Article Text

Abstract
Plateau iris syndrome (PIS) is a frequent cause of angle closure. Argon laser peripheral iridoplasty (ALPI) has been proposed in PIS to widen the iridocorneal angle. The objective of the present study was to perform a systematic review of the available studies evaluating the efficacy of ALPI on intraocular pressure (IOP), iridocorneal angle opening and the number of medications in patients with chronic angle-closure associated with PIS. One prospective and seven retrospective studies with a minimum 1 month of follow-up were included. Although ALPI seemed to lower IOP, to decrease the number of topical antiglaucoma medications and widen the iridocorneal angle shortly after the procedure, there is no current evidence of long-term efficacy. To date, there is no robust scientific evidence to advocate ALPI as a treatment for chronic angle-closure caused by PIS.
- Glaucoma
- Iris
- Treatment Lasers
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Of the nearly 67 million patients with glaucoma worldwide, primary angle-closure glaucoma (PACG) is a major cause of blindness, and it is estimated that 5.3 million people will suffer from blindness secondary to PACG in 2021.1 Relative pupillary block is considered to be the primary mechanism for angle closure, making laser peripheral iridotomy (LPI) a treatment of choice in PACG. LPI is able to significantly increase angle width and to lower intraocular pressure (IOP) in people with narrow angles.2 3 However, several studies reported patients with persistent angle closure after LPI (around 58%–80% of cases) in which the most common underlying mechanism was plateau iris.2 4
Tornquist et al5 first described the plateau iris configuration in 1958 on a young woman with high IOP and a flat iris surface. Gonioscopic examination revealed a closed-angle with a double-hump iris. Then plateau iris was classified by Wand et al6 in 1977, differentiating ‘plateau iris syndrome’ from ‘plateau iris configuration’. The ‘configuration’ refers to a preoperative condition with a gonioscopically confirmed narrow-angle and a flat iris. In most cases, the narrow angle associated with the plateau iris configuration was opened by a peripheral iridotomy. ‘Plateau iris syndrome’ (PIS) refers to a persistently narrow angle capable of closure despite a patent iridotomy resolving the associated relative pupillary block component. Wand et al7 confirmed and illustrated their observations in 1993 with histological and ultrasound biomicroscopy (UBM) exploration, showing an anteriorly displaced ciliary body that may secondarily rotate and push forward the peripheral iris root into the trabecular meshwork, causing angle narrowing or closure with a flat iris. As a consequence, PIS is now regarded as one of the mechanisms of angle-closure glaucoma.8
In 1982, after observing angle widening in front of an iridotomy site, Ritch9 proposed repeated non-transfixing spots on the iris periphery, describing the first argon laser peripheral iridoplasty (ALPI). ALPI contracts the peripheral iris tissues, pulling the iris away from the trabecular meshwork and reducing the area of iris–trabecular contact. Although ALPI is still considered as a laser treatment for PIS management, since 1982 and the first ALPI description, only a few studies have been conducted on this technique for PIS management.
The purpose of this study was to evaluate the efficacy and safety of ALPI on IOP lowering, angle opening and the number of medications in PIS by reviewing the available published literature.
Patients and methods
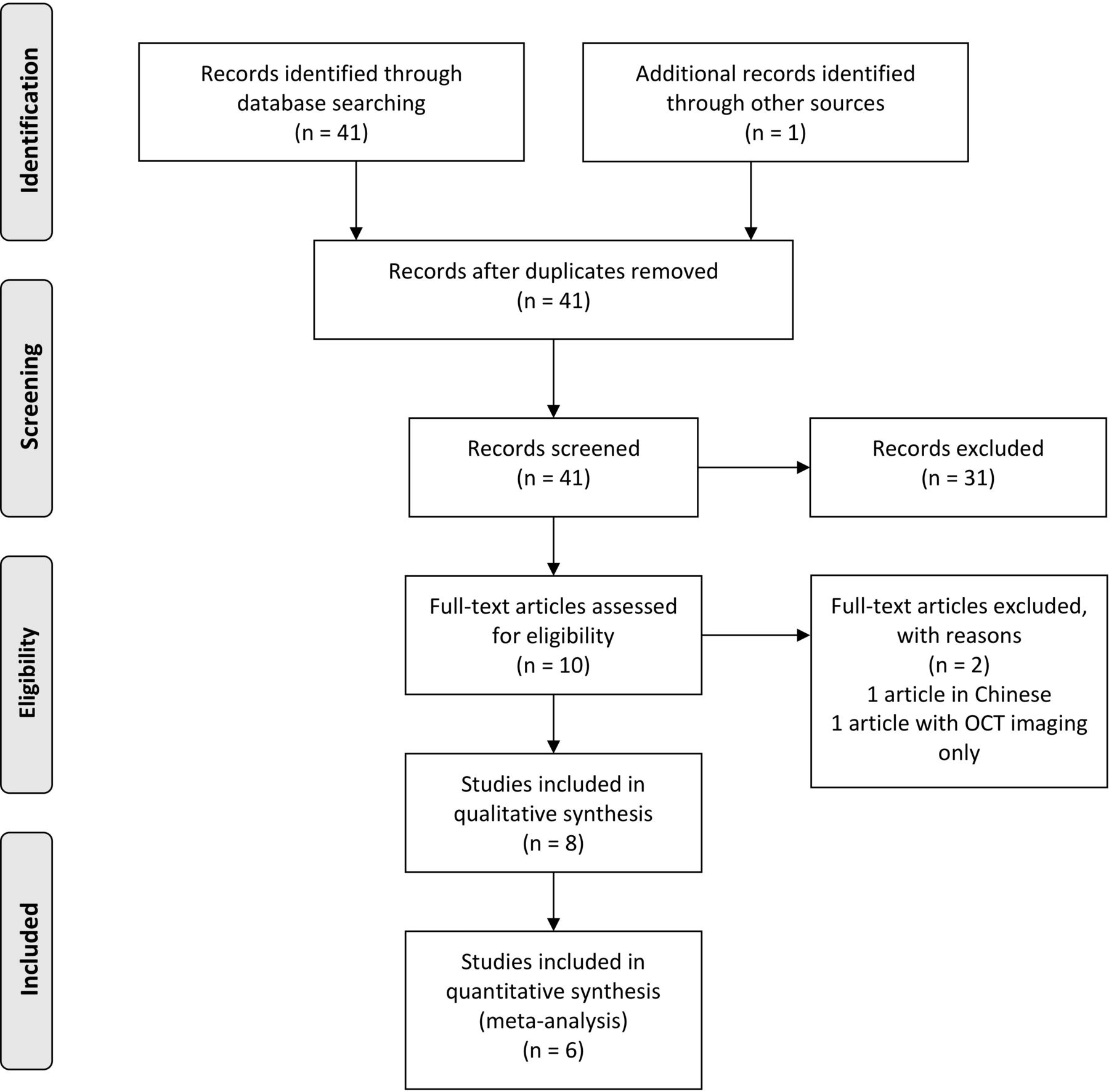
We conducted a systematic review of studies evaluating the efficacy of ALPI in PIS. The published literature was searched using the following keywords: (“Plateau iris” AND “Laser iridoplasty”) OR (“Plateau iris” AND “Gonioplasty”) OR “Iridoplasty”. We analysed all the prospective and retrospective cohorts evaluating ALPI in documented chronic ACG caused by PIS. We included studies that evaluated IOP lowering, angle opening and/or the number of medications with a 1-month minimum follow-up. A total of 41 articles were analysed of which 33 were excluded (figure 1). The reasons for exclusion are detailed in online supplementary annex 1. We provided an individual and an overall analysis for 1-year and 6-year outcomes. Weighted mean IOP (WMIOP) was calculated for 1-year and 6-year outcomes using each study’s final IOP weighted by the number of eyes included in the final evaluation:
Supplemental material


Flow chart.
Results
To date, there have been no randomised controlled trials evaluating the use of iridoplasty in chronic angle-closure caused by PIS. We included seven retrospective case series4 9–15 and one prospective observational case–control study16 published between 2004 and 2017. The study characteristics are described in table 1. A total of 170 eyes of 147 patients were analysed. The eight studies were conducted on patients with chronic angle-closure persistent after laser peripheral iridotomy. Three studies included both PIS and lens-induced angle closure11 13 16 and five evaluated PIS only.4 10 12–15 17 One study provided a 1-month follow-up,15 five studies a 12-month follow-up,11–13 16 two studies had a long-term follow-up of more than 6 years4 17 and the longest one provided 92.4 months of mean follow-up.10
Study characteristics
The ALPI procedure was not standardised and differed slightly between studies: spot sizes varied from 200 to 500 µm, energy levels from 200 to 550 mW and exposure times from 100 to 500 ms (table 2). The number of spots was specified in four studies and varied from 20 to 50.10 14–16 The procedures were performed in one session, except for Ouazzani et al,15 who performed ALPI in two sessions, with or without a contact lens to put non-overlapping spots on 360° of the peripheral iris. The primary efficacy outcome was a clear iris contraction for each laser application in all the studies presented. All procedures included postoperative steroidal or non-steroidal anti-inflammatory drugs and IOP control 45–60 min after the procedure.
ALPI procedures
Individual study analyses
Romito et al10 conducted a retrospective non-controlled interventional case series with 53 ALPI procedures performed in 48 eyes of 28 patients with PIS confirmed by UBM. The mean follow-up was 92.4±26.5 months. IOP varied from 15.92±2.62 mm Hg at baseline to 14.35±2.19 mm Hg (p>0.001) at the end of follow-up, with a non-significant augmentation in the number of medications from 0.81±0.94 to 1.2±1.04 (p>0.001). Five eyes required a repeated ALPI procedure 60.2±15.8 months after the first one justified by a persistent appositional closure on dynamic gonioscopy. No filtration surgery was required, but 21% of the eyes underwent SLT and 10% phacoemulsification warranted by a significant loss of vision caused by cataract.
Ritch et al17 conducted a retrospective, non-controlled interventional case series with 26 ALPI procedures performed in 23 eyes of 14 patients with chronic angle-closure and PIS requiring pilocarpine or IOP-lowering drugs. The mean follow-up was 78.9±8.0 months. IOP varied from 18.0±4.5 mm Hg at baseline to 18.2±4.5 mm Hg at the end of follow-up with a reduction in the number of medications from 1.2±1.0 to 0.6±0.7 (NS). The angle in 20 of 23 (87.0%) eyes stayed open throughout the entire follow-up period after only one ALPI procedure. In three eyes, there was a gradual angle narrowing 5–9 years after initial ALPI, but it was permanently reopened by a single differed treatment. No filtration surgery was necessary in any eye during follow-up.
Peterson et al4 retrospectively reviewed 22 eyes of 22 patients who underwent ALPI for a persistent iridotrabecular apposition after LPI caused by PIS with a mean 76-month follow-up. The mean IOP was 21.3±7.1 mm Hg before ALPI, 16.9±3.3 after 1 year (p=0.012), 16.5±3.9 (p=0.002) after 2 years, 17.2±4.2 (p=0.016) after 3 years, 16.6±2.7 (p=0.014) after 4 years, 18.3±3.2 (p=0.062) after 5 years and 19.7±6.4 mm Hg (p=0.038) at the end of follow-up (p=0.38). Only two (9%) eyes maintained an IOP <21 mm Hg without medications or surgery, and 17 eyes (77%) underwent surgery an average of 49.1±7.9 months after ALPI. Eight eyes (36%) underwent filtering surgery and nine eyes (41%) underwent phacoemulsification. Both results on IOP and the number of medications became non-significant between the fourth and fifth year of follow-up, and consequently, ALPI efficacy could not be ruled out with certainty.
Ramakrishnan et al16 conducted a prospective, observational case–control study with a 1-year follow-up. They included 16 eyes of 12 patients and among them 8 eyes had angle closure due to PIS and 8 had primary angle closure. All patients had a previous LPI without angle opening. When considering the entire population, there was a significant decrease in IOP from 24.4±5.6 mm Hg to 16.5±5.4 mm Hg (p<0.001) at the end of follow-up. However, there was no specific analysis for patients with PIS in that study. Gonioscopic examination focused on peripheral anterior synechiae (PAS) that were reduced from 3.5 to 2.5 clock hours (p<0.001). They also confirmed their observations with anterior-segment optical coherence tomography (AS-OCT) showing an angle opening depth (AOD500) increasing from 0.132±0.016 at baseline to 0.179±0.062 mm (p<0.001) at 1 year. The mean number of antiglaucoma medications decreased from 1.6±0.9 to 0.7±1.1 (p<0.001). There was no subgroup analysis focusing on PIS only. This study was the only study reporting adverse events with 20% IOP spikes, 16% iris haemorrhages and 4% persistent intraocular inflammation at 1 week.
Junqueira et al11 conducted a 1-year retrospective chart review of 27 patients who underwent ALPI for persistent occludable angles after laser peripheral iridotomy. The most common underlying mechanisms were plateau iris (56%) followed by lens-induced angle closure (34%). Considering the entire population, IOP was significantly reduced from 17.9±4.9 mm Hg to 14.5±4.2 mm Hg (p<0.01) at the end of follow-up, with no significant differences between patients with PIS and lens-induced angle closure (p=0.34). Approximately 90% of the eyes had a non-occludable angle defined as a posterior trabecular meshwork visible on 180° without indentation on gonioscopic examination following ALPI. The number of medications was not evaluated in this study.
Singh et al12 conducted a retrospective review on 12 eyes of 8 patients with PIS confirmed by UBM, who required medical treatment and underwent ALPI with a 1-year follow-up. A statistically significant IOP reduction was found after 1 year from 20.6±4.8 mm Hg to 17.8±3.8 mm Hg (p=0.01). Angle widening was noted in 46% of the treated quadrants by at least one grade (Shaffer’s classification) after 1 month of follow-up. There was no significant change in the number of medications.
In a 1-year retrospective study, Gomes Prado et al13 investigated 35 eyes of 21 patients: 56% of eyes were clinically diagnosed with PIS, 34% had lens-induced angle closure and 10% had other causes of angle closure. Considering the entire population, IOP was significantly reduced from 18.2±4.7 mm Hg to 14.6±3.8 mm Hg (p<0.01) with no significant difference between PIS and lens-induced subgroups. The value of this study was the absence of change in the treatment regimen during the entire follow-up with 1.5±1.1 medications. After ALPI, 91% of the patients showed non-occludable angle in gonioscopy without specifications on the examination criteria.
Ouazzani et al15 investigated nine eyes of five patients who underwent ALPI for PIS with glaucoma diagnosed by dynamic gonioscopy. The mean IOP before ALPI was 21.1 mm Hg, which decreased to 14.4 mm Hg at 1 month (no statistical analysis). After the procedure, hypotensive treatment could be withdrawn for four eyes. No data were collected on angle opening.
Effect on IOP
After ALPI, IOP decreased from −6.7 mm Hg (−30%) after 1 month15 to −2.8 mm Hg (−19%) (p=0.01),12 −3.4 mm Hg (−19%) (p<0.01),11 −3.6 mm Hg (−20%) (p<0.01),13 −4.4 (−21%) (p=0.012)4 and −7.9 mm Hg (−32%) (p<0.001)16 after 1 year. After a mean follow-up of 6 years, Ritch et al17 did not find any significant IOP change as compared with baseline (+0.2 mm Hg), similar to Peterson et al,4 who found a −1.6 mm Hg (p=0.38) non-significant IOP variation. Moreover, in this study, 36% eyes underwent filtering surgery and 41% eyes phacoemulsification. After 7.5 years of follow-up, Romito et al10 found a −1.56 mm Hg (−10%) (p>0.01) variation. IOP changes are presented in table 3.
IOP and angle widening variations (IOP in mm Hg)
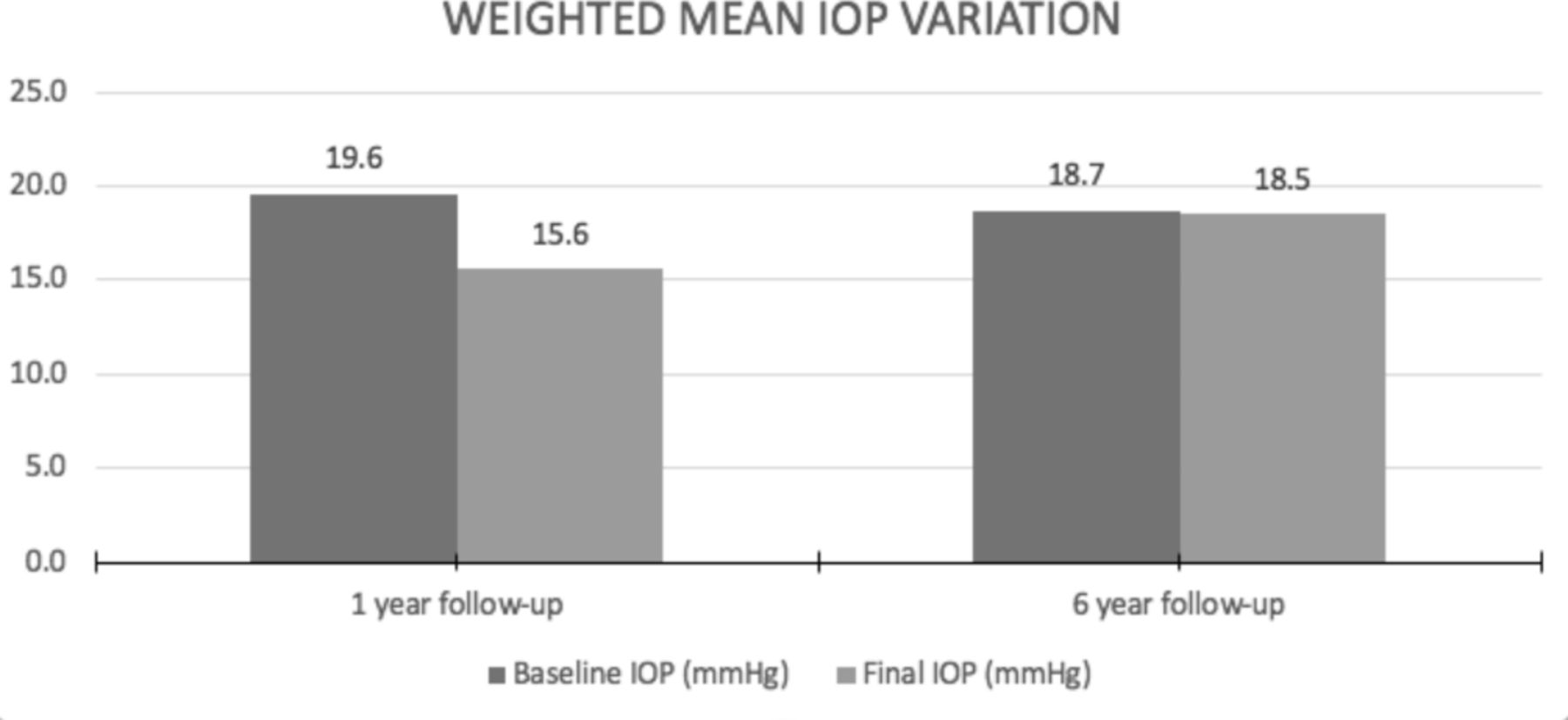
In studies with at least 1 year of follow-up, weighted IOP decreased from 19.6 mm Hg at baseline to 15.6 mm Hg at the last visit after ALPI, providing a −4.0 mm Hg or −20% IOP variation.4 11–13 16 In the studies with a 6-year follow-up, weighted mean IOP varied from 18.7 mm Hg to 18.5 mm Hg at the last visit after ALPI, providing a −0.2 mm Hg or 1% variation4 17 (figure 2).
{kind=link}
{kind=link}
Weighted mean IOP variation (IOP, intraocular pressure; n year, indicate follow-up time).
Effects on angle widening
Iridocorneal angle changes after ALPI were evaluated with gonioscopy in seven studies. Initial PIS evaluation was confirmed by UBM in four studies4 10 11 16 and AS-OCT in one study.16 The final angle evaluation was done by gonioscopy except for one study reported by Ramashrikan et al16 who added AS-OCT evaluation. Laser efficacy was most often characterised by the gain of 1 Shaffer or Spaeth grade in two of four quadrants after the laser procedure. Ritch et al17 had successful procedures in 100% of eyes with at least Shaffer II angle opening after the laser procedure, and 13% of the eyes had progressive angle narrowing within 5–9 years, requiring a second deferred ALPI procedure that was successful in all cases. Romito et al10 observed no unsuccessful ALPI procedures but noted a recurrent iridocorneal apposition in five eyes requiring a new successful ALPI procedure performed 60.2±15.8 months after the initial treatment. Peterson et al4 had an 87% direct success rate and 13% of the eyes needed a direct second procedure to gain 1 Shaffer grade, and 18% needed a new procedure after gradual angle narrowing. Singh et al12 had the lowest success rate with 46% of patients with angle widening. Junqueira et al11 found a posterior trabecular meshwork visible on 180° without indentation on gonioscopic examination for 90% of eyes after the laser procedure. Ramakrishnan et al16 were the only authors to focus on PAS, reducing the median number of clock hours with PAS from 3.75 (2.00–6.50) to 2.50 (0.75–5.00) (p<0.001). AS-OCT evaluation also found an angle-opening distance at 500 µm from the scleral spur (AOD500) increased from 0.132±0.016 at baseline to 0.179±0.062 mm (p<0.001) after 1 year. Gomes Prado et al13 declared 91% non-occludable angle after the ALPI procedure with no further details provided. The changes in angle widening are presented in table 4.
Angle reopening and number of medications
Effect on the number of antiglaucoma medications
The number of medications was not systematically evaluated in the publications that evaluated ALPI efficacy. Ouazzani et al15 stopped medications in four of the nine eyes studied after 1 month. Gomes Prado et al13 kept the same treatment regimen during the follow-up in order to analyse the efficacy of ALPI without the bias of hypotensive medication changes. Ramakrishnan et al16 showed a significant reduction from 1.6±0.5 to 0.7±1 medications (p<0.001) after 1 year. Ritch et al17 showed no significant changes in antiglaucoma medications with no filtration surgery required after more than 6 years. Romito et al10 found no significant change in the number of medications (from 0.81±0.94 to 1.2±1.04; p>0.05) after 7.5 years and 10 eyes required a selective laser trabeculoplasty (SLT) procedure. Peterson et al4 was the only study showing a significant increase in the number of medications 2 years after ALPI and the need for filtering surgery or phacoemulsification in two-thirds of the eyes. The effects on the number of antiglaucoma medications are presented in table 4.
Discussion
PIS is a common cause of chronic angle-closure glaucoma, and ALPI is presented by some authors as a safe and non-invasive procedure for IOP control and angle opening. Our study is the first review evaluating the efficacy of ALPI in PIS since Ng et al18 published a Cochrane meta-analysis in 2012 demonstrating the lack of clinical outcomes on ALPI. At that time, only the Ritch et al17 retrospective cohort study published in 2004 was available. Seven years later, there is still no randomised control trial published on ALPI efficacy and safety on chronic angle-closure caused by PIS. Unfortunately, the recent cohort studies contribute little, non-standardised information with results often combining PIS and lens-induced angle closure,11 13 16 that in 2019 does not allow us to draw a firm conclusion on the role of ALPI in PIS.
The first ALPI procedures were proposed by Ritch9 in 1982 to treat medically unresponsive angle-closure attack. Their observations were based on angle-closure glaucoma without distinguishing the underlying mechanisms. The aim of ALPI was to contract iris peripheral stroma to decrease its contact with the trabecular meshwork. These iris changes following ALPI were confirmed histopathologically in 1993 in a case report. Sassani et al19 theorised that heat-induced shrinkage of collagen may be responsible for the short-term response to ALPI and that the healing characterised by the contraction of the fibroblastic membrane may promote long-term angle opening. Ritch et al20 then extended ALPI indications to PIS, explaining that an anteriorly positioned ciliary body pushing the iris root forward towards the trabecular meshwork could be flattened by lower power, longer duration and large laser spot sizes, causing deep contraction burns. Iridocorneal angle morphology change before and after ALPI was evaluated with AS-OCT by Lim et al on 60 eyes with persistent occludable angle after LPI regardless of the angle-closure mechanism. Using the Anterior Segment Analysis Program, a significant increase in iridocorneal angle parameters was found: angle opening distance (AOD500 and AOD750), trabecular iris surface area (TISA500 and TISA750), anterior chamber volume and anterior chamber area (ARA500 and ARA750). However, no significant changes were observed on central anterior chamber parameters: anterior chamber width, anterior chamber depth and lens vault, illustrating the action of ALPI on the peripheral iridocorneal angle morphology.
The spot sizes might explain the disappointing results found by Peterson et al4 and Singh et al,12 given that they used smaller spots and a shorter exposure time than Ritch et al17 and Romito et al.10 Nevertheless, these authors explained their laser protocols as preventing adverse events. Ramakrishnan et al16 were the only authors to show transient photophobia following an ALPI procedure, and no other adverse events were reported in the other published studies on PIS. Espana et al21 presented a series of 12 eyes in eight patients with persistent iris dilatation after an ALPI procedure for acute angle-closure. Only one patient had a decrease in visual acuity, but seven of the eight patients declared blurred vision. The pupillary response to pilocarpine instillation was minimal or absent and mydriasis eventually resolved in all eyes without treatment within 1 year. The reversibility of these complications should reassure the patients and the ophthalmologist on ALPI tolerance. Moreover, in the study reported by Espana, ALPI was performed for an acute angle-closure that could be by itself responsible for persistent iris dilation.
Despite non-significant long-term results, Peterson et al4 compared their results to the Ritch et al17 cohort. They noted a higher baseline IOP (mean IOP, 21.3 mm Hg) with fewer eyes on IOP-lowering medications (seven eyes, 33%, on one to two medications) in the Peterson’s cohort, compared with Ritch’s study (mean IOP, 18 mm Hg with 100% of eyes on IOP-lowering medication). In addition, seven eyes (33%) in Peterson’s study had peripheral anterior synechiae (PAS), and two eyes (9%) had glaucomatous damage before ALPI, whereas PAS were not documented, and no eyes had glaucomatous damage in the Ritch et al study. It is noteworthy that Peterson’s cohort had more advanced disease than the patients from the Ritch et al study.
Based on Ouazzani et al’s observations,15 iridoplasty seems to have a rapid effect on lowering IOP, which seems maintained after 1 year. To date, Gomes Prado et al13 is the only study excluding hypotensive medication bias with no change in treatment during the 11.8 months of follow-up. However, long-term IOP management seems more difficult. Ritch showed three eyes (13%) with gradual angle narrowing 5–9 years after initial ALPI, but the angle reopened after a second ALPI treatment. Romito et al10 declared five eyes (10%) requiring a new ALPI for gradual angle reclosure 60.2 months after the first procedure. The author attributed this angle closure to the gradual lens growth and every secondary procedure was successful. Six eyes (10%) also required phacoemulsification justified by significant loss of vision. Peterson et al’s management of angle narrowing was different with eight (36%) eyes requiring filtering surgery and nine (41%) eyes requiring phacoemulsification within 6 years of follow-up. All eyes had controlled IOP after cataract extraction, and five out of nine eyes were free of IOP-lowering medications 3 months after surgery. Cataract surgery attenuated anterior positioning of the ciliary processes in eyes with primary angle-closure, concomitant with significant opening of the angle.22 However, Viet Tran et al23 showed the persistence of iridociliary apposition after phacoemulsification in a series of six patients with PIS previously treated with LPI and ALPI. These studies show the low probability of IOP resolution after phacoemulsification as a standalone procedure in PIS.
The ciliary bodies’ anteposition is the initial cause of angle-closure physiopathology in PIS. However, the ALPI mechanism is only based on the thinning of the superficial iris tissue at the level of the crowded angle24 and has no impact on the ciliary body anteposition, which might explain the poor long-term outcomes. Hollander et al25 hypothesised that shrinking the ciliary processes with endoscopic cyclophotocoagulation (ECP) creates a space that will accommodate the thickened peripheral iris during pupillary dilation and prevent angle closure. In a series of nine eyes of six patients with PIS, they showed a significant IOP reduction from 25.2 mm Hg to 17.1 mm Hg (p<0.05) with a lowering in the number of medications after a 73-month follow-up. Moreover, the angles were opened in UBM only in areas treated with ECP with corresponding flattened ciliary processes. This invasive procedure could become an advantageous treatment for patients with PIS and a persistent occludable angle or uncontrolled IOP due to PIS.
Conclusion
ALPI does lower IOP in chronic angle-closure PIS over the short term and may widen the iridocorneal angle. These effects may be associated with a short-term reduction in the number of medications. Nevertheless, these observations are based on small retrospective cohort studies with a 1-year follow-up and there is no current evidence of long-term efficacy among the three long-term cohort studies available. Moreover, the effects of ALPI on visual field progression have never been studied. As a consequence, there is no strong scientific evidence as yet to advocate ALPI as a treatment of chronic angle-closure caused by PIS.
References
Footnotes
Contributors VA and HB were in charge of bibliography, data extraction and article redaction. AL and CB, providing their glaucoma expertise, were in charge of the article supervision and careful rereading.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.