with the heaviest at 2515 g. Although majority (16 infants) had type 2 ROP and most (15 infants) had identifiable risk factors, there were no risk factors identified for two infants.
Realising that first world ROP screening guidelines may not necessarily apply to our local setting, the Philippine Academy of Ophthalmology PAO recommended new screening guidelines to cover older and bigger infants. The 2013 Philippine guidelines for screening and referral of ROP include any of the following: (1) infants with GA of <35 weeks, or (2) infants with a BW of <2000 g, or (3) infants with GA of ≥35 weeks or BW ≥2000 g which was assessed by the attending paediatrician to have an unstable clinical course or with identifiable risk factors.1
Published data estimate that there were 6.6%–28.3% of infants coming from developing nations who develop ROP but are not detected because they exceeded the international screening cut-off of <32 weeks GA or <1500 BW.8
The 2013 revised guidelines developed by the PAO together with its ROP Working Group (ROPWG), the Philippine Society of Paediatric Ophthalmology and Strabismus and the Vitreoretinal Society of the Philippines were envisioned to have a better detection rate than the old PAO-PPS 2005 guidelines, which was based on the 2003–2004 American Academy of Pediatrician Section of Pediatric Ophthalmology guidelines,10 that screened younger (less than 32 weeks) and smaller (less than 1500 g) preterm babies. The revision targeted ‘zero infants blind from ROP’. Both guidelines had a third often overlooked criterion that encompasses all with unstable course and/or neonatal risk factors regardless of the baby’s GA or BW.
Increasing the cut-off GA and BW increases the number of infants requiring ROP evaluations. ROP examinations require topical cycloplegic–mydriatic that may have systemic side effects. According to a study done by Kremer et al in 2019, systemic absorption of topical mydriatic agents was associated with clinically significant and life-threatening side effects among infants undergoing ROP screening. The authors noted significant changes in heart rate, blood pressure, increased prevalence of necrotising enterocolitis and apnea.11 A local study done by Mesina-Bayana and Arroyo (2005) stated that commercially available topical cycloplegic–mydriatic agents did not have any significant side effects among adult Filipino patients12; however, these preparations are of higher concentration than needed for ROP screening purposes and current packaging is for adult dosing not neonatal dosing.11 The actual conduct of the screening may in some instances cause unstable vital signs in a fragile neonate, with some authors highlighting reduction in heart rate due to the oculo-cardiac reflex in approximately 10% of infants following ROP screening.11 Unwarranted ROP examinations also burden the health system, not only its physicians, but also its government-subsidised insurance system—the Philippine Health Insurance Corporation. As such, this study aimed to find out if there was a significant difference between the detection rates for ROP of the two guidelines with differing cut-offs in terms of GA and BW. Being initially part of a multicentre study that would have prospectively evaluated the new 2013 guidelines, the institution adopted the 2013 Revised Philippine Guidelines for ROP screening soon after its publication. Five years hence, we now have the opportunity to compare the detection rates of the new guidelines vis-à-vis the 2005 PAO-PPS screening guidelines using the same patient cohort.
This study compared the detection rates of the 2013 Revised Philippine Guidelines and the 2005 PAO-PPS Screening Criteria in identifying infants who develop ROP. It also determined the incidence of ROP in the Philippine General Hospital (PGH) using both guidelines, and established the correlation between GA, BW and presence of risk factors with the development of ROP either on initial screening and/or subsequent follow-up. Lastly, the most common intervention or plan on screening and follow-up were also identified.
Operational definition of terms and acronyms
Retinopathy of prematuriy (ROP)
A condition in which there is abnormal growth of retinal blood vessels that may sometimes lead to blindness.
Plus disease
A degree of dilation and tortuosity of the posterior retinal blood vessels meeting or exceeding that of a standard photograph.13
Type 1 ROP
Defined as zone I, any stage ROP with plus disease; zone I, stage 3 ROP without plus disease; or zone II, stage 2 or 3 ROP with plus disease.13
Type 2 ROP
Defined as zone I, stage 1 or 2 ROP without plus disease or zone II, stage 3 ROP without plus disease.13
Aggressive posterior retinopathy of prematurity (APROP)
APROP, characterised by severe plus disease, flat neovascularisation in zone 1 or posterior zone 2, intraretinal shunting, haemorrhages and a rapid progression to retinal detachment.14
Gestational age (GA)
Age in weeks of the infant based on ultrasound (preferred) or the last menstrual period.
Birth weight (BW)
Weight in grams of the infant when born.
Corrected age
GA plus chronological age of the infant.
Anti-vascular endothelial growth factor (anti-VEGF)
Drug that is administered through the intravitreal route to decrease the concentration of VEGF, thus, minimising vasoproliferation.
Materials and methods
This study was a single centre, cross-sectional, hospital-based review of medical records, conducted in a tertiary hospital, focusing on the Medical Records of the Medical Retina Service of the Department of Ophthalmology and Visual Sciences (DOVS) and the neonatal intensive care unit (NICU) of the Department of Pediatrics of the PGH. Study used records of patients who have been screened by the Medical Retina Service for ROP of the DOVS, referred by the Department of Pediatrics, particularly the NICU of the PGH from 1 December 2013 to 30 November 2018.
Inclusion criterion was the presence of complete medical records of patients referred to the Medical Retina Service for ROP screening assessed by a Medical Retina consultant and/or Retina fellow certified to screen for ROP. The screening criteria were based on the 2013 recommended Philippine guidelines for screening and referral of ROP. All available records of infants screened for ROP from 1 December 2013 to 30 November 2018 from the institution were included. Records of patients excluded from the study were either due to (1) patients who were initially screened before the study start date of 1 December 2013 and (2) with incomplete medical records.
For the descriptive analysis, the means and standard deviation (SD) were used to summarise variables with normal distribution while the medians, first and third quartile, minimum and maximum observations were used to summarise variables with non-normal distribution. For the inferential analysis, a Student’s t-test or analysis of variance was used to compare means. A chi-square (χ2)test was used to determine any association between ROP and dichotomised clinicodemographical characteristics (eg, GA, BW and presence of risk factor). A simple logistic regression analysis was used to determine the variables which were independent predictors of ROP while a multiple logistic regression analysis was done to determine the predictors of ROP while accounting for the effects of other variables (ie, confounders). A variable with a p value of less than 0.20 was included in the multiple logistic regression analysis. The detection rates of infants who develop ROP using the two screening criteria were obtained and compared with one another. Variables with p value of less than 0.05 in all analyses were considered significant. STATA V.14 (Statacorp) was used for all analysis.
Ethical considerations
Patient confidentiality and privacy
Records reviewed were assigned control numbers by the data collector and did not bear the patient’s personal information. Coded identification numbers were assigned to each record. No written or informed consent was obtained; patient information was anonymised protecting sensitive health information and privacy. In accordance with the Philippines National Ethical Guidelines of Health and Health-related Research 2017, a waiver of informed consent was obtained from the Research Ethics Board panel.
Data storage
Data were stored in both physical (hard) copy and soft copy. For the soft copy, data were stored in a password protected folder in a computer in the Department of Ophthalmology of the institution and were accessible only to the primary investigator, data abstractor and statistician. All copies will be deleted after 5 years of publication of results. Physical copies of the collected data are stored in a cabinet under lock and key in the Department of Ophthalmology and Visual Sciences of the institution and is accessible only to the primary investigator, data abstractor and statistician. All physical copies will be shredded after 5 years of publication of results. The data obtained from the research will remain available to the Department of Ophthalmology and Visual Sciences of the tertiary government hospital.
Patient and public partnership
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Research funding
This research recieved a partial publication grant after completion of the study from the University of the Philippines Medical Alumni Society in America (UPMASA). No other specific grant from any funding agency in the public or commerical sectors were received.
Results
Patient characteristics
Data from 851 of 898 records screened by the Medical Retina Service for the presence of ROP from 1 December 2013 to 31 November 2018, referred by the Department of Pediatrics were included in the study. Excluded were 47 incomplete records. Table 1 summarises the demographic data and frequency of ROP, whereas figure 1 plots all 851 babies screened on the basis of GA and BW.
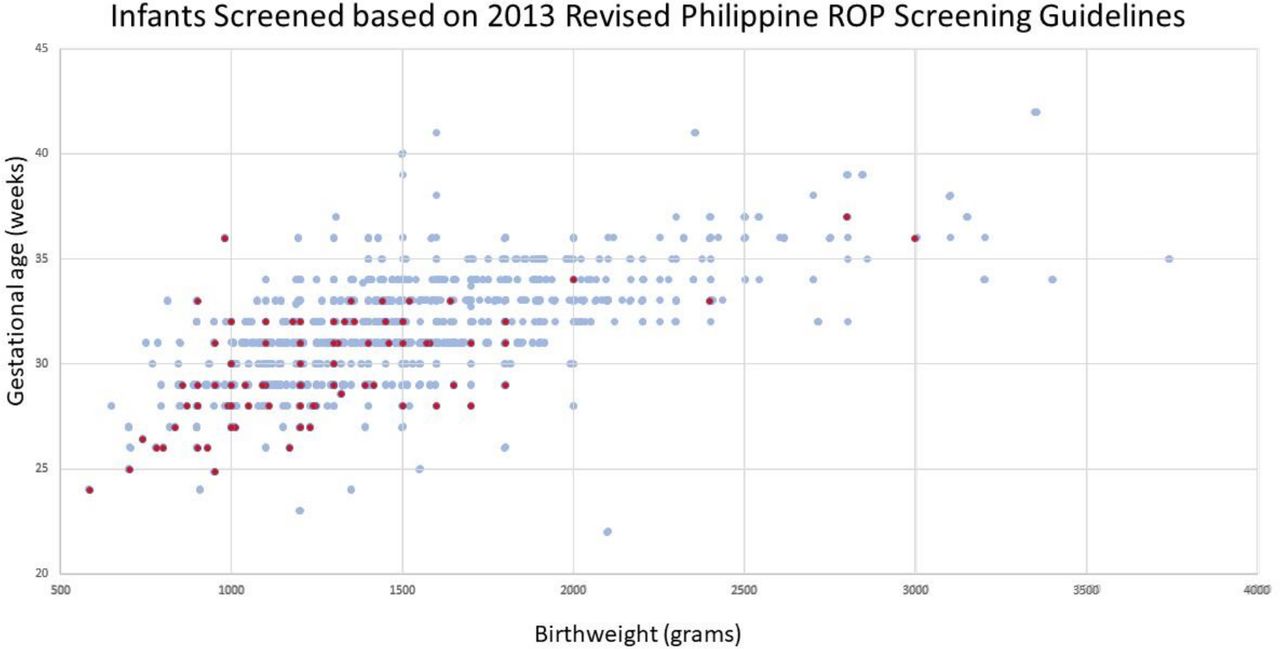
{kind=link}
Distribution of infants with retinopathy of prematurity (ROP) screened.
Demographics of infants and frequency of retinopathy of prematurity (ROP) in the study
Detection rate of 2013 revised Philippine ROP screening guidelines and the 2005 PAO-PPS ROP screening guidelines
The number of ROP patients screened using the old 2005 PAO-PPS ROP screening guidelines is a subset of the patients screened using the 2013 Revised Philippine ROP screening guidelines. Both guidelines had the same yield as to the number of ROP cases identified. The 2005 guidelines, however, had a better overall detection rate of 16.9% compared with 2013 guidelines at 13.3% since the number referred for screening was less using the 2005 guidelines (698 vs 851 infants) (table 2). This difference was statistically significant (p=0.0496). The presence of the third clause, that is, infants with GA of ≥32 weeks or BW ≥1500 g, having an identified risk factor for ROP and/or having a stormy course, identified the infants who were not included by the first two criteria consisting of GA and BW.
Detection rate of retinopathy of prematurity (ROP) using the 2005 Philippine Academy of Ophthalmology (PAO)-Philippine Pediatric Society (PPS) ROP screening guidelines compared with the 2013 Revised ROP Philippine Screening Guidelines
Prevalence of ROP
Of 851 patients screened, 118 had ROP for a prevalence rate of 13.86%. Seven of 118 patients (5.9%) had regressed ROP, 29 (24.6%) had ROP stage 1, 26 (22.9%) had ROP stage 2, 33 (28%) had ROP stage 3, 8 (6.8%) had ROP stage 4A, 4 (3.4%) had ROP stage 4B, 11 (9.3%) had ROP stage 5 (online supplemental table 1). Fourteen (11.9%) of them developed aggressive posterior ROP:<29 weeks: 4 babies, 29–30 weeks: 6 babies, 31–32 weeks: 3 babies and 1 baby at 33–34 weeks (online supplemental table 2). APROP was observed in infants with low BW and GA. Thirteen of 14 APROP (92.3%) occurred in babies less than 32 weeks GA with BW less than 2000 g (online supplemental table 4).
Supplemental material
Supplemental material
Supplemental material
Profile of babies with ROP
Among the 118 with ROP, 106 (90.2%) of ROP of any stage were found in babies born within 32 weeks GA or less, and in 103 (87.3%) of those who had a BW of less than 1600 g (details in online supplemental table 1). The mean GA and BW were 29.7 weeks (±2.46 weeks) and 1237.8 g (±416.5 g).
Severity of ROP
There was an inverse relationship between prevalence and severity of ROP, and GA and BW of the infant. One-hundred fifteen (97.5%) of 118 with ROP were seen among those younger than 34 weeks and 102 (86.5%) of ROP were seen among those weighing less than 1600 g. The ROP type showed that ROP severity decreased as the infants became older and heavier (table 3).
Frequency distribution of infants according to type of retinopathy of prematurity (ROP) at different gestational age (GA) and birth weight (BW) (N=851)
Risk factors among infants with ROP
Subjects were classified according to the presence of an identified risk factor known to cause ROP or having a ‘stormy course’ (table 4). The presence of a risk factor, together with low BW and younger GA infants, demonstrated a trend towards severe ROP, which improved as BW and GA increase.
Frequency distribution different types of retinopathy of prematurity (ROP) stratified according to presence or absence of risk factors, at gestational age (GA) and birth weight (BW) used in 2005 screening criteria (N=851)
GA and BW
GA in weeks (z=−4.36*, CI −0.35 to −0.13, p<0.001), BW in grams (z=−2.91*, CI −0.001 to −0.004, p=0.004) and presence of risk factor/s (z=3.89*, CI 3.95 to 9.80, p<0.001) were statistically significant as causing severe ROP. The negative z values of GA and BW connote that increasing GA and BW reduces the risk of ROP, while positive z value of presence of risk factor/s suggests that as risk factors increase, the risk of ROP likewise increases (online supplemental table 3).
Supplemental material
Among those diagnosed to have ROP, 82 (69.5%) have at least one identified risk factor which was known to cause ROP. In addition to younger age of gestation and lower BW, oxygen supplementation, blood transfusion and conditions such as sepsis, pneumonia, hyaline membrane disease and congenital heart defects were statistically significant in the development of ROP. Other risk factors identified that did not reach statistical significance were the following: mechanical ventilation, prolonged admission, multiple gestation, respiratory distress syndrome, premature rupture of membranes and low Appearance, Pulse, Girmace, Activity, and Respiration (APGAR) score. Among the risk factors identified, sepsis increased the chance of developing ROP 40-fold, followed by presence of pneumonia, hyaline membrane disease and need for blood transfusion which increased the risk of developing ROP by 30-fold, and the need for oxygen supplementation by 15-fold.
By including the third criterion of the 2005 PAO-PPS ROP screening guidelines (ie, those with risk factors or identified by paediatrician as having a stormy course), no infant with ROP was missed, regardless of BW or GA.
Treatment plans
Treatment plans on initial consultation were summarised based on the ROP type (as defined by Early Treatment for Retinopathy of Prematurity (ETROP) study) at presentation (refer to online supplemental table 5). Infants with severe ROP (stages 4A, 4B and 5, and APROP) were treated with laser indirect ophthalmoscopy (LIO), combination of anti-VEGF injection and LIO, retinal surgery, or were advised regarding the poor prognosis of the condition. Among those with severe ROP (23), 8 (34.8%) were advised to undergo surgery. Among those with type 1 ROP (21), treatment advise consisted of LIO alone (9 (42.9%)) or in combination with anti-VEGF (9 (42.9%)). Among those screened (851), 786 (92.4%) did not require any active intervention. Those without ROP at initial consultation (127 914.9%) were referred to the Paediatric Ophthalmology Service for continuation of care.
Supplemental material
Of the 118 patients with ROP, 89 (75.4%) received treatment or completed the necessary follow-up (refer to online supplemental table 5).
Discussion
In this cohort, 118 of infants with ROP were babies with BW heavier than 2000 g and GA older than 35 weeks, the heaviest being 3000 g and the oldest being 37 weeks. The average BW of infants with ROP was 1237.8 g (±416.5 g) while the average GA was 29.7 weeks (±2.46 weeks). These babies were lighter and younger than those in earlier local15–17 and Asian studies.4 8
The PAO and PPS developed ROP screening guidelines in 2005 which was largely based on international ROP screening guidelines at that time,10 namely: (1) BW <1500 g, or (2) GA <32 weeks, or (3) infants who are 32 weeks and/or older 1500 g or heavier with a complicated postnatal course, or identified by neonatologist as being at risk for developing ROP.
Several studies however showed older and heavier infants coming from Third World countries still developing ROP,2–5 8 18 including a local study done by Corpus et al (2013).8 In that study, two infants with ROP were missed based on the 2005 PAO-PPS guidelines. One infant had a BW of 1875 g and GA of 33 weeks, while the other had BW of 2200 g and GA of 34 weeks. Neither of them had risk factors.8
With the objective that no infant with ROP will be missed, the ROPWG of the PAO published the 2013 Revised Philippine Guidelines for screening and referral of ROP: (1) infants with GA <35 weeks, or (2) infants with a BW <2000 g, or (3) infants with GA of ≥35 weeks or BW ≥2000 g which was assessed by the attending paediatrician to have an unstable clinical course.1
This study was able to screen 851 infants based on the 2013 guidelines and was able to identify 118 infants with ROP. The same 118 infants were similarly identified with the old 2005 PAO-PPS screening guidelines. The glaring difference between the two protocols was the number of infants unnecessarily screened by increasing the cut-off BW and GA based on the 2013 guidelines. The detection rate was higher in the 2005 PAO-PPS guidelines (16.9%) compared with the 2013 guidelines of 13.3%. This was a crucial finding, favouring the use of the 2005 PAO-PPS screening guidelines on the basis of higher detection rate and no missed infants. Unnecessary ROP screening for the heavier and older infants without risk factors would also be avoided and would reduce the burden on the parents/guardians, and the health system, including hospital resources, physician manpower, and the national health insurance system.
The prevalence of ROP using both 2013 and 2005 guidelines would be the same at 13.86% since they were able to identify the same number of cases (118) among the preterm infants referred for screening (851). Available data from referrals for ROP screening from the Department of Pediatrics in this institution were obtained from 2015 to 2018 (774 infants). Of these infants, 75 were diagnosed with ROP giving an prevalence of 9.7%. This was significantly less than the available local data on prevalence of ROP (13.8%–47.5%) published between 2010 and 2017.8 15–17 An earlier study by Arroyo et al15 from the same institution had a prevalence rate of 47.5%; however, it should be noted that the increased prevalence may be due to the sampling. The prevalence was based on the infants with ROP compared with all infants screened for ROP which included infants born outside the tertiary care facility of PGH and already high-risk infants. The current study only included infants managed from birth in the NICU of this institution.
In assessing the prevalence of ROP, a recent study by Lazo and Corpus-Velasquez19 could be better compared with the current study because the cohort of patients came from the same institution. The current study obtained an prevalence rate of 9.7% which was less than the 25% obtained by Lazo.19 The decrease in prevalence may be attributed to better understanding of the mechanism of ROP, its risk factors and improved resuscitation techniques of premature infants.
Risk factors which were statistically significant have also been historically known to influence development of ROP, these are: younger GA, low BW, oxygen therapy, pneumonia, sepsis, congenital heart defects, hyaline membrane disease and blood transfusion.20 The severity of ROP was inversely proportional to GA and BW and was directly proportional to presence of 1 or more risk factors. Younger GA and presence of risk factors influence severity of ROP more than that of low BW. Other risk factors identified were multiple gestation, respiratory distress syndrome, mechanical ventilation, prolonged admission, hyperthyroidism and low APGAR score. The risk factors in the latter list, however, were not statistically significant in this study.
The initial treatment plans for the infants who were diagnosed with ROP depended on the severity of ROP at presentation. Patients with severe ROP underwent surgery, LIO or anti-VEGF injections alone or in combination. Some cases did not undergo any treatment since they had poor prognosis and further risk of intervention did not outweigh the benefits.
Chan and Herrera-Arroyo21 investigated outcomes of LIO for ROP in the same institution. Poorer outcomes were noted compared with published data (success rate of 60% vs 90%).21 Limitation and poor outcomes of this study were attributed to lack of uniformity in data collection, and insufficient identification of prenatal and perinatal risk factors. This stresses the importance of proper documentation of these risk factors from all involved in the care of preterm infants in identifying those requiring ROP screening.
In conclusion, the 2005 PAO-PPS Guidelines for ROP Screening, if used properly, has a higher detection rate than that of the 2013 PAO Revised Philippine Screening Guidelines. No infant with ROP would be missed if the paediatrician/neonatologist can identify risk factors and refer these infants promptly. Referral and screening protocols for ROP should be based on the institution. As seen in an earlier study by Arroyo et al15 done almost 10 years apart in the same institution, the prevalence of ROP is decreasing, possibly due to improved understanding of the disease as well as better management by attending paediatricians. Risk factors which greatly affect the development of ROP should not just be identified, but also specified since there are still grey areas in terms of the dose of oxygen therapy, and duration of stay in the ICU, among others. Revisiting and adjusting the screening guidelines of an institution, with proper lines of communication between the ophthalmologist and the paediatrician/neonatologist, would reduce the number of unnecessary screening of infants.
Recommendations
The authors recommend reevaluation of every institution’s ROP screening practices with regards to GA, BW and risk factors that have been identified by existing criteria and modified for their own use as necessary. Risk factors, such as manner of oxygen supplementation, oxygen levels and duration, should be properly quantified by referring paediatricians/neonatologists so that future studies may investigate these, and appropriate resuscitation measures may be set.
Limitations of the study
Since the study is retrospective, no further intervention was done for both the mother and infant. Only the information available at the time of data collection was included and the possibility of risk factors, both maternal and infantile, may have been missed.
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors planned the study. JATP collected and analysed the data and submitted the study. All authors wrote the discussion.
Funding This research received a partial publication grant after completion of the study from the University of the Philippines Medical Alumni Society in America (UPMASA). No other specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.