Article Text

Abstract
Objective To present the study design and the baseline data of a prospective cohort study investigating the safety, refractive correction and effectiveness of myopia control in subjects fitted with orthokeratology (ortho-k) lenses of different compression factors.
Methods and analysis This study is a 2-year longitudinal, double-masked, partially randomised study. Myopic children aged between 6 and 10 years are recruited and they may choose to participate in either the ortho-k or spectacle-wearing group. Subjects in the ortho-k group are randomly assigned to wear ortho-k lenses of either conventional compression factor (CCF, 0.75 D) or increased compression factor (ICF, 1.75 D). For the ortho-k subjects, the time and between-group effects within the first month of lens wear were analysed.
Results Sixty-nine ortho-k subjects (CCF: 34; ICF: 35) and 30 control subjects were recruited. There were no significant differences in baseline demographic data among the three groups of subjects (p>0.19). At the 1-month visit, the first fit success rates were 97% and 100% in the CCF and ICF ortho-k group, respectively. A higher percentage of ICF subjects could achieve full correction (CCF: 88.2%; ICF: 94.3%). The change in axial length was significantly higher in the ICF group (CCF, 0.003 mm; ICF, −0.031 mm) (p<0.05). No significant between-group differences in daytime vision or in the coverage and depth of corneal staining between the two ortho-k groups (p>0.05) were observed at any visit.
Conclusion ICF did not compromise the corneal integrity and the lens centration within the first month of lens wear. The preliminary performance of ortho-k lenses with ICF of 1.00D shows that it was safe to be used in the longer term for the investigation of myopia control.
Trial registration number NCT02643342.
- contact lens
- treatment other
- optics and refraction
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Orthokeratology (ortho-k) lenses with conventional compression factor (CCF) may not be adequate for achieving targeted refractive correction. The myopia control efficacy was relatively higher in the group of children with higher refractive errors.
What are the new findings?
Compared with CCF, in the increased compression factor (ICF), there was no difference in either the lens performance, in terms of centration, or the external ocular health. Although the desired over-correction could not be achieved in the ICF group, the axial length shortening was significantly higher than the CCF group at the 1-month visit, which may imply an increase in myopia control efficacy.
How might these results change the focus of research or clinical practice?
A long-term longitudinal study was warranted to confirm the effect of ICF, and this may lead to use of a new design in ortho-k lenses.
Introduction
Compression factor (also known as Jessen factor) refers to the extra power, apart from the manifest refractive power of individuals, added on to the target of orthokeratology (ortho-k) lenses, in order to achieve an over-correction1 2 for counteracting the daytime regression after lens removal in the morning.3 The incorporated compression factor varies among different ortho-k lens manufacturers, but usually ranges from 0.50 to 0.75 D. Clinical studies have reported that the desired target reduction in refractive error may not be achieved with the conventional compression factor (CCF, 0.75 D).4–7 According to a retrospective analysis of the refraction at the second week of lens wear in 123 ortho-k-treated patients,8 an extra of 1.48 D rather than 0.75 D was required to obtain an over-correction of 0.75 D.
Although evidence for ortho-k lenses in slowing down axial elongation has been well documented,9–15 the exact mechanism remains unknown. The myopic defocus to the retina induced by the cornea after ortho-k lenses wear has been proposed as the mechanism of slowing axial elongation.16 Therefore, the efficacy for myopia control of ortho-k lenses may be enhanced by increasing the steepening at the mid-peripheral cornea. The increased compression factor (ICF, 1.75 D) ortho-k can potentially achieve this purpose and induce a higher amount of peripheral retinal myopic defocus. Previous studies have shown promising results that greater corneal power changes were related to slower axial elongation,17–19 although Santodomingo-Rubido et al reported that there was no relationship between corneal power changes and either short-term or long-term axial elongation in ortho-k lens wearers.20 However, they did not account for the corneal power changes over the cornea across the entire treatment zone (including the steepened mid-peripheral annulus); considering only two points (paracentral (3–5 mm) and pericentral (5–8 mm)) at the cornea, whose results might be significantly affected by lens decentration or corneal asymmetry. In view of the potentially enhanced myopia control efficacy for ICF ortho-k and to investigate the equivocal results on the association between corneal power changes and axial elongation, a long-term longitudinal study is warranted.
This 2-year longitudinal study is therefore conducted to determine the myopia control efficacy and long-term ocular responses of eyes fitted with ICF ortho-k lenses. In this report, the study design, and the lens performance of the ICF and CCF lenses, axial length (AL) and changes in central corneal thickness (CCT) in the ortho-k groups at the 1-month visit are presented.
Materials and methods
Study design
This is a partially randomised, double-blinded study to compare myopia control efficacy in subjects fitted with ICF or CCF ortho-k lenses and those wearing single-vision spectacles. The primary outcome is the axial elongation over a 2-year period.
Subjects are recruited via advertisements posted in local newspapers and through the internal email system of The Hong Kong Polytechnic University. Written informed consent is obtained from the parent/guardian before commencement of any procedures. Subjects may choose to participate in either the ortho-k or spectacle-wearing group; however, ortho-k subjects are randomised to wear either CCF or ICF ortho-k lenses in both eyes according to a spreadsheet generator (Excel; Microsoft, Redmond, WA).
Subjects
Children of age 6 to not more than 12 years old, with myopia of 0.50 D to 4.00 D (inclusive) and astigmatism of less than 1.50 D, are recruited. Eligible subjects should be free of any ocular and systemic diseases and without any history of contact lens wear or myopia control treatment. The details of inclusion and exclusion criteria are listed in table 1.
Inclusion criteria
Subjects are prescribed with ortho-k lenses (test groups) or single-vision spectacles (control group). Subjects in the ortho-k groups are randomly fitted with either CCF or ICF lenses in both eyes. They are masked to the compression factors of their lenses. They are required to follow the instructions of daily cleaning (Spray and Clean; Menicon, Japan), rinsing (Saline, Ophtecs, Japan), disinfection (MeniCare Plus; Menicon), weekly cleaning (Progent; Menicon), and monthly replacement of care products and lens cases.
Interventions
Ortho-k lenses
All ortho-k subjects are fitted with the Menicon Z Night ortho-k lenses (NKL Contactlenzen, The Netherlands) made of gas-permeable lens material (Menicon Z material, DK 163 ISO, central lens thickness 0.24 mm) (table 2).
Lens details of Menicon Z Night lens
The initial lens parameters are determined using the computer software provided by the manufacturer (Easy Fit Software, V.2013; NKL Contactlenzen). The software uses the data obtained from the corneal topographer (Medmont E300 topographer; Medmont, Australia), subjective refraction and horizontal visible iris diameter to determine the lens parameters. Default parameters suggested by the software are ordered for the CCF group, but the compression factor is increased from 0.75 D to 1.75 D for ordering of lenses for the ICF group.
The target reduction in the two ortho-k groups is determined according to their baseline subjective refraction and remains unchanged throughout the whole study. A pair of single-vision over-spectacles, made of the same materials as those prescribed for the control subjects, are prescribed to correct the residual refractive errors for those with residual spherical equivalent refraction (SER) exceeding 0.50 D in either eye or monocular aided vision worse than or equals to 0.18 (logMAR) after stabilisation in refractive correction of the ortho-k treatment. Spare lenses are ordered for the ortho-k subjects in case of any damage or loss. All lenses are replaced annually.
Single-vision spectacles
For the control subjects, single-vision spectacle lenses with spherical design and made of plastic material with refractive index of 1.60 are used (Hoya Lens, Japan). The prescription is updated when the monocular aided vision is 0.18 (logMAR) or worse, or the change in SER is 0.50 D or greater.
Examination schedules and procedures
Cycloplegic examinations are performed at baseline and every 6 months on all subjects, after the commencement of the study (table 3).
Data collection schedule
These visits are all scheduled at about the same time of the day as the baseline visit to minimise the influence of diurnal variation on ocular parameters. Ortho-k subjects have to attend four extra follow-up visits: in the morning after the first overnight, first week, second week and 1 month after lens delivery. These visits aim to assess the lens performance and ocular health of the subjects. Unscheduled visits are provided if required.
Before the cycloplegic examination, two drops of 1% cyclopentolate applied 5 min apart are instilled. The pupillary response and the amplitude of accommodation are assessed after at least 30 min. Cycloplegic measurements are performed on the eyes only when there is no pupillary response and the amplitude of accommodation is less than 2.00 D.
Objective refraction is measured with an open-field autorefractor (Shin-Nippon 5500K; Ajinomoto Trading, Japan). Five readings with less than 0.25 D difference in both sphere and cylinder are recorded and averaged for analysis. Subjective refraction is conducted under standard clinical protocol with maximum plus for maximum visual acuity (VA). High-contrast (>90%) VA is measured by using the Early Treatment Diabetic Retinopathy Study charts (Series 2000; Precision Vision, IL, USA). The Efron grading scale21 is used to grade ocular signs which were observed on biomicroscopy.
An optical biometer (Lenstar LS 900; Haag-Streit AG, Switzerland) is operated by the masked examiner for AL and CCT measurements. Five measurements with between-measurement difference of not more than 0.02 mm are recorded and averaged for analysis. The corneal profile is measured with a corneal topographer (Medmont E300 topographer; Medmont). Four measurements with each score higher or equal to 98 are recorded.
A Shack-Hartmann aberrometer (Complete Ophthalmic Analysis System (COAS); Wavefront Sciences, New Mexico, USA) is used to measure the ocular aberrations with different accommodation stimuli of 0 D to 4 D (1 D per step) before cycloplegia and 0 D after cycloplegia. A total of 125 measurements for each accommodation stimulus are averaged and used for analysis. The corneal biomechanical properties are measured with a dynamic bidirectional applanation device (Ocular response analyzer (ORA); Reichert, USA). Four measurements with waveform score higher or equal to 4.0 are recorded.
The anterior and posterior segment optical coherence tomography (OCT) images are captured with an anterior OCT (CASIA ss-1000; Tomey, Japan) and a posterior OCT (Spectralis OCT; Heidelberg Engineering, Germany), respectively. The anterior OCT images are captured under customised two-dimension and three-dimension scanning modes with auto alignment. The resolution for the two-dimension scanning mode is set to be 2048 A-scans with a scan range of 16 mm for vertical and horizontal meridians. The three-dimension scanning mode is set to be 16 radial scans across the 10 mm scan range across the cornea.
The posterior OCT images consist of six radial line scans of 30 degrees long and 30 degrees apart with enhanced depth imaging mode. The first image taken at the baseline visit is set as the reference. All the sequential images are scanned at the same location as the reference by using the manufacturer’s ‘re-scan’ function. Three OCT images of anterior and posterior segment are saved.
Masking
The primary outcome of the longitudinal study is the increase in AL. To eliminate any examiner bias, a masked examiner measures and records AL measurements.
Sample size
Based on the 2-year axial elongation reported in two previous studies9 11 (ROMIO: 0.36±0.24 mm, HMPRO: 0.19±0.21 mm; 0.17 mm difference in elongation between ortho-k groups and SD of 0.21 mm) and according to the equation by Sakpal,22 a minimal sample size of 24 subjects in each ortho-k group is required to give a power of 80% at a two-sided 5% significant level. Assuming 30% dropouts, at least 34 subjects in each ortho-k group are recruited.
Statistical analysis
Following determination of normality of all data, most parameters were normally distributed, except cycloplegic subjective astigmatism. The significance level was set at 0.05. Only the data from right eyes are presented in this report. The differences in baseline characteristics between groups were analysed using one-way analysis of variance (ANOVA) or Kruskal-Wallis test, where appropriate. For the investigation of the time and between ortho-k group effects of parametric parameters, repeated measures ANOVA and post hoc tests with Bonferroni correction were used. For astigmatism, Friedman test and Mann-Whitney U test with Bonferroni correction were used, respectively. The refractive data were also transformed into Long’s formalism (SCxA) and the time effect was tested by using Hotelling’s T-squared.23 To evaluate the difference in external ocular health between two ortho-k groups, Mann-Whitney U test was used for ordinal data.
Patient and public involvement
Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or interpret the results. Patients were not involved in writing or editing of this article.
Results
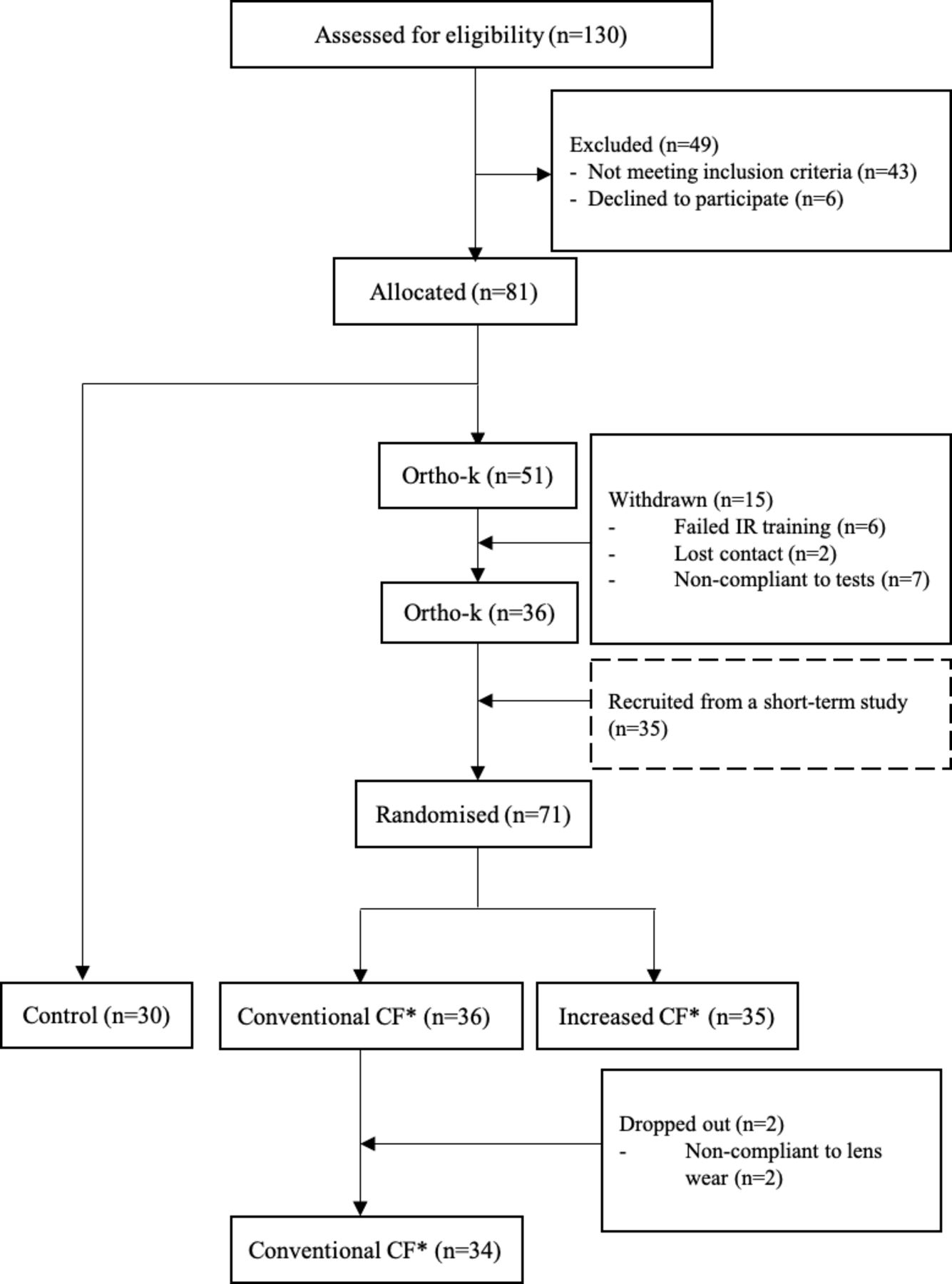
Thirty-six and 35 subjects were fitted with CCF and ICF lenses, respectively, and 30 subjects were fitted with single-vision spectacles (figure 1). Two subjects in the CCF group were excluded before the 1-month visit because of non-compliance with lens wear. Thirty-four subjects in the CCF group and 35 subjects in the ICF group completed the 1-month visit. At 2-week visit, one CCF subject needed to be refitted because of lens decentration, yielding a first fit success rate of 97% (33/34) and 100% (35/35) for CCF and ICF groups, respectively.

Flowchart of the conduct of the study. *CF, compression factor.
Table 4 shows a summary of the baseline data for the control and two groups of ortho-k subjects who completed the 1-month visit. No significant differences in baseline age, pre-cycloplegic and post-cycloplegic subjective refraction, high-contrast unaided and best-corrected visual acuity, and AL were found among the three groups (p>0.05).
Mean±SD (or median (range)) age and ocular parameters of the subjects at the commencement of the study
Ocular characteristics of the ortho-k subjects after 1 month of lens wear
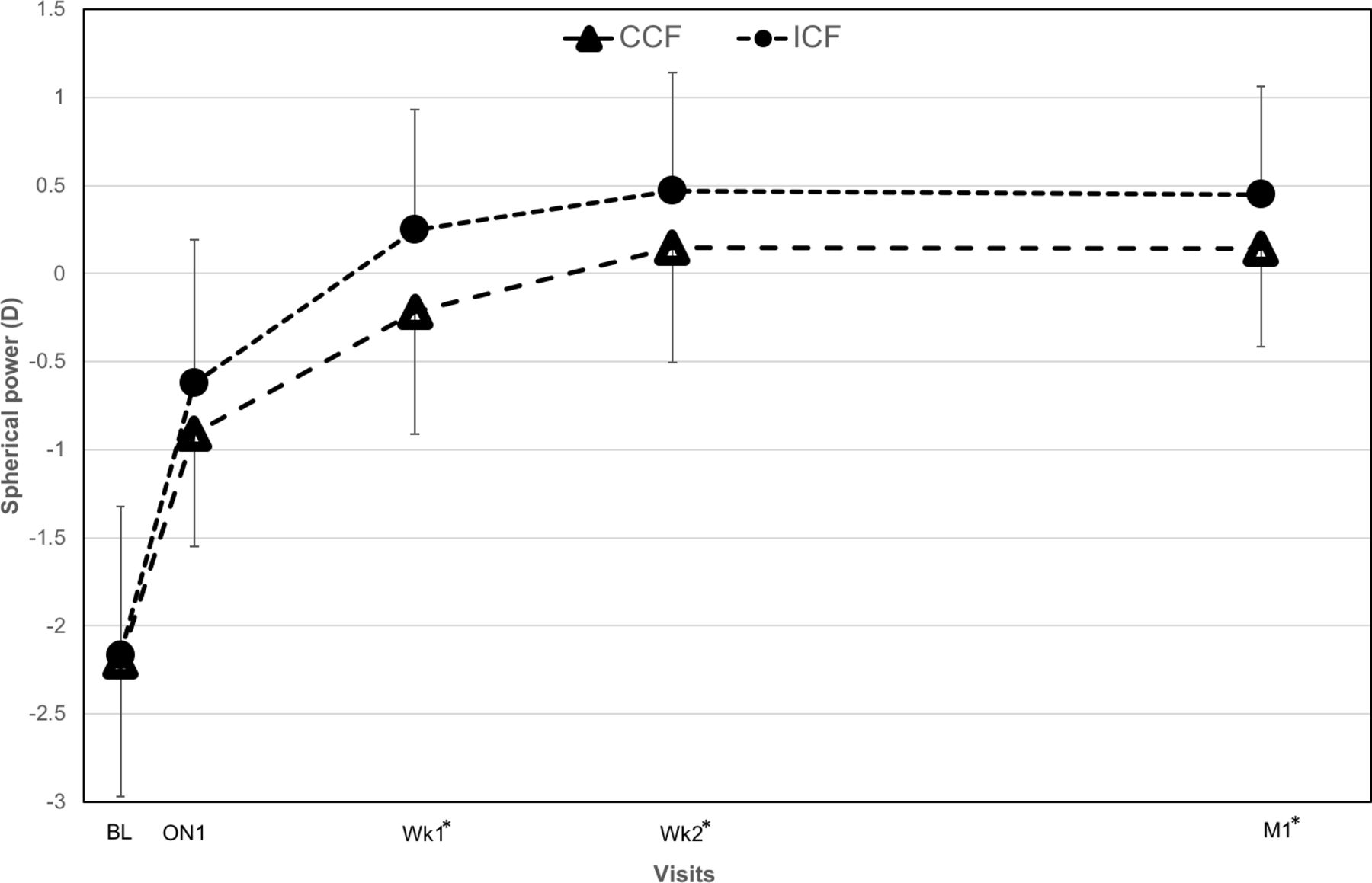
Changes in myopia for CCF and ICF groups are shown in figure 2. The refractive errors (SCxA) at 1-month visit were 0.12–0.20×10 and 0.42–0.13×19 for CCF and ICF, respectively. Myopia in the ICF group were significantly more positive than the CCF group from the 1-week visit onward (p<0.05). No significant reduction in astigmatism was observed in either group of subjects (p>0.05), and no significant differences were observed between the two groups at all visits (p>0.05) during the first month of lens wear. Full correction is defined as residual myopia of less than 0.50 D. Four subjects in the CCF group (11.8%) and two subjects in the ICF group (5.7%) did not achieve full correction at the 1-month visit. No significant difference in high-contrast unaided VA and best-corrected VA between the two ortho-k groups was observed at any visit (p<0.05).

Changes in myopia in ortho-k subjects wearing lenses of conventional compression factor (CCF) and increased compression factor (ICF). Error bars indicate the SD. The asterisk (*) denotes a significant difference in myopia between groups. BL, baseline; ON1, first overnight; Wk1, first week; Wk2, second week; M1, 1 month.
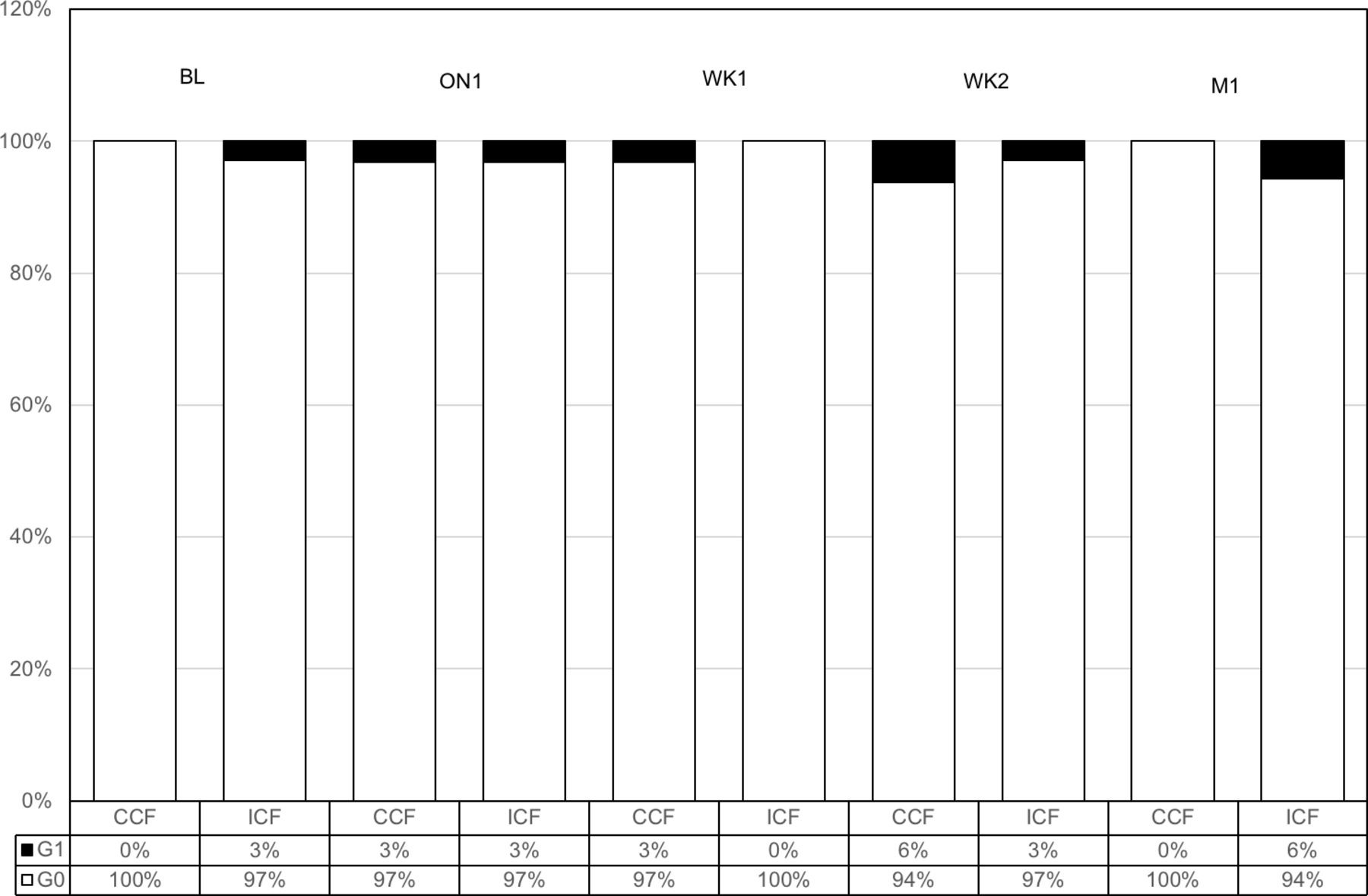
The coverage and depth of corneal staining observed during the first month of lens wear were not more than grade 2 in all ortho-k subjects. Central corneal staining observed in both groups at different visits are presented in figure 3. There were no significant differences in either coverage or depth of corneal staining between the two groups (p>0.05) at any visit. Corneal pigmented arc was observed in one subject in the CCF group at the 1-month visit and none in the ICF group. No infectious keratitis or any other serious ocular conditions occurred during the 1 month of lens wear.

{kind=link}
{kind=link}
{kind=link}
Severity (coverage) of central corneal staining in conventional compression factor (CCF) and increased compression factor (ICF) groups. BL, baseline; ON1, first overnight; WK1, first week; WK2, second week; M1, 1 month; G0–G1: grade 0 to grade 1.
AL was reduced in the ICF group (mean (SD) change: −0.031 (0.060) mm; p<0.05) but remained unchanged in the CCF group (mean (SD) change: 0.003 (0.038) mm; p>0.05) at the 1-month visit. The between-group difference in AL change was significant (p<0.05). CCT were reduced in both ortho-k groups (p<0.05) from baseline to the 1-month visit, although the between-group difference was not significant (p>0.05). The mean (SD) changes in CCT were −7.03 (8.06) and −10.34 (5.97) μm, respectively.
Discussion
This report presents the study design and the preliminary findings of ortho-k subjects participating in a longitudinal study exploring the efficacy of myopia control using ortho-k with higher compression factor. Although an extra 1 D target was added in the ICF group, there was only 0.30 D difference in the manifest refractive sphere between ICF and CCF groups. The results were in agreement with an earlier short-term study.24 The under-correction could be due to several factors. The first factor could be the time of data collection. The amount of manifest refraction could be dependent on the time of day when the measurement was made, the reported daytime regression by previous investigators was about 0.25 D to 0.50 D3 25 26 or even less than 0.25 D27; however, this factor should affect both the ortho-k groups and contribute minimally to the between-group difference. Although this factor could potentially affect the measured manifest refraction, subjects could not all be measured at the same time because of the limited resources. In this study, all measurements were performed during daytime and the diurnal variation was controlled by scheduling all the data collection visits at about the same time of day as the baseline visit. The second potential contributing factor could be the relatively short wearing period: the increased target may take a longer time to stabilise, although a previous study has shown that the manifest refractive power stabilised after 1 month of lens wear.27 Another explanation is that there may be a corneal mechanism, which is related to the corneal structural properties,28 that could limit the amount of corneal changes, hence affecting the manifest refractive power changes.
Peripheral corneal steepening along with the corneal power change induced in ortho-k will affect the peripheral retinal defocus. Three studies have investigated the association between the post-ortho-k corneal power change and axial elongation and revealed that a higher amount of corneal power change was associated with better retardation in axial elongation,17–19 although one study20 reported contradictory findings of no association between corneal power change after short-term and long-term ortho-k lens wear and eye growth. The discrepancies may be due to differences in defining the corneal region and the amount of corneal power change in each study.
The exact mechanisms for optical treatments, including ortho-k, in retardation of axial elongation are still unclear. One popular hypothesis for the effect of slowing axial elongation is that it is due to myopic defocus induced by the optical interventions.16 29 30 The effect of retinal defocus on axial elongation using animal models is well documented.31–33 There appears to be no significant correlation found between peripheral refraction and myopia progression in humans.34 However, myopia progression may be related to the hyperopic defocus and higher-order aberration of the eye.35–38
It has been shown that in a contralateral self-controlled study, increasing the compression factor by 1.00 D significantly increases the incidence of ocular higher-order aberrations, primarily spherical aberration.36 This increase could therefore improve the myopia control efficacy as axial elongation has been shown to be related to a visually driven mechanism.35 37 38 Lau et al have shown that higher-order aberration was associated with axial elongation; however, because of the study design, it is unclear whether the effect was due to change in aberration as a result of refractive correction or change in aberration due to normal ageing.39 Ocular higher-order aberrations are also measured in the current study and these will be investigated at the end of this study, after 2 years of lens wear.
The initial AL shortening after commencement of ortho-k treatment was significantly higher in the ICF group after 1 month of lens wear, which is in agreement with our previous study.40 The anterior segment length has been shown to be unaffected by ortho-k lens wear41 and CCT thinning in the ICF group only accounted for around 30% of the total AL shortening after 1 month of lens wear. The source of the remaining AL shortening was unclear, although it has been suggested to be due to thickening of the choroid.42 Retinal defocus in animals and human studies43–47 have demonstrated choroidal thickness changes both in response to exposure to spectacle lenses of myopic46 or hyperopic defocus,47 and in ortho-k-treated eyes.48 49 Again, the choroidal thickness changes and its association between the AL will be investigated at the end of this longitudinal study.
Originally, this current longitudinal study was planned as a randomised clinical trial with three arms; however, because of the popularity of using ortho-k lenses as a treatment in controlling myopia progression in Hong Kong, a partially randomised study design has to be adopted, owing to the high refusal rate in the control group. Popularity of ortho-k for myopia control is likely to be linked to the increase in evidence of the ability of ortho-k to slow myopia progression.9–15 An investigation of parents’ knowledge of methods for myopia control in Hong Kong revealed that ortho-k was the most widely known method.50 Parents are concerned about myopia progression and eager to seek ortho-k treatment for their children, leading to difficulties in recruitment of control subjects in recent studies, making a fully randomised study design impractical.
The spherical power achieved at 1 month for the ICF group was significantly more hyperopic than that of the CCF group. Despite a higher amount of refractive error correction, which might imply a higher exertion of pressure on the cornea, there were no significant differences in external ocular health, in terms of corneal staining between the two ortho-k groups. As well as corneal staining, pigmented arc is another commonly observed change at the mid-peripheral cornea after commencement of ortho-k wear.51 52 A pigmented arc was found in one subject in the CCF group at the 1-month visit and none in the ICF group. Although the refractive change was more rapid in the ICF group, the formation of a pigmented arc was not enhanced in the ICF group, at least, not in the first month of lens wear.
In conclusion, the preliminary results of this study indicated that the increased 1 D in compression factor increased myopia correction without compromising ocular health or the first fit success rate. ICF ortho-k lenses are therefore safe to be used by children and could reduce the time for children to achieve full refractive correction. This study is the first long-term longitudinal study to investigate the differences in efficacy of myopia control and ocular responses between ICF and CCF ortho-k. The results of this study may lead to development of a new ortho-k lens design and provide a better understanding of the mechanism of ortho-k in slowing axial elongation.
Acknowledgments
The authors thank Dr Maureen Boost for her advice in the preparation of the manuscript. The authors also thank Mr Bill Yau for his assistance in the transformation of refractive data into Long’s formalism.
References
Footnotes
Contributors All authors designed and planned the study. KW and JKL conducted the experiment. KW analysed the data and wrote the first draft of the paper. All authors interpreted the results, revised the manuscript and approved the final version of the work.
Funding KW and JKL are supported by the Research Residency Scheme provided by The School of Optometry of The Hong Kong Polytechnic University (PolyU). This study is supported by a Collaborative Research Agreement between PolyU and Menicon Co. Ltd., Japan (ZG3Z). Saline and artificial tears are supported by Ophtecs Co., Japan.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval All procedures are performed in accordance with the tenets of the Declaration of Helsinki. Ethics clearance has been obtained from the Departmental Research Committee of the School of Optometry at The Hong Kong Polytechnic University (HSEARS20150909002-01).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.