Article Text

Abstract
Objective Patients with diabetic macular oedema (DME) are known to have significantly greater medical treatment burden than patients with non-DME. Frequent injections and office visits can have a substantial impact on patient adherence and quality of life. This analysis assesses the impact of the 0.19 mg fluocinolone acetonide (FAc) implant (or injection) on treatment burden and practice resource utilisation in patients with DME.
Methods and analysis This study is a single-centre retrospective chart review of 30 eyes (23 patients) that received a single FAc implant. Data was collected for a 12-month period pre-injection and post-injection of the FAc implant. Primary outcomes included the frequency of injections and ophthalmology office visits. Secondary outcomes included visual acuity (VA), intraocular pressure (IOP) and central subfield thickness (CSFT).
Results The injection frequency significantly decreased from one injection every 2.6 months pre-injection to one injection every 8.8 months post-injection of the FAc implant (p<0.001). Sixty-three percent of the subjects did not require additional injections post-FAc implant. The mean number of ophthalmology office visits significantly decreased from 12.7 visits pre-FAc to 9.3 visits post-FAc implant (p<0.001). The mean VA (p=0.24) and CSFT (p=0.39) showed a mild numerical improvement that was not statistically significant. Thirty-seven percent of the eyes required additional IOP lowering drops. No eyes required incisional glaucoma surgeries.
Conclusions The FAc implant significantly decreased the treatment burden and improved practice resource utilisation while maintaining or improving VA and CSFT. IOP events were mostly well-controlled with drops and no eyes required incisional glaucoma surgery.
- macula
- treatment medical
- vision
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The fluocinolone acetonide (FAc) implant improves visual acuity and optical coherence tomography central subfield thickness in patients with diabetic macular oedema (DME). When used according to the US label, the FAc implant mitigates the risk of uncontrolled intraocular pressure responses.
What are the new findings?
The FAc implant decreases the frequency of ophthalmology and retina-related office visits without a significant change in monitoring visits in patients with DME.
How might these results change the focus of research or clinical practice?
A lower treatment burden may reduce the challenges associated with monthly treatment visits in patients with diabetes who need frequent healthcare provider visits.
Introduction
The International Diabetes Federation estimate that some 425 million people worldwide, or 8.8% of adults aged 20–79 years of age, are estimated to have diabetes with numbers projected to rise to 629 million people by 2045 based on current trends.1 Diabetic macular oedema (DME) is one of several ocular manifestations of diabetes mellitus. It is one of the main causes of vision loss among patients with Type II diabetes globally2 affecting around 6.8% of patients with diabetes worldwide3 and if left unmanaged, more than half of patients will lose ≥2 lines of visual acuity (VA) over a 2-year period.4 Hence, this future projection indicates that DME is set to increase as a public health problem driven by factors such as aging, increased prevalence of diabetes, longer duration of diabetes and an older age at onset.5
Intravitreal injections of corticosteroids or anti-vascular endothelial growth factors (anti-VEGFs) are proven treatments for the management of DME. Randomised control trials involving anti-VEGF therapy for DME show that a substantial percentage of patients, up to 65% reported in Protocol T,6 will continue to have residual oedema with anti-VEGF treatments despite ongoing treatment regimens.7 8 There is also the practical aspect of delivering the required number of intravitreal injections in real-world practise as used in randomised controlled trials (RCTs). Indeed, in a real-world setting, a monthly or bimonthly anti-VEGF injection schedules may not be achievable.9 10
In addition to injection treatments, patients with diabetes also have a heavy non-ophthalmic medical treatment burden due to comorbidities and complications that can require frequent doctor’s appointments, emergency department visits and hospitalisations. Patients with DME have an even heavier treatment burden. Studies have shown that patients with DME, on average, have one doctor appointment every 2 weeks.11 Furthermore, for every injection visit, greater than 50% of working patients need to take a day off, greater than 70% of patients need care-taker assistance and more than half of patients have anxiety for at least 2 days leading up to ocular injection visits. An intensive injection regimen can have a substantial negative impact on a patient’s time, quality of life and adherence to treatment.12
Decreasing the treatment burden of patients with DME, while maintaining or improving functional and anatomical outcomes with minimal side effects, still remains an unmet need and important for the patient’s quality of living.5 With this in mind, the fluocinolone acetonide (FAc) implant (ILUVIEN; Alimera Science, Alpharetta, Georgia, USA) uses a sustained release technology with near zero order kinetics that delivers continuous treatment with corticosteroid for up 36 months; thus, with a single injection, it may work to reduce treatment burden over the longer-term (ie, up to 3 years).10 This contrasts with other pharmacotherapies approved for DME in the USA that are injected between once every one to four months. Therefore, the FAc implant may help reduce intravitreal injections and treatment visits, and this may help to improve the patient’s adherence to the treatment regimen, quality of life and also improve the efficiency of the clinic.13
Large real-world studies in Europe and the USA demonstrated a significant reduction in injection burden after receiving the FAc implant while maintaining or improving VA and optical coherence tomography (OCT) central subfield thickness (CSFT).14 15 There are, however, little or no studies assessing its impact on patient visits and also practice resource utilisation (based on ophthalmic visits and injection burden) so we now examine these aspects in our clinical practice.
Materials and methods
This is a single-centre retrospective analysis of patients who received 0.19 mg FAc implant on or before 18 November 2016 at Cincinnati Eye Institute, Ohio, USA. An IRB waiver was obtained. A total of 132 eyes of 96 patients were identified using CPT4 code for FAc implant based on patients’ medical records. Forty-three eyes were excluded due to current sponsor trial participation.14 Forty-eight eyes were excluded for having insufficient data pre-injection or post-injection of the FAc implant of less than 1 year as of the last day of the data collection, which was 19 June 2017. Eleven eyes were excluded for having concomitant non-diabetic retinal conditions. A total of 30 eyes of 23 patients were included in the final analysis. All 30 eyes received treatment for DME for 12 months prior to the administration of the FAc implant.
Baseline characteristics were collected from the office visit notes taken on the day of injection of the FAc implant. These included age, sex, duration of DME diagnosis, diabetic retinopathy status (non-proliferative diabetic retinopathy (NPDR) or proliferative diabetic retinopathy (PDR)), lens status, cataract grading, vitrectomy status, pan-retinal photocoagulation (PRP) status, intraocular pressure (IOP) lowering medications, previous glaucoma procedures and other pathologies that may affect VA, IOP or CSFT including but not limited to glaucoma, epiretinal membrane, retinal vascular obstruction, age-related macular degeneration and posterior uveitis. These data points were also obtained from the clinic visit 12 months after injection of the FAc implant.
The primary outcome measure was treatment burden, which was assessed in two different categories: injection burden and ophthalmology visit burden, being a measure of practice resource utilisation, both of which were tabulated for the 12 month periods before and after injection of the FAc implant. Clinic visits were identified as belonging to four different subcategories based on the purpose of the visit including retina, cataract, glaucoma and other visits. Retina visits were defined as visits to a retina specialist for monitoring and/or treatment of DME and/or diabetic retinopathy. Cataract visits were defined as consultation, preoperative or postoperative visits for cataract surgeries. Glaucoma visits were defined as visits for assessment and/or management of IOP or glaucoma. Other visits were any appointments not falling into the previous categories such as an acute visit for conjunctivitis. Retina visits were counted as treatment or monitoring visits depending on whether treatment was performed. Treatment was defined as injections or laser.
Secondary outcome measures were VA, IOP and CSFT and were extracted from each clinic encounter during a 24-month period spanning 12 months before and 12 months after injection of the FAc implant. Snellen VA was collected from the chart and converted to Early Treatment Diabetic Retinopathy Study (ETDRS) letters. When pinhole VA was recorded, this value was collected instead of VA without pinhole. IOP was obtained with either Goldmann applanation or Tonopen. If both were obtained during the same visit, Goldmann applanation reading was recorded over Tonopen reading. CSFT was obtained with Heidelberg Spectralis OCT. The standard deviation (SD) of CSFT for the 12 months before and after injection of the FAc implant were calculated to assess the stability of the OCT signal over time.
The number and type of DME treatments (intravitreal injection and laser) were also collected. These were broken down into intravitreal bevacizumab (IVA), ranibizumab (IVL), aflibercept (IVE), triamcinolone acetonide (IVT), dexamethasone (IVO), focal laser photocoagulation (FLP) and PRP.
Statement of ethics
A waiver was obtained from the IRB as this was a retrospective audit of the use of the FAc implant in general practice. All data are anonymised and confidential and in compliance with the Declaration of Helsinki.
Patient involvement
Patients were not involved in the design of this study.
Statistical analysis
Data from all eyes were used in the analysis. For continuous variables, such as VA and retinal thickness, the observed and change from baseline values were summarised descriptively (mean, SD). Student’s one sample t-test was used to determine the statistical significance of the change from baseline values versus the null hypothesis of zero. The monthly injection burden for each eye was calculated as the number of DME treatments administered to the eye divided by the amount of available follow-up (in months) for the eye. The monthly treatment burden pre-FAc and post-FAc implant administration were summarised descriptively (mean, SD) and the inverse was calculated to determine the frequency of treatments. The number of ophthalmology office visit pre-FAc and post-FAc implant administration were summarised descriptively (mean, SD). A paired t-test was used to determine the significance of the difference, pre-FAc versus post-FAc implant administration, of the monthly treatment and appointment burdens. A variability analysis of the mean CSFT was performed by comparing the average SD of the mean CSFT pre-injection and post-injection of the FAc implant. Statistical significance was declared at a type 1 error rate of 0.050. Statistical calculations and analyses were performed using SAS for PC, V.9.3 (SAS, Cary, North Carolina, USA).
Results
There were 30 eyes of 23 patients included in our study with a mean age of 67.3 years old; 60% were female and 40% were male. The subjects had DME for a mean of 5.6 years (range, 2–13 years); 63% had PDR and 37% had NPDR; 57% had prior PRP and 43% had prior vitrectomy.
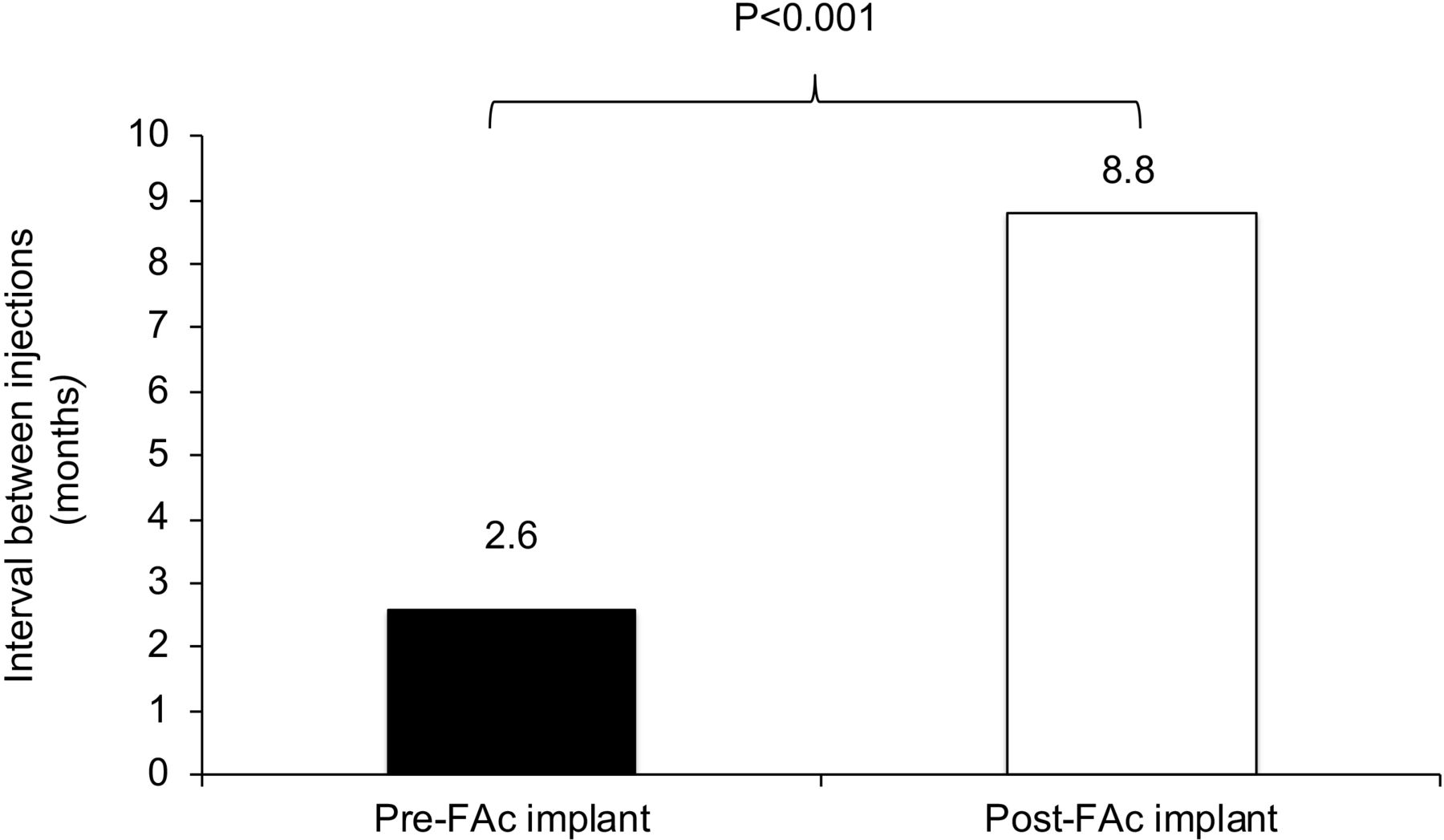
The mean number of intravitreal injections for DME treatments per 12-month period showed a significant reduction (70%) from 4.7 injections pre-FAc implant to 1.4 injections post-FAc implant (p<0.001) and 63% of the subjects did not require additional injections post-FAc implant. In terms of injection-free interval, this represents a change from 1 injection per 2.6 months pre-FAc implant to 1 injection per 8.8 months post-FAc implant (p<0.001) (figure 1).
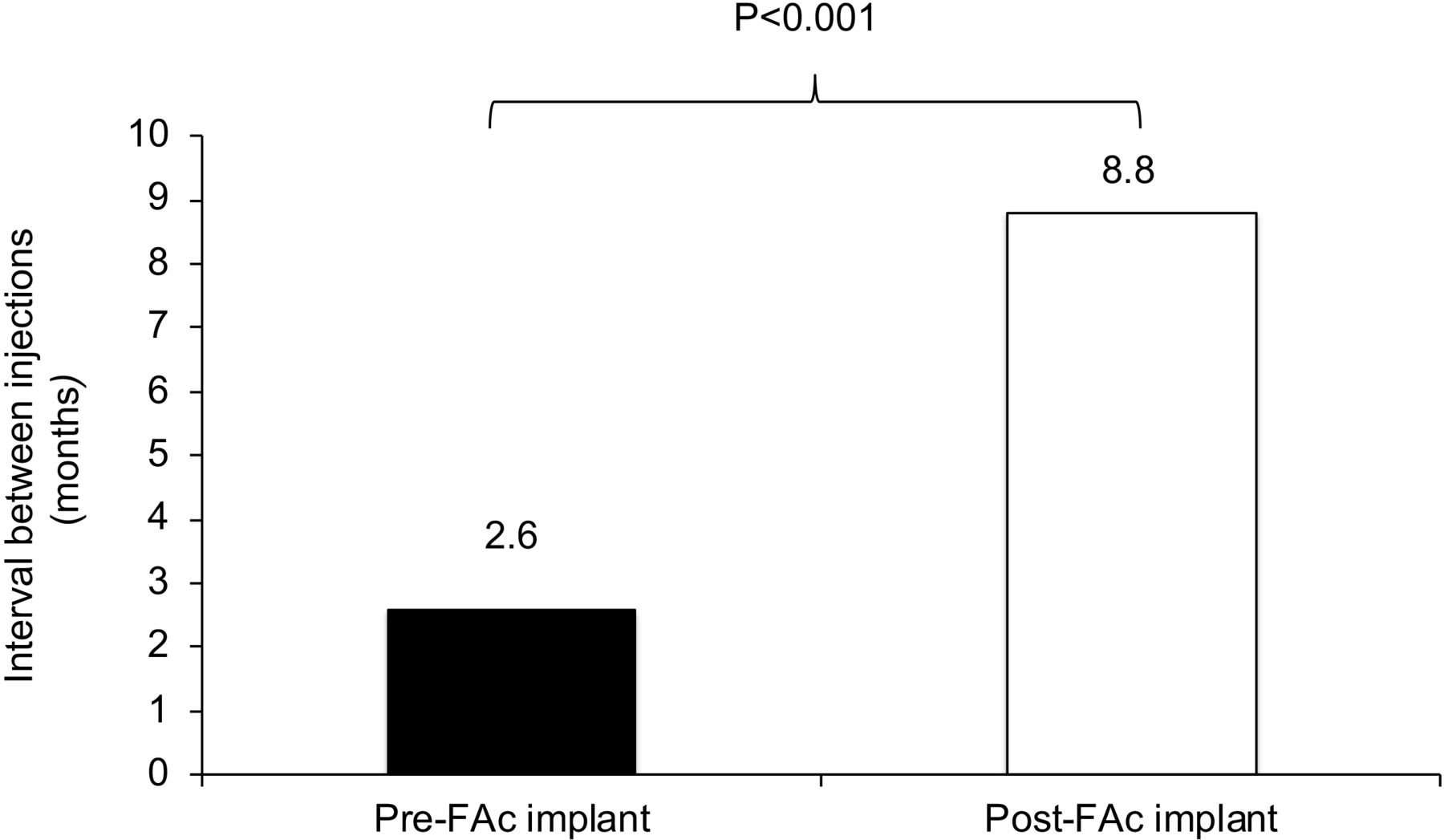
Injection burden and the interval between injections pretreatment and post-treatment with the FAc implant. FAc, fluocinolone acetonide.
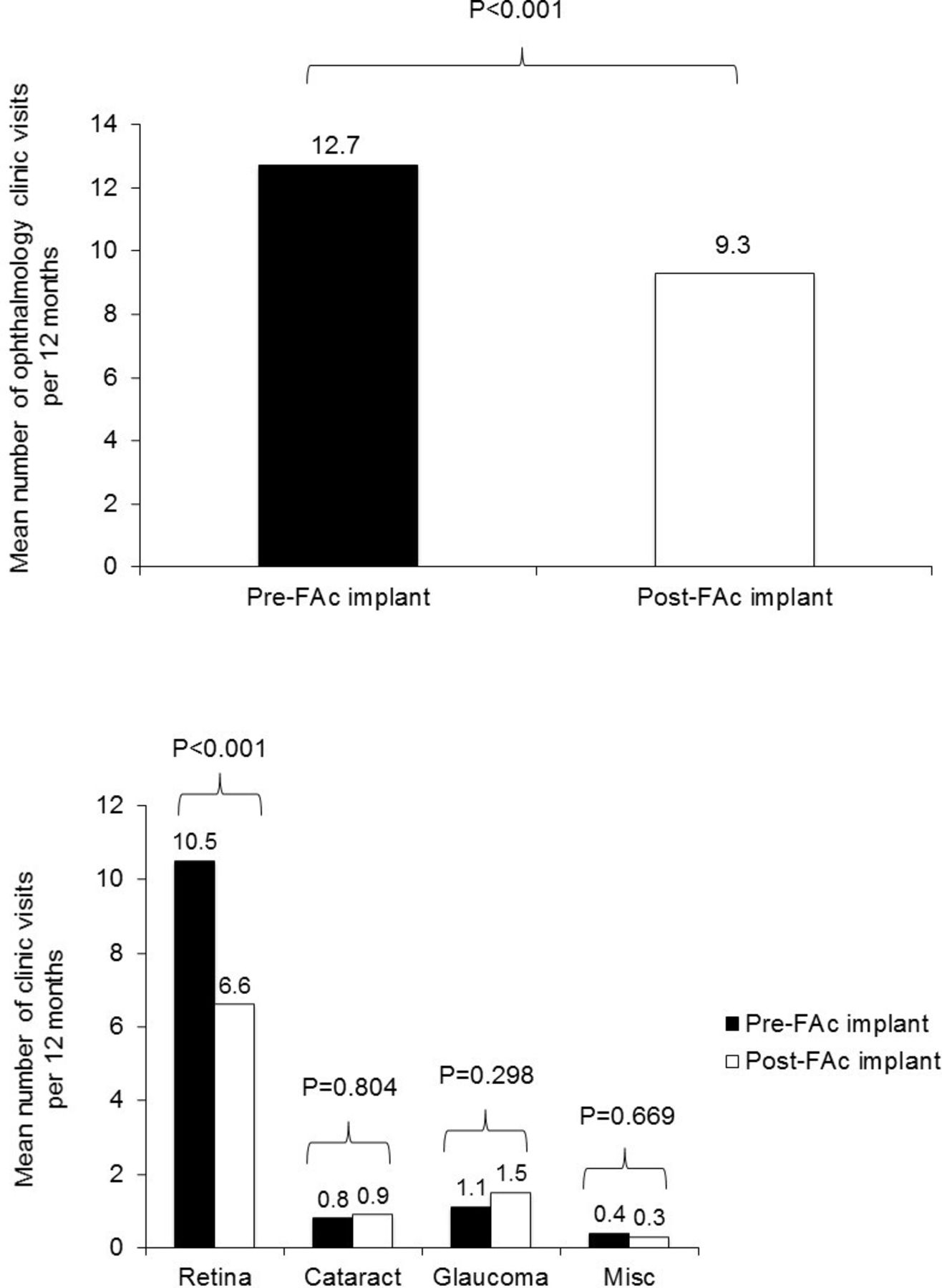
The mean number of ophthalmic visits per 12-month period was reduced by 27%, from 12.7 pre-FAc implant to 9.3 post-FAc implant (p<0.001) (figure 2, top panel). The reduction in ophthalmic visits was due to a large reduction in retina visits (37%), from 10.5 pre-FAc implant to 6.6 post-FAc implant (p<0.001). There was no meaningful change in cataract, glaucoma or miscellaneous visits (figure 2, bottom panel).

Mean number of ophthalmology-related clinic visits pre-injection and post-injection of the FAc implant over a 12-month period (top panel) and by ophthalmology specialty (bottom panel). FAc, fluocinolone acetonide.
There was a large reduction in treatment visits (70%), from 4.93 pre-FAc implant to 1.50 post-FAc implant (p<0.001) within the 12-month pre-FAc/post-FAc implant timeframe. There was no meaningful change in monitoring visits (p=0.47) (figure 3).
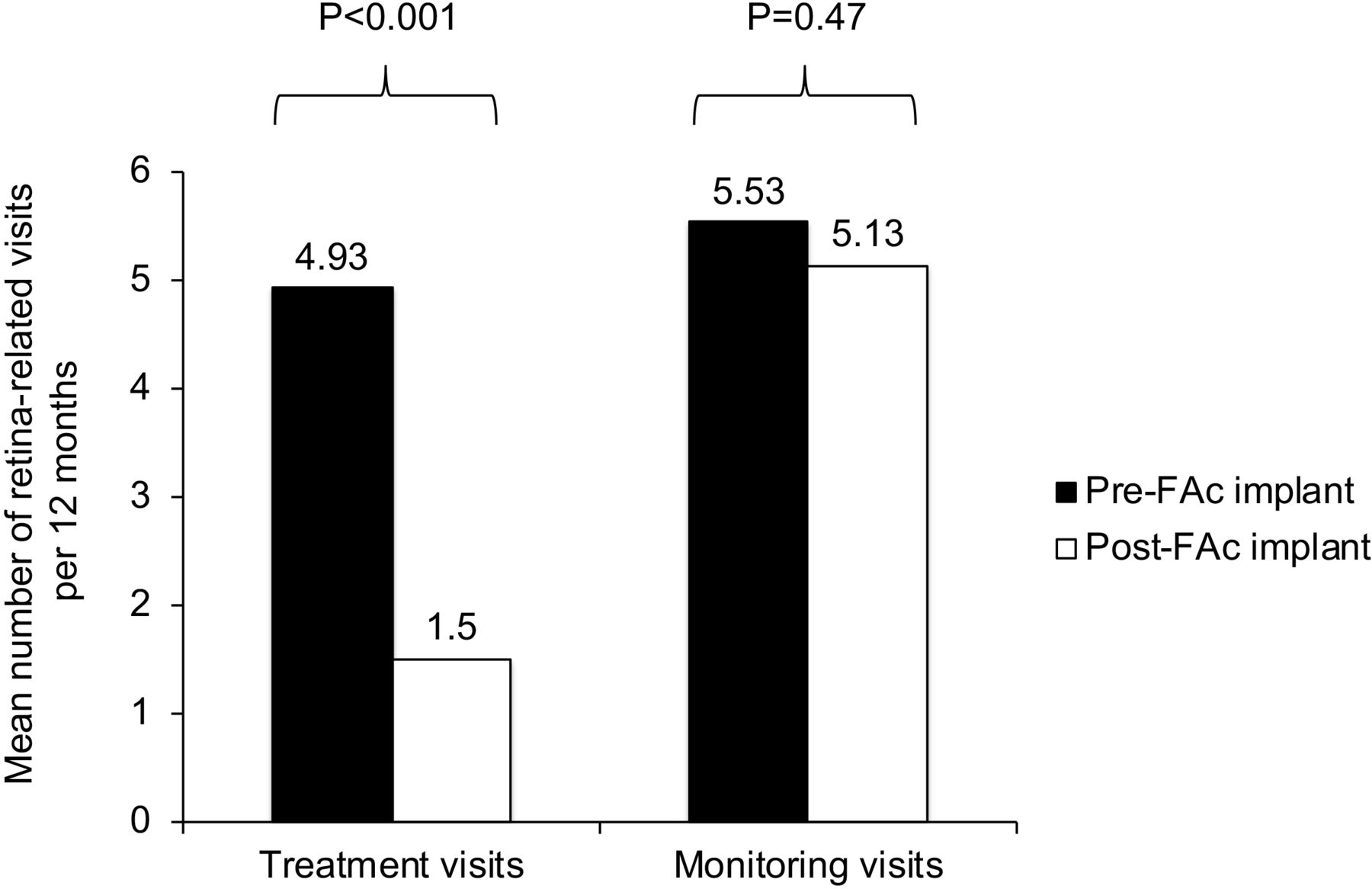
Retina-related visits showing the burden of treatment and the burden of monitoring visits pre-injection and post-injection of the FAc implant. FAc, fluocinolone acetonide.
Secondary outcomes including the mean VA, CSFT and IOP did not show a statistically significant change. There was a modest increase in mean VA from ETDRS letter score of 60 pre-FAc implant to 62 post-FAc implant (p=0.24) (figure 4, top panel). The mean CSFT declined from 358 μm pre-FAc implant to 340 μm post-FAc implant (p=0.37) (figure 4, middle panel). Mean IOP slightly increased from 17.2 mm Hg pre-FAc implant to 17.6 mm Hg (p=0.336). (figure 4, bottom panel) Eight subjects (27%) had an increase in IOP of >10 mm Hg after FAc implant. IOP >21 mm Hg was observed in 11 subjects (37%) pre-FAc implant and in 13 subjects (43%) post-FAc implant. IOP >30 mm Hg was observed in four subjects (13%) pre-FAc implant and in six subjects (20%) post-FAc implant. All four eyes with an episode(s) of pre-FAc IOP >30 mm Hg had a diagnosis of glaucoma prior to the FAc implant. All of the four eyes were on topical antihypertensives and two of them also received argon laser trabeculoplasty (ALT) prior to the FAc implant. Of those four eyes, only one eye subsequently developed another episode of IOP >30 mm Hg following the FAc implant. Following the FAc implant, a total of six eyes (20%) developed an episode(s) of IOP >30 mm Hg. Of those, four eyes had never been on topical antihypertensives, and their IOP normalised with an IOP-lowering drop(s). The fifth eye was on one topical antihypertensive, and the IOP normalised with an additional IOP-lowering drop. The sixth eye had an episode of IOP >30 mm Hg prior to the FAc implant which was controlled with topical antihypertensives and ALT and subsequently developed another episode of IOP >30 mm Hg following the FAc implant. This eye underwent repeat ALT followed by cataract extraction and intraocular lens placement with trabectome which normalised the IOP. Most of the IOP events were successfully treated with topical antihypertensive medications. Nine subjects (37%) required additional IOP-lowering drops post-FAc implant. Four of these subjects (13%) also underwent laser trabeculoplasty post-FAc implant. The four eyes that underwent laser trabeculoplasty following the FAc implant are of the two patients who received bilateral FAc implants. The first patient had an episode of IOP >30 mm Hg in both eyes prior to the FAc implant which was controlled with topical antihypertensives and ALT. The patient subsequently developed IOP >30 mm Hg in one eye and IOP >20 mm Hg in the other eye following the bilateral FAc implants and underwent ALT in both eyes with normalisation of the IOP. The second patient had no episodes of IOP >30 mm Hg in either eye prior to the FAc implant. This patient subsequently developed IOP >25 mm Hg in one eye while maintaining a normal IOP in the other eye following the bilateral FAc implants and underwent selective laser trabeculoplasty in both eyes with normalisation of the IOP. None of the subjects required an incisional glaucoma surgery post-FAc implant.
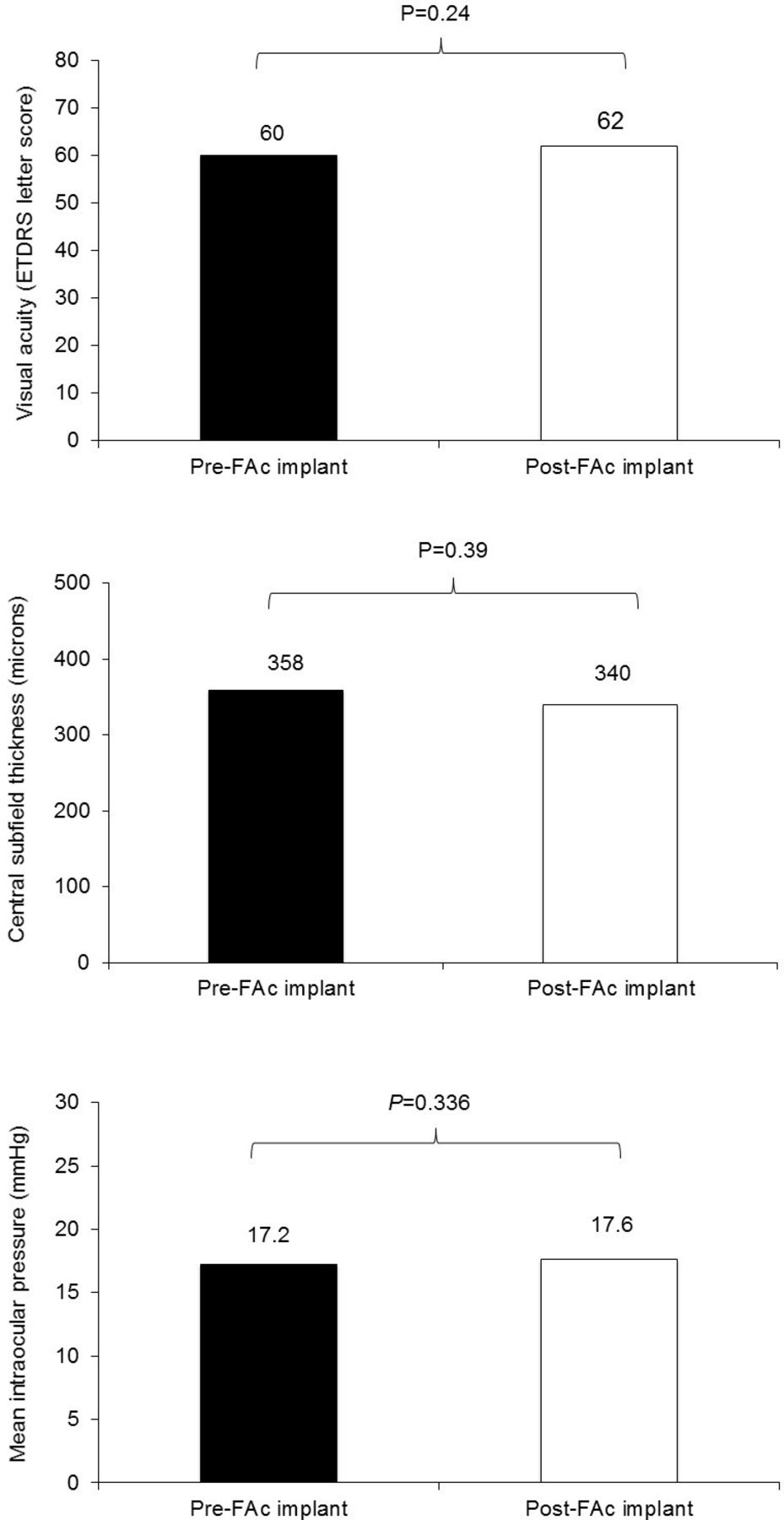
Mean visual acuity (top panel), central subfield thickness (middle panel) and intraocular pressure (bottom panel) for the 12 months pretreatment and post-treatment with the FAc implant. FAc, fluocinolone acetonide.
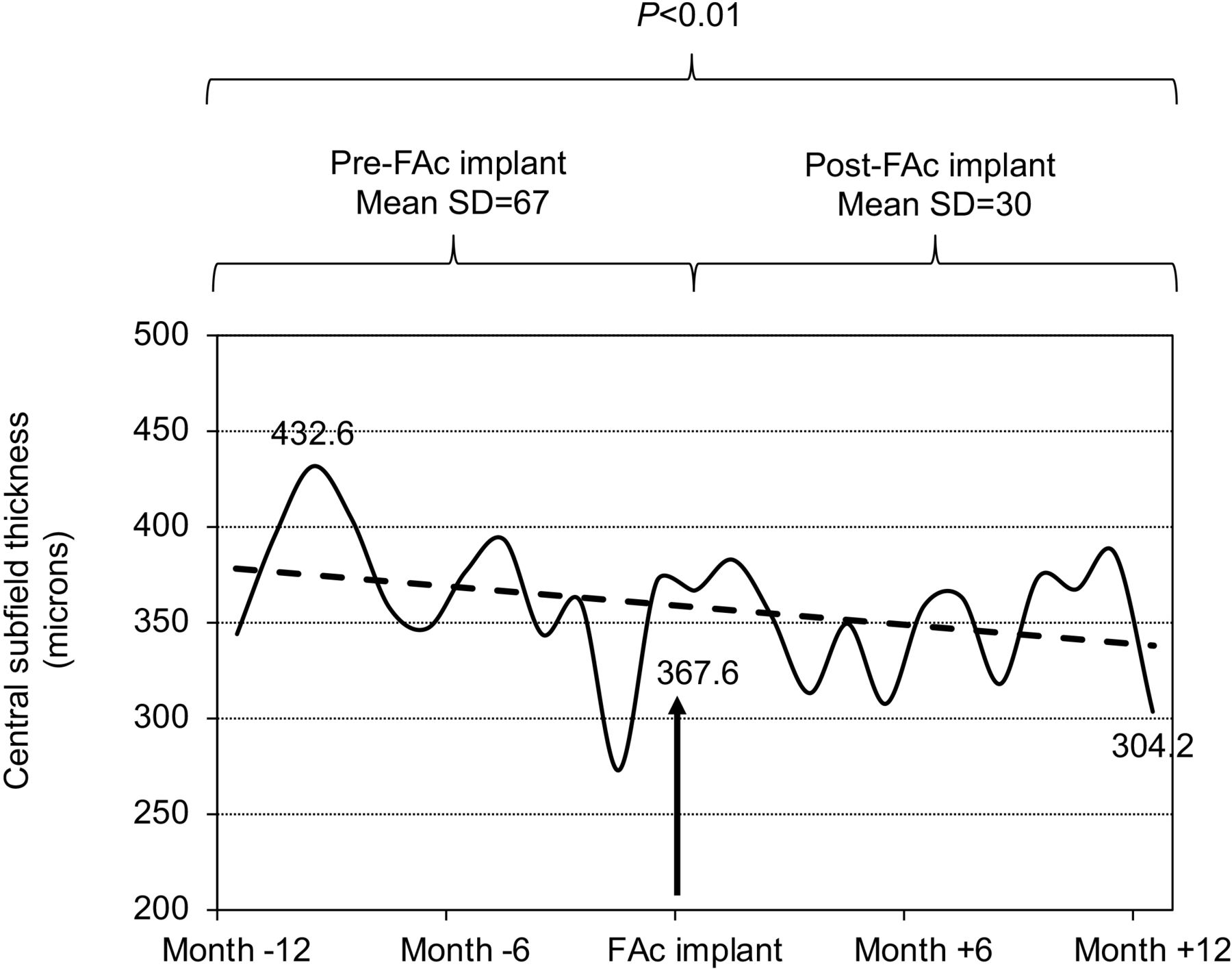
The variability analysis of the mean CSFT showed a significant reduction in the mean intrasubject SD from 67 μm pre-FAc implant to 30 μm post-FAc implant, indicating an improved stability of the oedema control associated with the administration of the FAc implant (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean central subfield thickness variability in the 12 months pretreatment and post-treatment with the FAc implant. FAc, fluocinolone acetonide.
DME treatment before the FAc implant was composed of 42% IVE, 23% IVO, 17% IVT, 16% IVA and 2% FLP. For the eyes that required additional treatment after the FAc implant was given, the treatment was composed of 64% IVE, 14% IVO, 14% IVT, 8% IVA and no FLP.
Discussion
Our small retrospective case series of 30 eyes clearly shows that treatment with the FAc implant is associated with notable reductions in treatment burden, satisfactory VA and CSFT results and markedly improved CSFT stability for the 12 months after the FAc implant compared with the 12 months prior to its implantation.
Patients with DME have heavy treatment burden. Studies have shown that patients with DME average one doctor’s appointment every 2 weeks.7 Intensive injection regimens can negatively impact both the patient and caretaker’s quality of life, and secondarily compliance with and adherence to treatment. Studies have shown that for every injection visit, more than half of working patients take a day off and more than 70% additionally need a caretaker’s assistance. Patients become anxious with injections with over half experiencing anxiety for at least 2 days leading up to the injection.12
From a therapeutic perspective, it is well established that all approved therapies for DME, except the FAc implant, require regular and repeated treatment visits to maintain a therapeutic effect.14 In contrast, a single injection of an FAc implant creates a therapeutic effect that lasts for up to 3 years.16 In the current study, the FAc therapeutic effect was adequate as monotherapy for DME control in most patients for the 12-month period after FAc implant injection. Treatment burden was significantly reduced regardless of pre-FAc VA. Whether the healthcare economics of this unique, durable and effective treatment option for patients with DME which alters and may improve practice resource utilisation is more cost effective than the recurrent repeated treatment visits associated with other approved DME treatments is an important area for future study.
Although randomised clinical trials support the benefits of monthly intravitreal injections, evidence from RCTs may not apply to real‐world practice, where patients are often less-treated and less‐monitored than the RCTs recommendations.17 Prior to FAc implantation, our patients were treated less frequently (every 2.6 months) than published treatment regimens of RCTs8 18 19 much like two large, real-world studies from the USA (ie, USER and PALADIN) where patients received about 1 injection every 3 months regardless of the baseline VA.12 14 15 This may represent a real-world ceiling effect inherent to DME treatment of patients not enrolled in a RCTs.20
The benefit of the FAc implant in reducing the injection burden while maintaining or improving anatomical and functional outcomes has been clearly demonstrated in both RCT21 and real-world studies.14 15 21 Our VA, OCT and treatment burden data were completely congruent with these reports showing a 70% reduction in injection frequency with 63% of patients not requiring additional injections after the FAc implant was administered. Our study is the first to look at the ophthalmology visit burden and stratify this by ophthalmic subspecialty in addition to treatment burden. After administration of the FAc implant, our patients had significantly fewer ophthalmology visits (27%). This was largely due to a 37% reduction in retina-related visits secondary to a 70% reduction in retina treatment visits. Despite cataract and glaucoma being known side effects of corticosteroid therapy, there was minimal to no increase in cataract or glaucoma related visits in our patient cohort. This is in part due to the high percentage of pseudophakic patients (83%) in our study population as well as the relatively short 12-month follow-up after the FAc implant in terms of the timeline of cataract formation. Of the five phakic patients, four (80%) had cataract progression and three (60%) had cataract surgery in the 12 months after the FAc implant. Nonetheless, our study suggests that the reduction of retinal injection visits does not appear to come at the expense of significantly increased visits to manage IOP and cataract events. Also, the reduction of injection visits after the FAc implant was not associated with a reduction in retinal clinic visits to monitor the clinical progression of diabetic retinopathy and DME.
All patients in our cohort received a prior course of a corticosteroid without a clinically significant rise in IOP, as required by the US FDA-approved label. Other real-world reports have validated that this approach significantly mitigates the risk of an uncontrolled IOP response.22 Our study further supports the risk mitigating effect of the US indication verbiage. The steroid IOP effects were predictable and manageable in our cohort of patients.
Reduced injection and clinic visit frequency may improve patient adherence to treatment. This is suggested by the stronger concordance between RCTs and real-world studies of patients receiving the FAc implant compared with RCT and real-world studies of patients receiving anti-VEGF injections for DME.11 18 19 Patients that require frequent injections but are not able to comply with frequent clinic visits may be able to receive adequate treatment with fewer clinic visits after the FAc implant with potentially better oedema control and long term visual outcomes due to better treatment adherence. We did not investigate the healthcare economic aspects of therapy with the FAc implant but strongly suggest this as an important area for future study.
The improved stability of CSFT measurements has been previously reported by our group in the setting of retinal thickness amplitude (RTA) calculations performed on USER, PALADIN and FAME study data sets.23 These variability measures have been found to correlate better with VA than individual CSFT measurements.14 The present patient cohort strictly excluded any previously reported patients from any of these three previously reported trials and represents a fourth data set that demonstrates improved CSFT stability following treatment with the FAc implant compared with pre-FAc implant. This study is the first report of using the SD of the CSFT signal to quantify the variability and this may prove to be a more accurate and precise way to characterise CSFT stability than other measures such as RTA, although this needs to be confirmed in future work. RTA only reports the difference between the maximum and minimum values of CSFT over a defined follow-up period ignoring all other data points whereas CSFT SD factors in all available data. We recommend using measures of CSFT and VA stability over time (whether RTA or SD) as potential useful measures of DME (and potentially other disease state) treatment efficacy and durability.
As with all retrospective studies, there are significant limitations to our study. ETDRS letter scores were calculated from non-standardised Snellen VA. Different intravitreal injections and lasers were counted equally regardless of their duration of the action. Physician criteria for those who were treated with the FAc implant were not defined and patient selection evolved over time as might be expected with any new treatment. We had a high number of pseudophakic patients limiting the strength of our conclusions regarding cataract formation and the treatment burdens associated with managing cataracts post-treatment with the FAc implant. There were only a limited number of subjects with 12 months of follow-up and insufficient power for important subanalyses.
Nonetheless, we conclude that the treatment burden was reduced after the FAc implant in our cohort of 30 eyes in the setting of predictable and favourable anatomical and visual results in patients with DME. Both treatment burden and ophthalmology visit burden were reduced by a clinically meaningful magnitude. Lesser treatment burden may reduce the challenges associated with monthly treatment visits in patients with diabetes who need frequent healthcare provider visits. The reduction in retina visit burden did not come at the price of less frequent retina monitoring visits or at the price of increased glaucoma/IOP or cataract visits. Less variability of CSFT over time after the FAc implant also supports the notion that long-term sustained release therapy may be associated with more stable anatomic and visual results when compared with the imperfect implementation of frequent intravitreal injection recommendations of RCTs in the real-world.
References
Footnotes
Contributors Substantial intellectual contributions to the content of this manuscript were made by the authors in the following areas. Planning the research question: MB and JO. Conducting the protocols described: MB and JO. Drafting, critical revision and final approval: MB, JO and CDR. Corresponding author and overall content guarantor: MB and CDR.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MB received a travel grant from Alimera Sciences for the poster presentation of this study at ARVO 2017 annual meeting. CDR receives compensation as a consultant and speaker for Alimera Sciences.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.