Article Text

Abstract
Objective This study aimed to compare the efficacy of a cotton tipped applicator and a knife blade in obtaining corneal samples in patients with infectious keratitis.
Methods and analysis This is a retrospective cohort study of patients with suspected infectious keratitis during 2004–2014. Samples for corneal culture were obtained by a cotton tipped applicator and a knife blade, and directly inoculated on GC agar, blood agar and Sabouraud agar.
Results In all, 355 patients were included. Corneal sampling by cotton tipped applicator yielded a significantly higher rate of patients with positive corneal culture, 156/355 (43.9%), compared with knife blade, 111/355 (31.3%) (p<0.001). On a patient level, the culture results obtained by the cotton tipped applicator and the knife blade were identical in 269/355 (76%) of the patients. The overall agreement between the two instruments on microbial level was 0.66 (Cohen’s kappa 95% CI 0.60 to 0.72).
Conclusion Corneal sampling by cotton tipped applicator generated a higher rate of positive corneal cultures and a higher proportion of isolated microbes than by knife blade. Future studies with randomised sampling order are needed to establish which instrument, cotton tipped applicator or knife blade, is the most effective in sampling microbes for direct inoculation in patients with infectious keratitis.
- infection
- microbiology
- cornea
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about the subject?
The identification of the causal microbe and the determination of its antibiotic susceptibility pattern are vital in the management of infectious keratitis. Thus, optimising the corneal culture procedure is of importance.
What are the new findings?
The findings of the present study indicate that the instrument used for corneal sampling in patients with infectious keratitis influences the corneal culture outcome. In our study, sampling with cotton tipped applicator generated a higher rate of positive cultures and a higher proportion of isolated microbes than the knife blade.
How might these results change the focus of research or clinical practice?
The findings of the current study indicate that a dry cotton tipped applicator is a more efficient instrument to use for corneal sampling in patients with infectious keratitis than a knife blade.
Introduction
Non-viral infectious keratitis is an acute ophthalmological condition caused by bacteria, fungi or protozoa that in a worst case scenario can result in corneal perforation and endophthalmitis. The diagnosis is clinical, based on slit-lamp biomicroscopy and patient history, but corneal sampling for culture is required to identify the causative microbe(s) and their antibiotic susceptibility pattern. Some of the steps in the procedure of corneal culture in infectious keratitis are well studied, such as which topical anaesthesia to use prior to corneal sampling,1–4 appropriate inoculation media and whether to inoculate directly or via a transport medium.5–11 The optimal method for obtaining a corneal sample has only been reported in cases series with a limited number of patients included.12–14 The instruments used can be divided into two groups: sharp or blunt metal instruments such as Kimura spatula, surgical knife blade or needle; and non-metal instruments with absorbent qualities such as calcium alginate swab, cotton tipped applicator or Mini-tip Culturette.
The aim of this study was to investigate if the sampling instruments, cotton tipped applicator and knife blade, by direct inoculation on agar plates, influenced corneal culture outcome in infectious keratitis.
Materials and methods
This retrospective study made use of both medical records and microbiology reports over a period of 11 years, from 1 January 2004 to 31 December 2014.
Patients with suspected infectious keratitis from whom corneal cultures were obtained at any of the three departments of ophthalmology in the region of Örebro County were eligible for inclusion. One of these, the Department of Ophthalmology at the University Hospital in Örebro is a tertiary corneal referral centre. The other two, situated in the towns of Lindesberg and Karlskoga, respectively, provide primary outpatient ophthalmological care during office hours. Patients were included if they met at least one of two inclusion criteria15: (1) positive corneal culture (all growth of microbes was considered positive) and (2) stromal infiltration with overlying epithelial defect in combination with one or more of the following: lesion within or overlapping the central 4 mm of the cornea and/or uveitis and/or pain.
Eligible patients were searched for by two pathways to minimise losses due to failure to identify cases: first by diagnostic code for keratitis in the patient records (code H16.9 in version 10 of the International Classification of Disease) and second by searching for corneal cultures in the database at the Department of Laboratory Medicine, Clinical Microbiology, Örebro University Hospital. Of the 392 patients with keratitis that were identified, 2 were excluded due to lack of medical charts, 2 due to inadequately handled cultures and 33 due to cultures not performed in accordance with the written instructions on corneal culture described in detail in the "microbiological culture" section below.
Patient involvement
Patients were not directly involved in the design of this study.
Microbiological cultures
Corneal samples were obtained by either an ophthalmologist or a resident in ophthalmology according to written instructions available at the relevant time period. These written instructions were in accordance with the Swedish State of the Art Document on Infectious Keratitis Caused by Bacteria, Yeast and Protozoa,16 and can be considered a routine procedure. This document recommended both a so-called direct and indirect inoculation of the corneal specimen. When directly inoculated, the corneal specimen was directly transferred onto agar plates. When indirectly inoculated, an enrichment media, fastidious anaerobic broth, was used and later subcultured onto agar plates for both anaerobic and aerobic incubation at the laboratory. In this study, only the culture results from direct inoculation on agar plates are examined.
Corneal samples were collected according to the following standard procedures. Samples from the infiltrates were first collected with sterile cotton tipped applicators, one for each plate, and streaked onto one half of each of the three agar plates. The cotton tipped applicators were not moistened with any liquid prior to corneal sampling, that is, they were used dry without any modifications. This was followed by samples collected from the infiltrate by scraping with a sterile knife blade held withtable 1 a sterile glove or sterile forceps and streaked onto the other half of the same three agar plates in the same order. The plates used were GC agar (GC Medium Base, Becton Dickinson (BD), Sparks, Maryland, USA, supplemented with 1% BBL IsoVitaleX enrichment), blood agar (3.9% Columbia Blood Agar Base, Oxoid, Basingstoke, Hampshire, UK, supplemented with 6% defibrinated horse blood) and Sabouraud (SAB) agar (1.3% Agar No2, Lab M, Heywood, Bury, UK; 4% D-Glucose, VWR, Leuven, Belgium; 1% Peptone BD) for isolation of fungi.
Agreement and differences between cotton tipped applicator and knife blade in isolated microbes subdivided according to presumed pathogenicity in the study population 2004−2014
There is only one clinical microbiological facility in the region of Örebro County, the Department of Laboratory Medicine, Clinical Microbiology, Örebro University Hospital. Thus, all corneal cultures obtained at any of the three departments of ophthalmology were registered and handled at the same microbiological laboratory as follows: the GC agar plate was incubated in CO2 at 36°C, the blood agar plate was incubated in air at 36°C and the SAB plate was incubated in air at 30°C.
All plates were checked for growth on days 1 and 2, and if no growth was detected at day 2, the plates were incubated for another 5 days for a final evaluation. The SAB plate was checked every day and discarded after 7 days if no growth was detected.
If bacterial growth was detected, further typing to species level was carried out in one of two ways. Before January 2014, typing was carried out with currently available routine methods including API kits. From January 2014 onwards, it was carried out with matrix-assisted laser desorption/ionisation time-of-flight mass spectrometry (Microflex LT and Biotyper 3.1, Bruker Daltonik, Bremen, Germany).
For the purpose of further analysis, microbes isolated by direct inoculation were divided into two groups according to presumed pathogenicity. We used two different sets of definitions: Fleiszig and Efron’s classifying coagulase-negative staphylococci, Corynebacterium spp. (except C. diphtheriae), Cutibacterium acnes, Micrococcus spp., Bacillus spp. and Peptostreptococcus spp. as normal flora and other microorganisms as potentially pathogenic17; second, our own classification based on microbial virulence and clinical experience (see footnote in table 1).
Statistical analysis
Agreement between cotton tipped applicator and knife blade on a microbial level was calculated as Cohen’s kappa and as positive and negative agreement, 95% CI. Differences in culture outcome and in isolation of the different microbes were calculated with McNemar’s test. When analysing the isolated microbes in total and in the two subgroups according to pathogenicity, we used the same procedure of summarising the culture negative readings by both methods as Pakzad-Vaezi et al,9 that is, the negative plate readings for each species were totalled. All these statistical calculations were performed through the Vassarstat.net website.18 Additional statistical analysis concerning the baseline characteristics (table 2) were calculated in using IBM SPSS software package V.25, using Pearson’s χ test or Fischer’s exact test when appropriate, t-test for comparing mean age and the Mann-Whitney U-test for comparing median visual acuity at first visit.
Baseline characteristics in the study population with suspected infectious keratitis (2004–2014), in total and according to outcome of corneal culture by direct plating under aerobic conditions
Results
In all, 355 patients with infectious keratitis were included. Antimicrobial treatment had already started at the time of sampling in 65 cases. Mean age at episode onset was 50.5 years, median BCVA in Snellen equivalents (SE) was 0.6 and the most common risk factor for keratitis was contact lens wear (n=155) (table 2).
When the study population was divided into culture positive and culture negative outcome, based on direct inoculation, the culture positive group displayed a significantly higher mean age (p<0.001), a significantly higher proportion of left eyes (p=0.038) and a significantly lower median BCVA (SE) at first visit (p<0.001) (table 2).
Positive corneal cultures by direct inoculation were seen in 46.5% (165/355) of the cases. Cotton tipped applicator generated a culture positive rate of 43.9% (156/355) and knife blade a culture positive rate of 31.3% (111/355) (p<0.001).
Polymicrobial growth on direct inoculation was seen in 29 cases: 26 cases with two microbes, 2 cases with three microbes and 1 case with four different aerobic microbes (table 2). In total, 198 isolates (194 bacterial and four fungal) were isolated by direct plating. Of these, 99 (50%) microbes were isolated by both instruments, 81 (41%) by cotton tip only and 18 (9%) by knife blade only (table 3).
Agreement between cotton tipped applicator and knife blade on isolated microbes after direct plating in patients with infectious keratitis
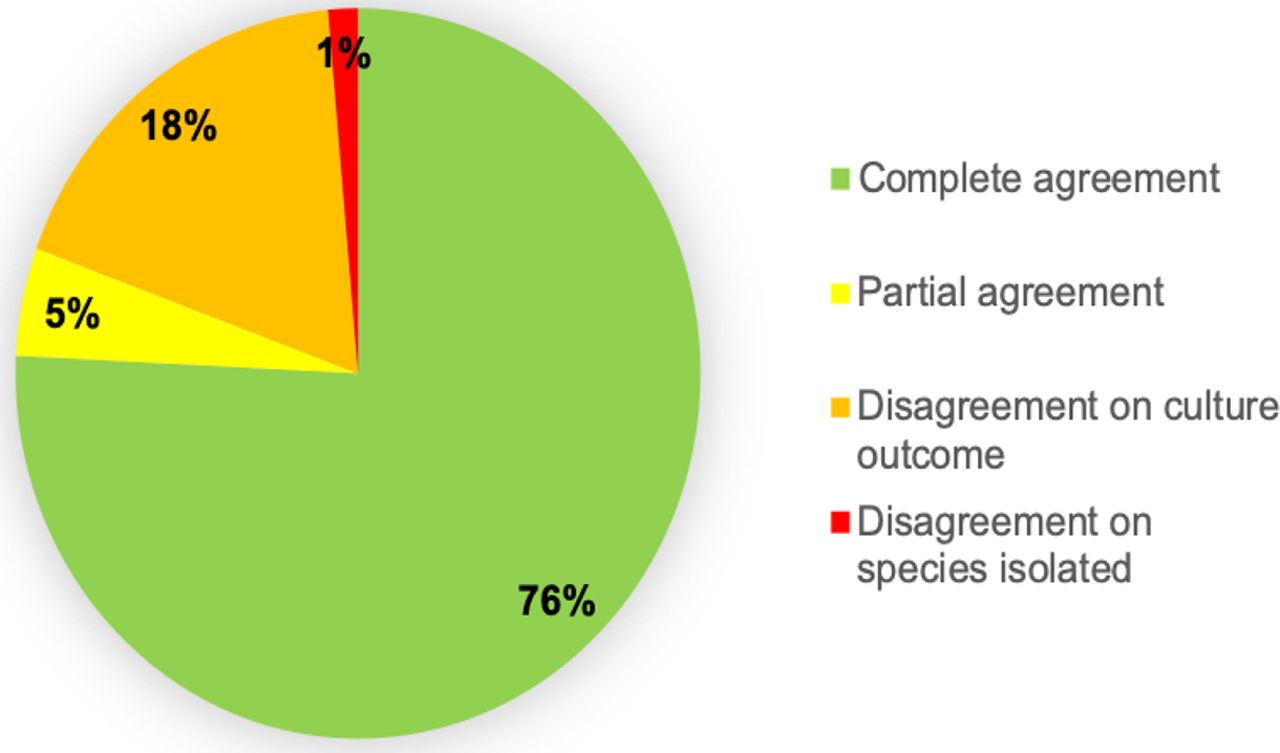
On the patient level, cultures by cotton tipped applicator and knife blade were identical in 76% (269/355) of the patients, either culture negative (190 patients) or culture positive with identical isolated microbe(s) (79 patients) (figure 1). Of the 79 patients with positive corneal culture, 76 cases showed monomicrobial growth and 3 cases showed polymicrobial growth with two microbes. Cotton tipped applicator and knife blade disagreed in 19% of the patients (69/355), either on culture outcome (n=64 (18%)) or on the identity of the microbe isolated (n=5 (1%)). The isolates from these five patients are shown in table 4.
{kind=link}
Agreement on the patient level in corneal culture results between sampling with cotton tipped applicator and knife blade in patients with infectious keratitis 2004–2014 (n=355). Complete agreement ( ): both methods culture negative (n=190) or both methods culture positive displaying the same species (n=79), partial agreement (
): both methods culture negative (n=190) or both methods culture positive displaying the same species (n=79), partial agreement ( ): of one isolated species, in samples displaying polymicrobial growth (n=17), disagreement on culture outcome (
): of one isolated species, in samples displaying polymicrobial growth (n=17), disagreement on culture outcome ( ): culture positive by cotton tipped applicator only (n=55) or by knife blade only (n=9), disagreement (
): culture positive by cotton tipped applicator only (n=55) or by knife blade only (n=9), disagreement ( ) on species isolated (n=5).
) on species isolated (n=5).
Microbes isolated in patients with inconsistent corneal culture result between cotton tipped applicator and knife blade
Of the 64 patients who differed in culture outcome, 60 showed monomicrobial growth and 4 showed polymicrobial growth of two microbes; 55 were culture positive by cotton tipped applicator only and 9 by knife blade only.
In the remaining 5% (17/355), cotton tipped applicator and knife blade agreed partially; that is, on the identity of one of two to four isolated microbes in patients displaying polymicrobial growth (figure 1). Of these patients, 15 had two microbes, 1 had three microbes and 1 had four microbes.
On the microbial level, the overall agreement between cotton tipped applicator and knife blade as calculated with Cohen’s kappa was 0.66, 95% CI 0.60 to 0.72. When isolated microbes were classified as either potential pathogens or normal flora according to Fleiszig and Efron,17 the agreement was 0.76 for potential pathogens and 0.50 for normal flora. When our own classification of ‘probably pathogenic’ versus ‘commensal’ was applied (see footnote in table 1), Cohen’s kappa was 0.78 and 0.54, respectively (table 1).
Discussion
In the present study, we investigated two instruments used for obtaining corneal material for direct inoculation in patients with suspected infectious keratitis: a blunt instrument with absorbent properties, that is, a dry sterile cotton tipped applicator and a sharp, sterile, non-absorbent knife blade.
The cotton tipped applicator yielded a statistically significant higher rate of both positive corneal cultures and a higher proportion of isolates than the knife blade. In a previous study by Benson et al12 where samples were inoculated directly on agar plates, they observed that a moistened calcium alginate swab gave a significantly higher retrieval of organisms from bacterial keratitis than a platinum spatula.12 Jacob et al compared knife blade with a moistened calcium alginate swab, and they did not find any difference between the two instruments used on bacterial and mixed ulcers, but the swab retrieved a significantly greater number of organisms in cases of mycotic ulcers. However, they inoculated the specimens indirectly through a Calgon solution.
We chose the dry cotton tip approach since moisturising the cotton tip with any liquid may reduce its absorbent qualities. However, in an animal study by Epley et al, there were no difference in yield between a dry and a saline moistened Dacron tipped applicators (Mini-tip Culturette).13
There have been concerns that a cotton tipped applicator may favour the uptake of transient commensals and not only representative infectious material from the infiltrate.19 We therefore divided the findings of isolated microbes into two groups according to presumed pathogenicity. When grouping the isolated microbes into more or less pathogenic, the cotton tip yielded a statistically higher proportion of isolated microbes in both groups no matter which pathogenicity classifications we used.
There may be several explanations as to why the cotton tip generates more isolates and a higher rate of positive cultures. The ophthalmologists may be more confident in handling a cotton tipped applicator compared with a knife blade, which can potentially induce more harm to the patient. In addition, the risk of perforating the surface of the agar when transferring the obtained sample from the instrument to the agar plate is probably less with a cotton tip than a knife blade, which facilitates a correct interpretation of the agar plate. The absorbent qualities of the cotton tip compared with the knife blade may also play a role.12
This study showed an overall agreement of 76% between the instruments on a patient level and an agreement of 0.66 (Cohen’s kappa) on microbial level, which can be considered as good20 or substantial.21 The major difference in the patient level was not on the identity of the isolated microbe, but on culture outcome, that is, if the culture was positive or not, with a majority of the cultures (55/64) positive by cotton tipped applicator only. This could indicate that sampling by cotton tip is more effective at obtaining microbes in patients with suspected infectious keratitis. Since 18% of the culture positive cases in our study displayed polymicrobial growth, and polymicrobial growth has been reported in even higher rates, 32%,22 we believe that agreement on the patient level is relevant from a clinical point of view.
One strength of our study is the number of patients included and the likelihood of a low number of missing cases, since we applied two separate approaches to identifying patients with suspected infectious keratitis.
A major limitation of the study is the retrospective design. Medical charts and culture procedures were not always complete, which resulted in exclusion of some cases. The order of obtaining corneal material for culture was not randomised, and this may have favoured the cotton tipped applicator. There is, however, evidence in the literature that sampling order does not influence the number of different species recovered by direct plating9 or the amount of microbial growth.12 14 Furthermore, in an in vitro study by Kaye et al, there was evidence that up to five scrapings could be obtained from pig corneas without affecting viable counts of S. aureus.6
In our region, fungi as an infectious agent in keratitis are rare compared with bacteria, and therefore, the sample size of this subgroup was very small.
Conclusion
The overall agreement on microbial level between cotton tipped applicator and knife blade was good. Corneal sampling for direct inoculation by cotton tipped applicator yielded a significantly higher proportion of positive cultures and higher proportions of isolates, both those considered pathogenic and those considered not. In our study population, which consisted of mainly bacterial ulcers, very few probably pathogenic microbes would have been missed if sampling for direct inoculation was performed by using solely a cotton tipped applicator. Further prospective studies with randomised sampling order are needed to establish which instrument is the most effective in sampling microbes for direct inoculation in patients with infectious keratitis.
References
Footnotes
Contributors All authors have contributed to the manuscript according to the guidelines by ICMJE.
Funding This study was funded by Region Örebro County Council research committee.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval by the Regional Ethical Review Board of Uppsala (ref: 2015/335/1) was obtained before the study was initiated.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.