Article Text

Abstract
Objective To determine the time to first clinically meaningful improvement in best-corrected visual acuity (BCVA) in patients treated with ranibizumab for diabetic macular oedema (DME) and identify predictors of early visual improvement.
Methods and analysis We retrospectively analysed the phase III RIDE (NCT00473382) and RISE (NCT00473330) trials, in which 759 patients with DME were randomised to monthly intravitreal ranibizumab 0.3 mg (n=250), ranibizumab 0.5 mg (n=252) or sham treatment (n=257). After month 24, 191 sham-treated patients crossed over to monthly ranibizumab 0.5 mg through month 36, while ranibizumab-treated patients continued treatment. Kaplan-Meier analyses assessed time to achieve ≥15 or ≥10 Early Treatment Diabetic Retinopathy Study (ETDRS) letter gains from baseline or ≥20/40 Snellen equivalent BCVA in each treatment arm. Baseline predictors of ≥15 ETDRS letter gains at month 6 were identified by logistic regression.
Results Median time to first ≥15 ETDRS letter gain was significantly shorter in patients who received ranibizumab (0.3 mg, 11.1 months; 0.5 mg, 10.9 months) than sham-treated patients who crossed over to ranibizumab 0.5 mg at month 24 (35.7 months; both p<0.0001). Half of ranibizumab-treated patients achieved ≥20/40 BCVA within 2.3 (0.3 mg) and 1.9 months (0.5 mg). Baseline predictors of early vision improvement among ranibizumab-treated patients were BCVA ≤55 ETDRS letters, younger age and presence of subretinal fluid.
Conclusion Prompt ranibizumab therapy for DME was associated with rapid, clinically meaningful vision gains that were maintained over 36 months of treatment. Lower BCVA, younger age and presence of subretinal fluid were predictive of early vision improvement.
- Diabetic macular oedema
- ranibizumab
- visual acuity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The phase III RIDE and RISE trials have previously demonstrated the safety and efficacy of intravitreal ranibizumab in patients with diabetic macular oedema (DME). To better understand functional responses to ranibizumab, this posthoc analysis quantified the time to achieve clinically meaningful visual improvements in RIDE/RISE and identified patient characteristics that were predictive of early vision gains.
What are the new findings?
On average, patients randomised to receive ranibizumab at RIDE/RISE baseline first achieved 20/40 or better vision after 3 monthly injections and gained ≥15 Early Treatment Diabetic Retinopathy Study (ETDRS) letters in best-corrected visual acuity (BCVA) within 1 year of treatment. In these patients, clinically meaningful visual improvements were maintained over 36 months of treatment and occurred earlier than in sham-treated patients who received delayed ranibizumab therapy after month 24. Patient factors associated with an early visual response to ranibizumab (defined as a BCVA gain of ≥15 ETDRS letters from baseline at month 6) included younger age, lower BCVA and the presence of subretinal fluid at baseline.
How might these results change the focus of research or clinical practice?
These data highlight the value of prompt versus delayed ranibizumab therapy for DME and may be used to manage patient expectations and inform treatment decisions in clinical practice.
Introduction
Diabetic retinopathy (DR) is a leading cause of blindness among working-age adults in the developed world and is estimated to affect 35% of individuals with diabetes aged 20–79 years.1 Diabetic macular oedema (DME), a vision-threatening complication of DR, develops in ~20%–30% of individuals with a ≥20-year duration of diabetes.1 2 Although the pathophysiology of DME is not fully understood, chronic hyperglycaemia is believed to cause retinal microvascular damage and increased expression of vascular endothelial growth factor (VEGF).3 Along with pathological angiogenesis, VEGF upregulation promotes increased vascular permeability, contributing to the breakdown of the blood-retina barrier and the vascular leakage underlying DME.3
Intravitreal ranibizumab, a monoclonal antibody fragment targeted against VEGF-A, has been shown to decrease macular oedema and improve vision in patients with DME4–7 and is approved for this indication in several regions, including Europe8 and the USA.9 In particular, evidence that informed the US Food and Drug Administration approval of ranibizumab for DME was primarily derived from RIDE and RISE, two methodologically identical, phase III, multicentre, double-masked, randomised controlled trials that evaluated the efficacy and safety of intravitreal ranibizumab in patients with vision loss due to DME.4 Compared with those who received sham injections, a significantly greater proportion of ranibizumab-treated patients in RIDE and RISE gained ≥15 Early Treatment Diabetic Retinopathy Study (ETDRS) letters in best-corrected visual acuity (BCVA) from baseline to 24 months;4 BCVA gains achieved during this period were maintained through month 36 with ongoing ranibizumab treatment.5
At month 24, sham patients in RIDE and RISE crossed over to receive monthly ranibizumab 0.5 mg, which allowed investigators to assess the effect of delayed treatment on visual outcomes.5 Vision gains observed in the sham crossover group between months 24 and 36 were lower than that achieved by the ranibizumab treatment arm from baseline to 12 months,5 suggesting that prompt intervention may be necessary to avoid the irreversible consequences of chronic DME and maximise patient responses to therapy.
Understanding patterns of response to ranibizumab and predictors of early visual improvement may inform physician and patient expectations of ranibizumab therapy in clinical practice. Using data obtained from RIDE and RISE, this retrospective analysis aimed to quantify the time to clinically meaningful vision gains in patients with DME treated with ranibizumab and to identify baseline patient and ocular characteristics that predict early responses to treatment.
Materials and methods
RIDE and RISE
Full details of the study design, patient population, methods and primary outcomes of RIDE and RISE are reported elsewhere.4 5 Briefly, RIDE (ClinicalTrials.gov identifier NCT00473382) and RISE (NCT00473330) included patients aged ≥18 years, with diabetes mellitus (type 1 or 2), vision loss due to DME (BCVA 20/40–20/320 Snellen equivalent) and macular oedema identified by time-domain optical coherence tomography. One eye per patient was randomised to receive monthly intravitreal injections of ranibizumab 0.3 mg, ranibizumab 0.5 mg or sham treatment; after month 24, sham patients were eligible to receive monthly treatment with ranibizumab 0.5 mg for the remainder of the 36-month treatment period. From month 3 onwards, all patients were eligible to receive macular laser therapy according to protocol-specified criteria; panretinal laser was available as clinically indicated.
The primary efficacy endpoint of RIDE and RISE was the proportion of patients who gained ≥15 ETDRS letters in BCVA from baseline at month 24.4 Secondary endpoints relevant to the present analysis included mean change from baseline BCVA over time and the proportion of patients who achieved BCVA of 20/40 or better (equivalent to 70 ETDRS letters). Both trials were conducted in accordance with the Declaration of Helsinki and were compliant with the Health Insurance Portability and Accountability Act. Protocols were approved by institutional review boards, ethics committees or as applicable, and all patients provided written informed consent.
Posthoc analyses
Data from RIDE and RISE were pooled in the present study, with analyses conducted on the intention-to-treat population by treatment arm. In the analyses of primary and secondary endpoints, missing BCVA values were imputed using last observation carried forward methodology. In the posthoc analyses described below, missing BCVA values were not imputed. Patient and public involvement was not sought for the design, conduct and reporting of this study.
Time to clinically meaningful visual improvement
Kaplan-Meier analyses were conducted to estimate the cumulative proportion of patients who achieved clinically meaningful visual improvements by month 36 and the time to first occurrence of such an event. Clinically meaningful visual improvements were defined as a gain of ≥15 or ≥10 ETDRS letters from baseline or the achievement of BCVA 20/40 or better. Time-to-event distributions for each of these definitions were compared between treatment arms using two-sided log-rank tests, with a threshold probability value of p≤0.05 selected a priori to indicate statistical significance. Patients who did not achieve a clinically meaningful visual improvement by month 36 were censored at the last available BCVA assessment.
Predictors of early visual improvement
Factors predictive of early visual improvement, defined as a BCVA gain of ≥15 ETDRS letters from baseline at month 6, were identified by multiple logistic regression modelling. Candidate covariates included baseline patient characteristics, demographics and targeted medical histories (table 1); significant variables were selected by the stepwise selection algorithm in models fitted separately for each treatment arm. A final model derived for the overall cohort included significant variables identified from each of the separate models, in addition to a treatment variable (ranibizumab-treated versus sham) and appropriate interaction terms. Odds ratios (ORs) and 95% CIs were estimated for each factor from the final logistic regression model.
Potential predictors of early visual improvement in RIDE and RISE
Results
As previously described,4 5 759 patients with DME were initially randomised to receive monthly sham injections (n=257), ranibizumab 0.3 mg (n=250) or ranibizumab 0.5 mg (n=252). After 24 months, 191 of 210 sham patients who remained in the study crossed over to active treatment and received monthly ranibizumab 0.5 mg through month 36 (sham/0.5 mg group). Patient demographics and study eye characteristics were well balanced across treatment arms at baseline.4 Over 36 months, a greater proportion of sham-treated patients received macular or panretinal laser therapy to the study eye compared with patients who received ranibizumab (table 2).
Treatments administered to study eyes through month 36 of RIDE and RISE, stratified by treatment arm (pooled data)
Patients with clinically meaningful visual improvement
The proportion of patients who gained ≥15 ETDRS letters in BCVA increased rapidly among those randomised to receive ranibizumab and was consistently greater than the sham-treated group over 36 months (figure 1A). At month 6, 27.2% and 23.8% of patients treated with ranibizumab 0.3 mg and 0.5 mg gained ≥15 ETDRS letters from baseline, respectively, compared with 8.6% of sham-treated patients. Following crossover at month 24, the proportion of sham/0.5 mg patients who gained ≥15 ETDRS letters from baseline increased modestly to 20.6% at month 36, but remained lower than the ranibizumab 0.3 mg and 0.5 mg treatment arms (44.0% and 40.9%, respectively; figure 1B).
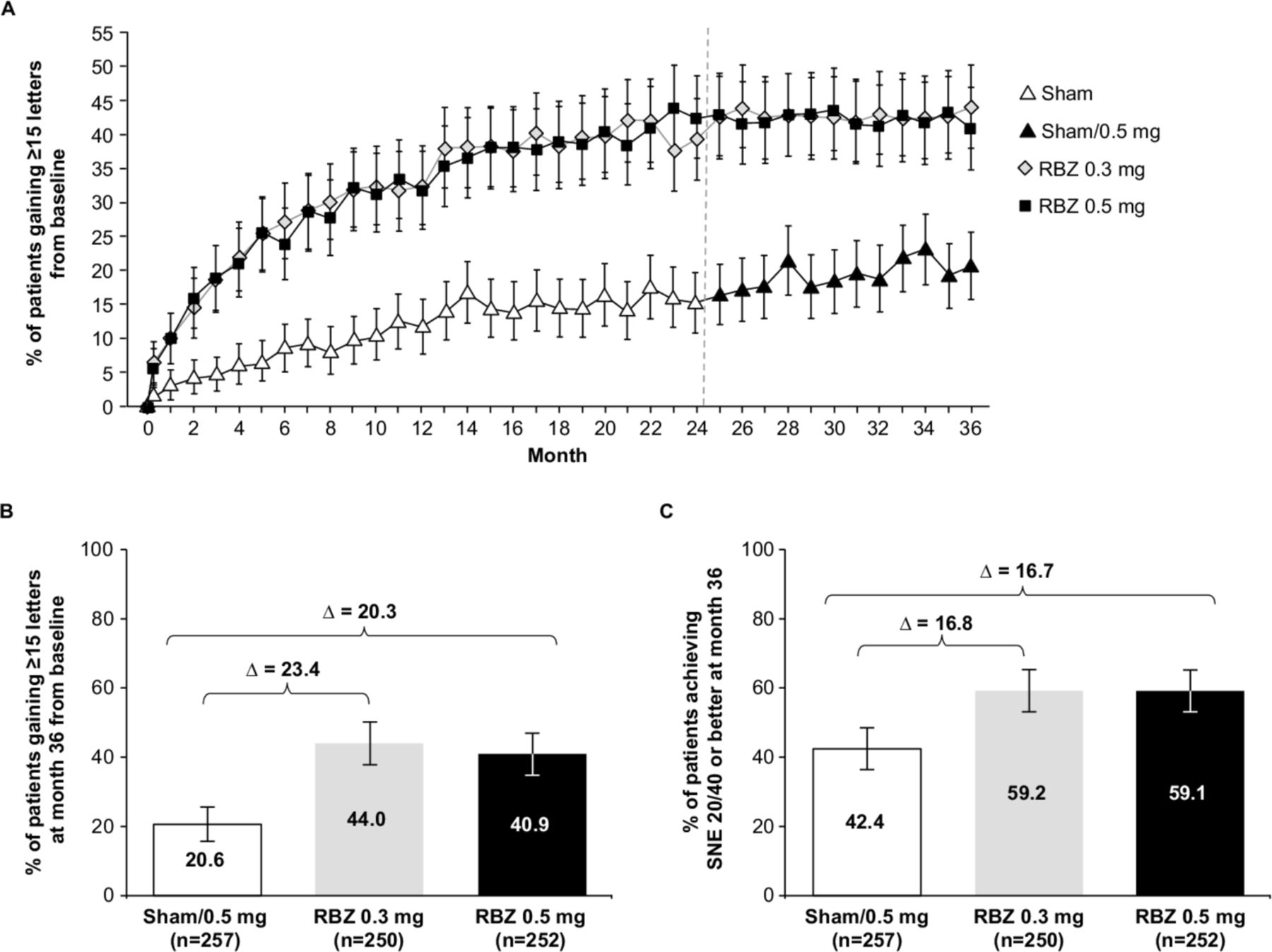
Proportion of RIDE/RISE patients with BCVA gains of ≥15 Early Treatment Diabetic Retinopathy Study letters from baseline (A) over time and (B) at month 36; (C) proportion of RIDE/RISE patients who achieved BCVA 20/40 or better SNE at month 36. Error bars represent 95% CIs; missing values were imputed by last observation carried forward. BCVA, best-corrected visual acuity; RBZ, ranibizumab; SNE, Snellen equivalent.
Similarly, a greater proportion of patients randomised to ranibizumab at RIDE/RISE baseline achieved BCVA 20/40 or better at month 36, compared with sham crossover patients (figure 1C). At baseline, 19.5% of sham/0.5 mg patients, 16.4% of ranibizumab 0.3 mg patients and 19.4% of ranibizumab 0.5 mg patients had 20/40 or better vision; these proportions increased to 42.4%, 59.2% and 59.1%, respectively, at month 36. Among those who achieved BCVA 20/40 or better at month 36 (n=406), 29.1% had this level of vision at baseline.
Time to clinically meaningful visual improvement
Clinically meaningful visual improvements were achieved earlier in ranibizumab-treated than sham-treated patients in RIDE and RISE, irrespective of the endpoint used to define such an event (figure 2). As shown in figure 2A, the median time to first gain of ≥15 ETDRS letters from baseline was significantly shorter in the ranibizumab 0.3 mg and 0.5 mg treatment arms (11.1 months and 10.9 months, respectively) compared with the sham/0.5 mg group (35.7 months; both p<0.0001) and was not estimable in sham patients who did not cross over to ranibizumab treatment (sham/no crossover group; n=66). The cumulative proportions of patients who ever gained ≥15 ETDRS letters by month 36 were 72% and 71% in patients treated with ranibizumab 0.3 mg and 0.5 mg, respectively, compared with 52% of sham/0.5 mg patients and 38% of sham/no crossover patients. In an exploratory time-to-event analysis of vision gains achieved after crossover at month 24, we found that the median time to first gain of ≥15 ETDRS letters from crossover was not estimable in the sham/0.5 mg group (data not shown). Cumulatively, less than 25% of sham/0.5 mg patients ever achieved a ≥15 ETDRS letter gain from crossover by month 36; in contrast, over 50% of patients randomised to ranibizumab at RIDE/RISE baseline ever gained ≥15 ETDRS letters within the first 12 months of treatment.
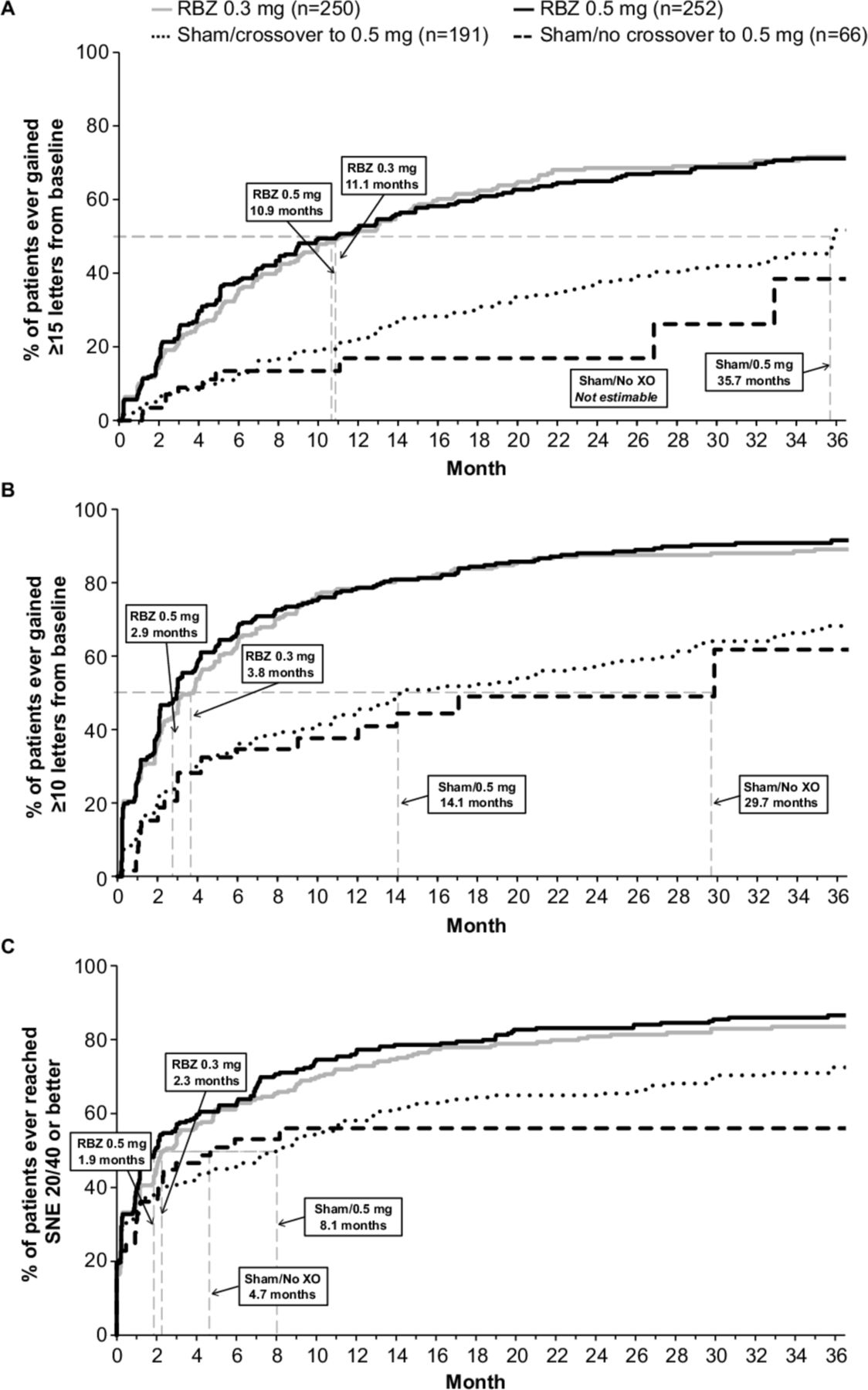
Kaplan-Meier plot of time to first BCVA gain of (A) ≥15 and (B) ≥10 Early Treatment Diabetic Retinopathy Study letters from baseline; (C) Kaplan-Meier plot of time to first achievement of BCVA 20/40 or better SNE. RIDE/RISE pooled data; missing values were not imputed. BCVA, best-corrected visual acuity; RBZ, ranibizumab; SNE, Snellen equivalent; XO, crossover.
Early responses to ranibizumab treatment were also observed when clinically meaningful visual improvements were defined as a gain of ≥10 ETDRS letters from baseline (figure 2B) or the achievement of BCVA 20/40 or better (figure 2C). The median time to first gain of ≥10 ETDRS letters from baseline was significantly earlier in patients treated with ranibizumab 0.3 mg and 0.5 mg than either the sham/0.5 mg or sham/no crossover groups (3.8 months and 2.9 months vs 14.1 months and 29.7 months, respectively; all p<0.0001). Similarly, the median time to first achievement of BCVA 20/40 or better was significantly shorter in the ranibizumab 0.3 mg and 0.5 mg treatment arms (2.3 months and 1.9 months, respectively) compared with sham/0.5 mg patients (8.1 months; p=0.002 and p<0.001, respectively) and sham/no crossover patients (4.7 months; p=0.036 and p=0.009, respectively).
Predictors of early visual improvement
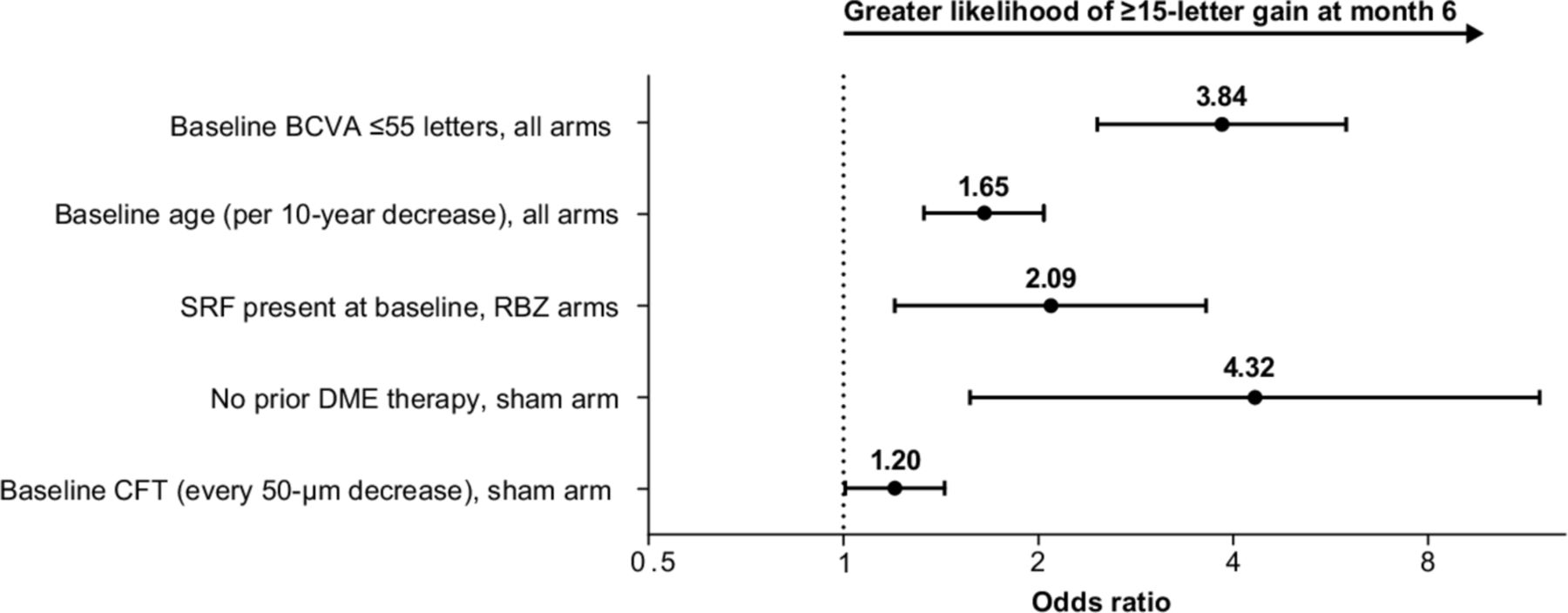
Factors predictive of early visual improvement, defined as a BCVA gain of ≥15 ETDRS letters from baseline at month 6, are presented in figure 3. Of the characteristics examined, baseline BCVA of ≤55 ETDRS letters (OR 3.84, 95% CI 2.47 to 5.98) and younger baseline age (OR per 10-year decrease 1.65, 95% CI 1.33 to 2.04) were associated with greater likelihood of early visual improvement across all patients, while the presence of subretinal fluid at baseline was predictive of early visual improvement in the ranibizumab treatment arms (OR 2.09, 95% CI 1.20 to 3.63). Among sham-treated patients, no prior DME therapy (OR 4.32, 95% CI 1.57 to 11.9) and lower central foveal thickness at baseline (OR per 50-µm decrease 1.20, 95% CI 1.01 to 1.43) were associated with greater likelihood of early visual improvement. In additional analyses, similar factors were identified as predictors of a BCVA gain of ≥10 ETDRS letters from baseline at month 6 (data not shown).

{kind=link}
{kind=link}
{kind=link}
Factors predictive of early visual improvement in RIDE/RISE, defined as a BCVA gain of ≥15 Early Treatment Diabetic Retinopathy Study letters from baseline at month 6. Error bars represent 95% CIs; missing values were not imputed in logistic regression analyses. BCVA, best-corrected visual acuity; CFT, central foveal thickness; DME, diabetic macular oedema; RBZ, ranibizumab; SRF, subretinal fluid.
Discussion
RIDE and RISE previously showed that ranibizumab therapy improved visual acuity and anatomic outcomes in patients with DME and that such benefits were maintained over 36 months of treatment.4 5 To further explore patient responses to ranibizumab, this retrospective analysis of RIDE and RISE compared the time to achieve clinically meaningful visual improvements between treatment arms and identified factors that predict early responses to therapy. Compared with sham controls, patients treated with ranibizumab benefited from significantly earlier vision gains, with >50% of patients achieving BCVA 20/40 or better within 3 months, gaining ≥10 ETDRS letters within 4 months and/or gaining ≥15 ETDRS letters within 12 months. Baseline patient characteristics associated with an early response to ranibizumab included lower BCVA, younger age and the presence of subretinal fluid. However, the cumulative proportion of ranibizumab-treated patients who ever achieved clinically meaningful visual improvements exceeded 70% by month 36, indicating that vision gains are nevertheless achievable with ongoing therapy.
In this study, the proportion of patients who achieved clinically meaningful visual improvements at month 36 was lower among sham-treated patients who switched to ranibizumab therapy after month 24 than those who received ranibizumab 0.3 mg and 0.5 mg from RIDE/RISE baseline. This finding is consistent with previous research5 and suggests that chronic oedema may impact a patient's capacity to gain vision with future treatment. Alternatively, photoreceptor damage caused by macular and/or panretinal laser therapy, which were received by more sham-treated patients in RIDE and RISE, may also limit visual responses to subsequent ranibizumab treatment. RIDE and RISE were not designed to compare laser therapy with ranibizumab; therefore, we were unable to determine whether suboptimal vision gains achieved by sham/0.5 mg patients were the result of laser therapy or delayed ranibizumab treatment. Nevertheless, patients with DME who initiated prompt ranibizumab therapy benefited from rapid vision improvements that were sustained over 36 months, which highlights the importance of early intervention to maximise treatment responses.
The results of our time-to-event analyses suggest that patients with DME may resume activities of daily living soon after initiating monthly ranibizumab therapy. For example, 20/40 vision in one or both eyes is the minimum requirement for a driving licence in many countries10 11 and is an acceptable threshold for daily tasks requiring an adequate level of visual acuity. In this study, the median time to BCVA 20/40 or better was ~2 months in RIDE/RISE patients who received prompt ranibizumab therapy, which was significantly earlier than in sham/0.5 mg and sham/no crossover patients. More than 80% of patients randomised to receive ranibizumab 0.3 mg or 0.5 mg in RIDE/RISE achieved 20/40 or better vision at any point over the study period, which was maintained by ~60% of patients at month 36.
Identifying factors that predict functional and anatomical responses to ranibizumab may inform and manage treatment expectations among clinicians and patients. Previously, factors associated with an early anatomical response to ranibizumab in RIDE/RISE (defined as an improvement of ≥2 steps on the ETDRS Diabetic Retinopathy Severity Scale12 from baseline at month 6) included baseline DR severity (particularly moderately severe to severe non-proliferative DR), no prior panretinal photocoagulation at baseline and the absence of DME at month 3.13 In the present study, baseline characteristics predictive of an early visual response to ranibizumab in RIDE/RISE were lower BCVA, younger age and the presence of subretinal fluid. While a lack of these characteristics may conversely reduce the likelihood of achieving early vision gains with ranibizumab, further studies are needed to identify other patient factors that predict a delayed or suboptimal response to treatment.
Our findings are consistent with other posthoc analyses that identified poor baseline BCVA, subretinal fluid at baseline and young age as predictors of ≥15 ETDRS letter gains from baseline at month 24.14 Lower BCVA and younger age at baseline were similarly associated with larger 1-year visual responses to ranibizumab in the Diabetic Retinopathy Clinical Research Network (DRCR.net) Protocol I study, in addition to less severe DR on clinical examination and the absence of surface wrinkling retinopathy.15 The presence of proliferative DR was not identified as a predictor of early vision gains in the present study, likely due to the exclusion of patients with active proliferative DR in RIDE and RISE.
It is unclear why younger age may be predictive of early vision gains with ranibizumab therapy; however, it has previously been hypothesised that the macula of younger patients may tolerate fluid accumulation without incurring loss of visual potential.14 Our observation that lower baseline BCVA was associated with early treatment response is suggestive of a ‘ceiling effect’; in other words, smaller improvements are required to achieve good vision in patients with higher BCVA at baseline, while those with poorer starting vision have greater capacity to achieve clinically meaningful visual gains over the course of treatment. Although further research is required to understand the association between subretinal fluid and early visual improvements, our findings may suggest that subretinal fluid is less disruptive to vision gains than intraretinal fluid or that eyes with subretinal fluid may be more responsive to ranibizumab treatment. Additional analyses of sham-treated patients showed that predictors of early treatment response included a lack of prior DME therapy and reduced central foveal thickness, characteristics consistent with less severe disease at baseline. Vision gains in the sham arm were likely driven by laser therapy, which has been associated with modest benefits in some patients with DME.16 17
Interestingly, neither baseline glycated haemoglobin (HbA1c) nor other systemic characteristics associated with diabetes were predictive of an early visual response to ranibizumab therapy. Similar findings have been reported in previous analyses of RIDE and RISE, which showed no association between systemic factors (including antihyperglycaemic medication history, serum glucose, renal function, body mass index, blood pressure and HbA1c) and functional or anatomic outcomes such as BCVA improvements and reductions in central foveal thickness.18 19 At the discretion of their evaluating physician, all patients in RIDE/RISE were permitted to continue standard treatments for diabetes; as a result, HbA1c and blood glucose at baseline and month 24 were similar between ranibizumab-treated and sham-treated patients, and no association was found between these parameters and BCVA gains achieved with ranibizumab therapy.19 Taken together, these data suggest that patient responses to ranibizumab are independent of non-ocular factors related to the systemic management of diabetes. However, because most RIDE/RISE patients had HbA1c ≤8% at baseline, patients with uncontrolled diabetes (HbA1c >12%) were excluded and follow-up was limited to 3 years,4 5 caution is required when generalising our analyses to alternative populations with elevated and/or uncontrolled HbA1c and extrapolating results over longer time horizons. It is well established that long-term glycaemic control is imperative to manage the risk of macrovascular and microvascular complications, including DR;20 therefore, further studies are required to characterise direct relationships between systemic control of diabetes and patient responses to ranibizumab.
In conclusion, this posthoc analysis of RIDE and RISE demonstrated the value of prompt versus delayed ranibizumab therapy for DME and identified predictors of early treatment responses in this patient population. The majority of patients randomised to receive ranibizumab at RIDE/RISE baseline achieved 20/40 or better vision after 3 monthly injections and gained ≥15 ETDRS letters from baseline within 1 year of treatment. Clinically meaningful visual improvements in these patients were maintained through month 36 and occurred earlier than in sham-treated patients who received delayed ranibizumab treatment at month 24. Baseline predictors of early vision gains among ranibizumab-treated patients included lower BCVA, younger age and the presence of subretinal fluid, information which may be used to manage patient expectations and inform treatment decisions in clinical practice. Data arising from this study provide an indication of how quickly patients with DME may regain vision and resume daily activities with monthly ranibizumab therapy and support the notion of early DME management in conjunction with systemic control of diabetes.
Acknowledgments
The authors thank the RIDE/RISE study group and investigators for their contributions to these trials; Jason S. Ehrlich, MD, PhD, of Genentech, Inc. for his contributions to RIDE/RISE and the initiation and concept stages of the present analysis; and Jeffrey R. Willis, MD, PhD, of Genentech, Inc. for his contributions to the manuscript.
References
Footnotes
Presented at Data reported herein were presented in part at the Association for Research in Vision and Ophthalmology 2013 Annual Meeting, May 2013, Seattle, Washington, USA.
Contributors LM and LT contributed to the design and conduct of the study and data collection. LM, LY and LT contributed to data analysis, interpretation and critical review and final approval of the manuscript. LM contributed to provision of materials, patients or resources. LY contributed to statistical expertise.
Funding Genentech, Inc., a member of the Roche Group, provided financial support for the study, participated in the design and conduct of the study and was involved in data collection, management and interpretation. Third-party writing assistance, provided by Karina D. Hamilton-Peel, PhD, Jack W. Pike, PhD and Kathryn H. Condon, PhD, of Envision Pharma Group, was funded by Genentech, Inc.
Competing interests LM serves as a consultant for Allergan, Genentech, Inc. and Iridex. LY and LT are employees of Genentech, Inc.
Patient and public involvement statement Patient and public involvement was not sought for the design, conduct and reporting of this study.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Qualified researchers may request access to individual patient level data through the clinical study data request platform (www.clinicalstudydatarequest.com). Further details on Roche's criteria for eligible studies are available here (https://clinicalstudydatarequest.com/Study-Sponsors/Study-Sponsors-Roche.aspx). For further details on Roche's Global Policy on the Sharing of Clinical Information and how to request access to related clinical study documents, see here (https://www.roche.com/research_and_development/who_we_are_how_we_work/clinical_trials/our_commitment_to_data_sharing.htm).