Article Text

Abstract
Objective Studies have shown that hypertensive disorders of pregnancy (HDP) are associated with both postpartum retinal microvascular changes and cardiovascular (CV) risks. However, the underlying mechanism of HDP transitioning to microvascular and macrovascular changes remains unknown, due to the interaction between microvasculature and CV risks. In this study, we examined whether associations between antenatal systolic blood pressure (SBP) and postpartum retinal arteriolar changes are independent of postpartum CV risks.
Methods We included 276 Singaporean mothers attending both baseline index pregnancy (2009–2010) and 5-year postpartum follow-up visits (2014–2015). We measured SBP at baseline. At follow-up, we assessed retinal microvascular structure and function with retinal photography and dynamic vessel analyser, together with CV risks using a validated 2008 Framingham Risk Score (FRS). We performed a traditional four-step mediation analysis using linear regression by adjusting for a series of baseline characteristics: age, ethnicity, college degree, prepregnancy body mass index and gestational diabetes mellitus diagnosis at baseline.
Results We found that each 10 mm Hg increase in baseline SBP was associated with reduced arteriolar calibre (−1.3 µm; 95% CI −3.0 to 0.2) and fractal dimension (−0.4 degrees of freedom (df); −1.0 to 0.2), and significantly with increased arteriolar constriction (0.5%; 0.001 to 1.0) at 5-year postpartum. Even though baseline SBP was associated with postpartum FRS, the latter was not associated with any retinal arteriolar measures. Therefore, no further mediation analysis was required.
Conclusion Our study suggested that elevated SBP during pregnancy was associated with suboptimal retinal arteriolar structure and function independent of postpartum CV risks.
- epidemiology
- imaging
- public health
- retina
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of the study
What is already known about this subject?
Elevated antenatal blood pressure was found to be associated with 5-year postpartum retinal microvascular changes in mothers.
What are the new findings?
The association found above was not mediated by postpartum cardiovascular (CV) risk assessed by Framingham Risk Score.
How might these results change the focus of research or clinical practice?
Our findings suggested that the pathophysiology between elevated antenatal blood pressure and postpartum arteriolar abnormality in both function and structure is independent of increased CV risk as assessed with established risk stratification scoring system. Future studies should examine other forms of CV risks that might underlie microvascular dysfunction in mothers with history of gestational hypertensive disorders.
Introduction
Emerging evidence has shown that hypertensive disorders of pregnancy (HDP) are associated with postpartum microvascular changes,1 2 such as retinal arteriolar narrowing and venular widening. Since antenatal blood pressure (BP) is also known to increase a series of cardiovascular (CV) risks such as insulin resistance,3 oxidative stress and endothelial dysfunction,4 it is unclear whether previous findings of antenatal BP and postpartum microvascular alteration are mediated by CV risks.
In this study, we explored the potential mediating role of CV risks in the association between antenatal BP and postpartum retinal vasculature. Furthermore, in order to align with our previous findings that women at risk of HDP were inclined to have abnormal retinal arteriolar morphology (ie, calibre narrowing, fractal dimension reduction and branching angle enlargement),5 we only investigated the association between antenatal systolic BP (SBP) and postpartum retinal arteriolar structural and functional changes, and the potential mediating role of postpartum CV risks. We hypothesised that postpartum CV risks might partially mediate the association between antenatal SBP and changes in postpartum retinal arteriolar structure and function.
Materials and methods
Study population: patient and public involvement
This is an exposure-matched, prospective observational study, embedded within an ongoing birth cohort (Growing Up in Singapore Towards Healthy Outcomes, GUSTO) in Singapore.5 We recruited 1136 women with singleton pregnancies during their first trimester from June 2009 to September 2010. Our study population consisted of 276 women who attended both baseline index pregnancy (26–28 weeks gestation) and follow-up (5 years after delivery) visits, as detailed in our previous publication.5
Exposure: antenatal systolic and diastolic blood pressure
All subjects underwent BP evaluation according to standardised protocols, using the automatic Omron sphygmomanometer (Dinamap, carescape V100, GE, USA) during baseline recruitment. All mothers sat upright with back support with a cuff around their non-dominant upper arm after resting for at least 5 min. We took the average of two separate measurements on both SBP and diastolic blood pressure (DBP), and a third measurement if the first two readings differed by 5 mm Hg.
Outcome: 5-year postpartum retinal arteriolar microvascular structural and functional measures
We performed digital retinal photography on both eyes with pupil dilation at the 5-year follow-up visit, using a 45° non-mydriatic retinal camera (Canon CR-1, 40D SLR digital retinal camera backing; Canon, Tokyo, Japan). A trained grader assessed the best-quality retinal image centred on the optic disc of each eye using a semiautomated computer-based programme (Singapore I Vessel Assessment, V.4.0, Singapore Eye Research Institute, Singapore) following a standard protocol.5 We masked trained graders to the participants’ identity and gestational diabetes mellitus (GDM) status. Graders assessed retinal microvascular variables quantitatively within a zone 0.5–2.0 disc diameters from the optic disc margin. We assessed intragrader reliability using 10% (n=27) of randomly selected retinal images from the same study. The intraclass correlation coefficient was above 0.80 for all retinal vascular variables.
We introduced the measurements of retinal vascular structure and function a priori.5 We used diffused luminance flickering light to induce vasodilatation in both arterioles and venules, and such phenomenon measured by the dynamic vessel analyser (DVA) has been described as functional hyperaemia or neurovascular coupling. We observed transient constriction several seconds following vascular dilatation only in arterioles.6 In this study, only retinal arteriolar measures in structure and function were used for analysis.
Potential mediator: 5-year postpartum CV risks assessment
As a proxy of CV risk, we scored these 276 patients at the 5-year follow-up visit using the 2008 Framingham Risk Score (FRS) scaling system,7 which predicts a 10-year risk of a series of CVD events based on subjects’ age, levels of high-density lipoprotein (HDL), total cholesterol, SBP or history of medicated hypertension, smoking status and diagnosis of diabetes mellitus (online supplementary file 1). Although originally developed for use in Western populations, it has been shown to be compatible in multiethnic populations8 and even useful for a 10-year prediction of coronary heart disease, particularly in Asian women.9 We assessed mothers’ 5-year postpartum FRS based on a list of variables defined below:
Supplemental material
Lipid profile: We collected the participants’ blood samples via venipuncture for measurement of cholesterol levels (HDL, low-density lipoprotein and total cholesterol).
Diagnosis of diabetes mellitus: We conducted a 2-hour 75 g oral glucose tolerance test after the participants had fasted overnight for 8–10 hours. We defined type 2 diabetes as (1) fasting plasma glucose ≥7.0 mmol/L and/or 2-hour plasma glucose ≥11.0 mmol/L10 or (2) based on self-reported history of diabetes in the questionnaire.
Smoking: We obtained information regarding the current and past smoking status and the number of cigarettes smoked per day using interviewer-administered questionnaires.
SBP or history of medicated hypertension: SBP was measured with the same protocol mentioned above at the 5-year follow-up visit, and history of medicated hypertension was collected by self-recalled medical history.
Covariates
Trained staff collected information on age, college education, pregnancy history (parity, past HDP and past GDM), family history of diabetes mellitus and self-reported history of hypertension via questionnaires, at the baseline and 5-year follow-up visit. We collected information on prepregnancy weight only at the baseline visit. We measured weight and standing height using a calibrated weighing scale and stadiometer (SECA model 803 and 213, respectively, Seca, Hamburg, Germany) according to standardised protocols5 and calculated body mass index (BMI) as (weight in kilograms)/(height in metres)2.
Statistical analysis
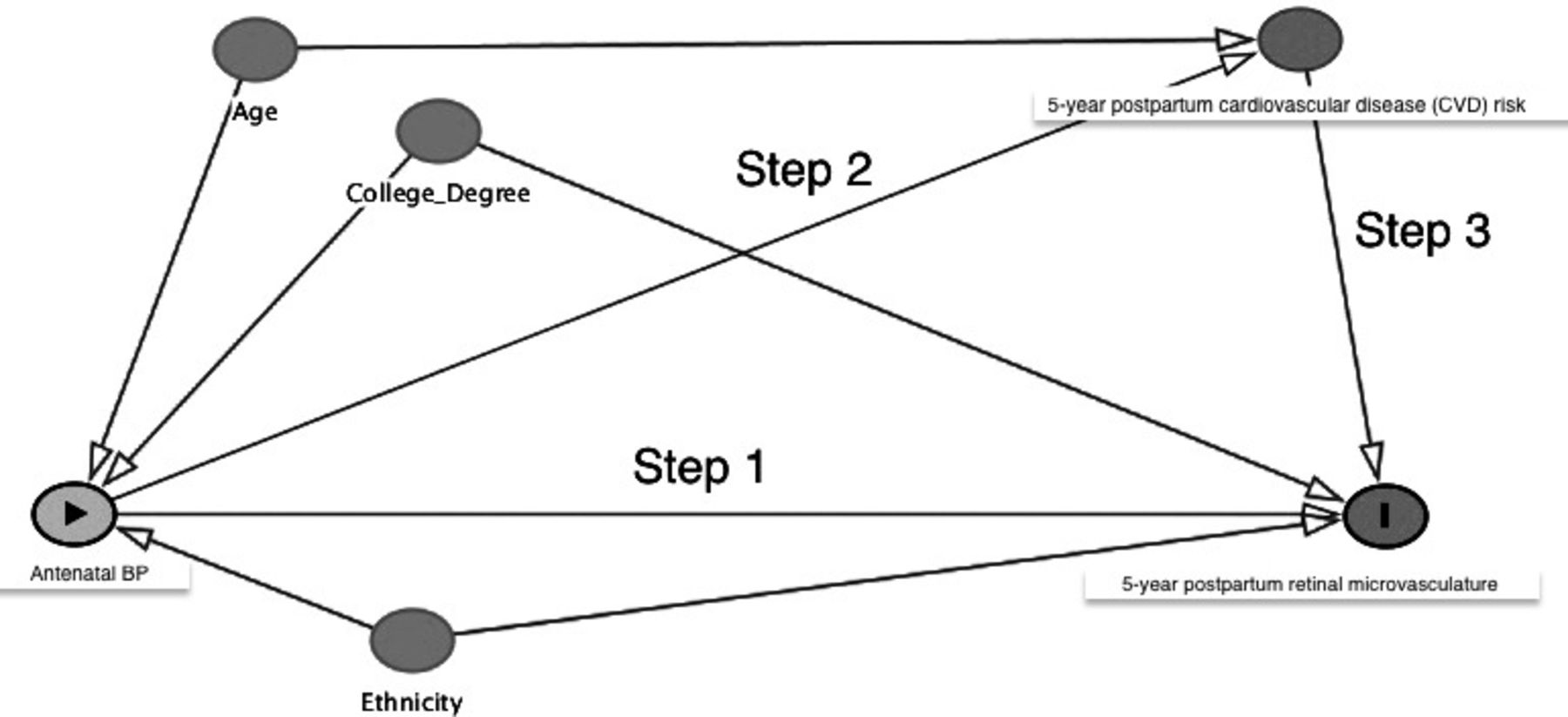
We reported mean and SD for continuous variables and count and percentages for categorical variables. We performed a mediation analysis using the following conventional regression approaches.11Step 1: examined the association between antenatal SBP and 5-year postpartum retinal arteriolar microvasculature; step 2: examined the association between antenatal SBP and 5-year postpartum FRS; step 3: examined the association between 5-year postpartum FRS and 5-year postpartum retinal arteriolar structural and functional measures; step 4: examined the mediating effect of 5-year postpartum FRS on the relationship between antenatal SBP and 5-year postpartum retinal arteriolar structural and functional measures. All steps are illustrated in the directed acyclic graph (DAG) demonstrated in figure 1.

{kind=link}
Directed acyclic graph depicting the traditional four-step mediation analysis using conventional regression approaches. BP, blood pressure.
We performed sensitivity analyses to test the robustness of all our final adjustments, with the inclusion of baseline variables such as family history of diabetes, parity, history of GDM, use of in-vitro fertilisation and weight gain until 26–28 weeks of gestation (calculated as the difference between weight at prepregnancy and weight at 26–28 weeks gestation). We set a two-tailed p value for significance at 0.05 and provided the 95% CI for all estimates.
Results
Table 1 shows the baseline demographics and 5-year postpartum ocular parameters of our participants. The mean age and SBP of the study participants at baseline were 33.0±4.9 years and 110.4±13.0 mm Hg, respectively, and 54.3% (n=150 out of 276) were of Chinese ethnicity. The prepregnancy BMI was 26.9±4.1 kg/m2, 42.8% (n=118 out of 276) of them had a college degree and 51.4% (n=142 out of 276) of them had the diagnosis of GDM.
Characteristics of mothers at baseline (26–28 weeks gestation) and follow-up (5 years after delivery)
Table 2 shows the associations of antenatal SBP at baseline and retinal arteriolar structural and functional measures at the 5-year follow-up, which demonstrates step 1 of our planned mediation analysis. After adjustment for age, ethnicity and college degree, each 10 mm Hg increase in baseline SBP was significantly associated with reduced retinal arteriolar calibre (β −1.1 µm; 95% CI −2.2 to 0.04) and fractal dimension (−0.6 degrees of freedom (df); –1.1 to –0.1) and increased arteriolar constriction (0.3%; 0.02 to 0.7). After further adjusting for GDM diagnosis and prepregnancy BMI at baseline, the associations for retinal arteriolar calibre (−1.3 µm; −3.0 to 0.2) and fractal dimension (−0.4 df; −1.0 to 0.2) attenuated to non-significance, while DVA constriction remained significant (0.5%; 0.001 to 1.0). We did not find any significant change on the sensitivity analysis.
Associations of antenatal systolic blood pressure at baseline and retinal arteriolar structural and functional measures at 5-year follow-up
Table 3 shows the association between baseline antenatal SBP and 5-year postpartum FRS, which demonstrates step 2 of our planned mediation analysis. Baseline SBP was consistently associated with elevated postpartum FRS in three models. In the fully adjusted model, each 10 mm Hg increase in antenatal SBP was significantly associated with a higher postpartum FRS (0.7; 0.04 to 1.4).
Associations between antenatal systolic blood pressure at baseline and cardiovascular risk score (Framingham Risk Score) at 5-year follow-up
Table 4 illustrates step 3 of our planned mediation analysis. Each point increase in FRS was associated with reduced retinal arteriolar fractal dimension (−0.3 df; −0.5 to –0.04) in the unadjusted model with a p value of 0.02 (p<0.05) and is hence statistically significant. However, after full adjustment, the association was no longer significant. After adjusting for age, ethnicity and college degree, the p value was 0.15 (p>0.05) and hence not statistically significant. After additionally adjusting for GDM diagnosis and prepregnancy BMI at baseline, the p value remained not statistically significant at 0.14 (p>0.05). Therefore, this precludes FRS as a potential mediator, and thus, step 4 of the mediation analysis was not justifiably required.
Associations between cardiovascular risk score (FRS) and retinal arteriolar structural and functional measures both at 5-year follow-up
Discussion
In this multiethnic Asian cohort, we found that elevated antenatal SBP was associated with 5-year postpartum increased retinal arteriolar constriction and borderline associated with reduced retinal arteriolar calibre and fractal dimension. Even though antenatal SBP was associated with 5-year postpartum CV risks assessed via FRS, this score did not appear to mediate the underlying relationship between antenatal SBP and 5-year postpartum retinal arteriolar changes.
Existing evidence suggests that the earliest changes in the pathogenesis of hypertension are changes in the structure and function of the microcirculation,12 suggesting that antenatal BP is associated with changes in small vessels. With the introduction of digital retinal photography in the recent decades, the state-of-the-art technique of quantitatively assessing retinal vascular network has been widely adopted and retinal microvasculature has been suggested as the ‘window’ to systemic microcirculation.13 Since retinal circulatory architecture conforms to optimally designed principles,14 any deviation from this architecture (eg, arteriolar narrowing, venular widening, larger branching angle and lower fractal dimension) has been hypothesised to be a proxy of less efficient and impaired microcirculatory transport.15 Aligned with such hypothesised pathophysiological changes on retinal vessels impacted by elevated blood pressure, our key finding is that elevated antenatal SBP was associated with increased 5-year postpartum retinal arteriolar constriction and to a lesser extent, reduced retinal arteriolar calibre and fractal dimension. Even though some associations (ie, antenatal SBP and arteriolar calibre and fractal dimension) were attenuated after adjusting for major confounders, the trend of similar estimates remained similar.
Another key finding that our study shows is that antenatal SBP was associated with 5-year postpartum CV risks assessed via FRS. Prior studies showed that HDP was associated with changes in retinal arteriolar narrowing and venular widening, at both perinatal and postpartum phases. Both HDP and subsequent retinal vascular changes may be mediated by CV risks as HDP induces endothelial changes in both macrovaculature and microvasculature.16 Furthermore, elevated constriction in arterioles has been shown to increase CV risks by contributing to increased vascular tone and slower blood flow and correlates with clinical cardiovascular outcomes (eg, cardiovascular mortality), markers of subclinical vascular disease (eg, carotid plaques and coronary calcifications)5 as well as markers of inflammation such as C reactive protein.17 One valid way to explore this is to apply mediation analysis. In this pilot study, we performed a traditional four-step approach for mediation analysis, yet found no associations between FRS-represented CV risks and postpartum retinal vasculature. A possible explanation could be that our study was underpowered due to our small sample size. Moreover, FRS may not be a good indicator of CV risk over a short period (ie, less than 10 years).
Our pilot study only focused on SBP, as it has been shown to be a stronger clinical predictor of CV risk than DBP,18 19 especially in Asian populations.20 Furthermore, we only focused on retinal arteriolar measures, due to substantial evidence21 including our prior findings5 that had demonstrated a more consistent association of retinal arteriolar changes instead of venular changes with elevated BP. Such a mechanism has been hypothesised as vasoconstriction of peripheral arterioles, growth and apoptosis of smooth muscle cells of peripheral arterial wall5 which venules lack,22 which supports our observation of elevated SBP and retinal arteriolar narrowing, more scarce retinal arteriolar fractal dimension and increased retinal arteriolar constriction.
The strengths of our study include the prospective study design, a relatively long follow-up period (5 years after delivery), a decent sample size (n=276) and standardised protocols for exposure and outcome measurements. However, our limitations include the lack of local cardiovascular risk score to appropriately stratify risk in our multiethnic Asian cohort, potential selection bias due to loss to follow-up and residual bias due to unmeasured confounding.
In summary, our data showed that higher antenatal SBP is associated with 5-year postpartum retinal arteriolar changes. Although antenatal SBP was associated with 5-year postpartum FRS, which is a proxy of CV risks, our findings did not identify a mediating role of postpartum CV risks in the association between elevated antenatal SBP and postpartum retinal arteriolar changes.
References
Footnotes
Contributors We declare here that all authors have read and approved the submission of the manuscript; the manuscript has not been published and is not being considered for publication elsewhere, in whole or in part, in any language. All authors have contributed significantly and are in agreement with the content of the manuscript. RS conducted the literature review, drafted the manuscript and conducted data analysis and interpretation. IMA supervised the data analysis, helped interpret the data and edited the manuscript. YSC designed the study and edited the manuscript. TYW supervised the data analysis and edited the manuscript. L-JL designed the study, directed its implementation, designed the study’s analytical strategy, reviewed and edited the manuscript.
Funding This study was funded by Singapore National Medical Council Transition Award, grant number: NMRC TA/0027/2014, NMRC/CG/C008A/2017_KKH and Singapore National Medical Council, grant number: NMRC/CNIG/1114/2013.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: this study is funded by the Singapore National Medical Council (NMRC/CNIG/1114/2013), L-JL is funded by a Singapore National Medical Council Transition Award (NMRC/TA/ 0027/2014). The GUSTO cohort, under the Translational Clinical Research (TCR) Flagship Program on Developmental Pathways to Metabolic Disease, is funded by the Singapore National Research Foundation (NRF) and administered by the Singapore National Medical Research Council (NMRC/TCR/004-NUS/2008). The authors declare no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Patient consent for publication Not required.
Ethics approval We obtained approval from the SingHealth Centralised Institutional Review Board and the National Health Group’s Domain Specific Review Board. We conducted the study according to the tenets of the Declaration of Helsinki and obtained informed written consent from each participant at the 5-year follow-up visit.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.