Article Text

Abstract
Objectives To investigate whether people with age-related macular degeneration (AMD) are able to self-detect symptoms and, if so, what symptoms they experience, from whom they first seek help, whether help is sought within the 1 week recommended by the Royal College of Ophthalmologists’ guidelines and reasons for any delay.
Methods and analysis A retrospective, cross-sectional survey design. Postal surveys were sent to 4000 members of the UK Macular Society. Inclusion criteria were participants aged >50 years at diagnosis of AMD with diagnosis after August 2008; criteria were met by 621 respondents. The main outcome was reasons for delays in diagnosis for wet AMD. Data were analysed using χ2 and conventional content analysis.
Results Only one third (n=199; 32%) of respondents were able to self-detect symptoms. In line with national guidance, over half (n=131; 64%) of those self-detecting symptoms sought help promptly. For those whose initial diagnosis was delayed more than 1 week, 27% had potentially treatable wet AMD requiring urgent treatment to prevent vision loss. Reasons for delay reflected individual & service-related issues, including AMD not being detected in the initial consultation, and individuals not perceiving the urgency for symptom investigation.
Conclusion In practice most patients sought help within 1 week; however, potentially sight-damaging delays occurred from symptom onset to diagnosis. Suggestions for reducing delay include increasing population awareness of AMD symptoms, the need for urgent detection and close monitoring for AMD and signposting patients to appropriate support services to ensure prompt detection of any future signs of wet AMD.
- degeneration
- macula
- retina
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Previous research has shown symptoms of age-related macular degeneration (AMD) can be difficult to self-detect. There are delays from symptom onset to diagnosis despite findings that early help seeking leads to better treatment outcomes (eg, visual acuity) in wet AMD.
This study shows that most patients seek help within 1 week but delays occur between symptom onset and diagnosis, which reflect individual & service-related issues.
This paper provides a unique insight into patient-reported reasons for delays including delays obtaining appointments, AMD not being detected in the initial consultation and patients not perceiving the urgency of prompt help-seeking for their symptoms.
Suggestions for reducing delay and shaping clinical practice are provided, including increasing patient and practitioner awareness of AMD symptoms, the urgency of detecting and close monitoring for AMD (particularly following treatment for other eye conditions) and educating patients alongside signposting to support services to ensure prompt detection of any future signs of wet AMD, following the diagnostic consultation.
Introduction
Age-related macular degeneration (AMD) is the leading cause of severe visual impairment in older adults.1 Late-stage AMD accounts for two thirds of registrations of visual impairment or blindness in the UK.1 The estimated UK prevalence for 2010 was 513 000 cases of late-stage AMD, which is expected to rise to 679 000 by 2020.2 There is some debate about whether AMD symptoms can be self-detected satisfactorily at an early stage. The guidelines of the Royal College of Ophthalmologists (RCOphth) (2013)1 suggested patients with symptoms of dry AMD may not be able to self-detect symptoms. Consequently these may only be detected by a professional on routine examination. However, when both eyes are affected, patients commonly report deterioration in central vision and difficulty with daily activities (eg. reading). Patients with wet or neovascular AMD may report blurred central vision, distorted vision (including straight lines appearing wavy (metamorphopsia)) or missing patches (scotomas) in their central vision. When both eyes are affected, patients are more likely to lose their ability to read, drive or see fine details including facial expressions. However, having good vision in one eye may mask difficulties in the other eye.3 There has been little research examining how patients identify and describe the symptoms that lead them to seek help.
There is mounting evidence that treatment outcomes for wet AMD, including visual acuity (VA), can be improved by early diagnosis and treatment4 . Patients with better pre-treatment VA have been shown to have better VA outcomes following anti-vascular endothelial growth factor (VEGF) treatment (ranibizumab or bevacizumab) for wet AMD, with the effects holding up to 1 year later.5 Furthermore, having symptoms of AMD less than a month before starting treatment has been associated with better post-treatment VA than having the symptoms for a longer duration before treatment.6 Hence there are significant benefits to early help seeking and detection of wet AMD. The benefit of early detection of dry AMD is less clear as there is currently no treatment available, other than the age-related eye disease study (AREDS) nutritional supplement formulation, which slows progression of dry AMD.7 However, as dry AMD can turn into wet AMD, educating patients on the use of Amsler grid to self-monitor for indications of further deterioration or possible conversion to wet AMD and encouraging lifestyle changes, such as smoking cessation, may help to reduce the risk of dry or wet AMD progression.3
In practice, patients who have advanced AMD in one eye are encouraged to seek help from an optometrist or hospital eye service as soon as possible, once symptoms in the second eye are noticed.1 In addition, healthcare professionals (HCPs) are encouraged to provide advice to, and follow-up, patients with earlier stages of AMD in a timely way. The RCOphth guidelines1 recommend that patients with suspected wet AMD are referred by optometrists to a fast track macular clinic within a week, and have treatment commenced in no more than one additional week. This is further reinforced in the 2018 National Institute for Health and Care Excellence (NICE) AMD guidelines, which recommended that treatment for wet AMD be commenced within 14 days of first presentation/diagnosis.8 Since 2009, optometrists have been advised to make direct referrals to the fast track macular clinics for suspected cases of wet AMD, rather than via the general practitioner (GP). Research suggests, however, that these guidelines have not always been followed in practice, with ongoing delays occurring from symptom detection to diagnosis.9 Among patients with wet AMD, the mean duration from symptom onset to assessment has been found to be around 2 months, with delays being longer for older patients aged over 75 years than younger patients.9 10 To the authors’ knowledge reasons for such delays have not previously been reported.
This study investigated the diagnostic experiences of a UK-wide sample of Macular Society members with AMD, including how their AMD (wet or dry) was first noticed, the symptom(s) that led them to seek help, the time taken and reasons for any delay. This study offers a unique insight into patient-reported symptoms and reasons for delay, with important implications for clinical practice.
Methods
Participants
A total of 4000 Macular Society members were selected from those who had joined the Society after 1 January 2000, using campaign management software (NFP CARE, Advanced Computer Software Group). In order to achieve an adequate sample size to investigate the impact of the RCOphth guidelines, stratified sampling was used, based on the date of joining the Macular Society (see figure 1). The reasons for this stratification are described elsewhere.11

Flowchart of respondents included in analysis. AMD, age-related macular degeneration. *The reasons for the stratified recruitment listed earlier are explained within the main text.
The main inclusion criteria were diagnosis with AMD after August 2008 (the date when NICE guidelines12 were published recommending early use of anti-VEGF injections for wet AMD and early help seeking and diagnosis became important) and age at diagnosis over 50 years (the diagnostic cut-off for AMD).12
Measures
The Macular Society survey 2013, used to collect the present data, asked respondents about several aspects of their experiences of living with a macular condition. Development work on the questionnaire and data from other parts of this survey are reported elsewhere.11 This paper focuses on the time around diagnosis. Several questions were designed to focus on:
How the respondent’s condition was first noticed, and if by themselves or someone else.
From whom they first sought help.
The symptom that led them to seek help (free-text response).
How quickly they sought advice from a HCP once symptoms were noticed.
If their appointment was delayed by more than 2 days, the reason(s) why (free text-response).
Sociodemographic information (sex, age, whether they lived alone) was collected, alongside whether they had heard of macular conditions before their diagnosis, self-rated health status, and eye-related information (diagnostic type, date of diagnosis).
Patient involvement
The Macular Society survey 2013 was adapted from a previous survey sent to members of the Society in 1999. The 1999 survey was pilot tested with people with AMD, to understand their experiences and priorities regarding the management of their condition. The Society funded and supported both surveys. Findings from both surveys have been reported to members in meetings of the Society and in their publications, SideView and Digest and elsewhere.13
Procedure
Informed consent was gained by receipt of a signed information/consent sheet attached to the survey.
The Macular Society survey 2013 was posted to 4000 members of the Society in November 2013. The survey was printed in large text and telephone-interview completion was offered to ensure that those who were severely sight impaired could participate. Twenty-six respondents requested telephone-interview completion: all were conducted by EB. No prompts were used in the telephone interviews so that this method of completion matched paper completion as much as possible; however, clarification about the meaning of questions was provided if needed. No follow-up reminders were sent to respondents in order to preserve confidentiality and avoid possible confusion for those who had already completed the survey.
Data analysis
Conventional content analysis14 was conducted to convert the free-text comments for symptoms and reasons for delay into numerical data. Data were analysed in IBM SPSS V.20. For the reasons-for-delay responses a coding framework was developed by AP and EB. These responses were coded by both researchers (75%), with the remaining responses coded by AP. For the symptom responses a coding framework was developed by AP and WMA. All responses were then coded by both researchers. Any discrepancies were discussed and resolved. Where multiple reasons/symptoms were given, multiple codes were allocated. These codes were then sorted into broader subthemes and themes and reviewed before being named and defined. Quotes, illustrating each theme, are provided in the results.
χ2 analyses were conducted to examine whether differences between respondents in reported time taken to seek help were associated with age, sex, health status, whether they lived alone and previous awareness of AMD. For these analyses, time to seek help was re-categorised into 0–6 days or ≥1 week as the RCOphth guidelines1 recommend patients seek help within 1 week. Age was re-categorised into 2 groups of 50–75 years and ≥76 years, as previous research suggested there are longer delays for those >75 years; overall health status was re-categorised into three groups: (i) excellent to good, (ii) neither good nor bad, and (iii) bad to extremely bad.
Missing data
There were varying amounts of missing data among the outcome variables, the greatest being for reason for delay in the appointment with a HCP about symptoms (missing n=43, 30.7%). There were no suitable variables to allow imputation of these missing values. Sample size for each analysis will vary slightly depending on item non-response and the missing n for each variable is provided within the results and table 1.
Respondent characteristics (n=621)
Results
Sample characteristics
Responses were received from 1571 members (response rate=39%) of whom 621 matched the sub-study inclusion criteria. For full respondent characteristics see table 1. The most common reason given for non-completion was old age, followed by ill health of members.
Detection of symptoms and seeking help
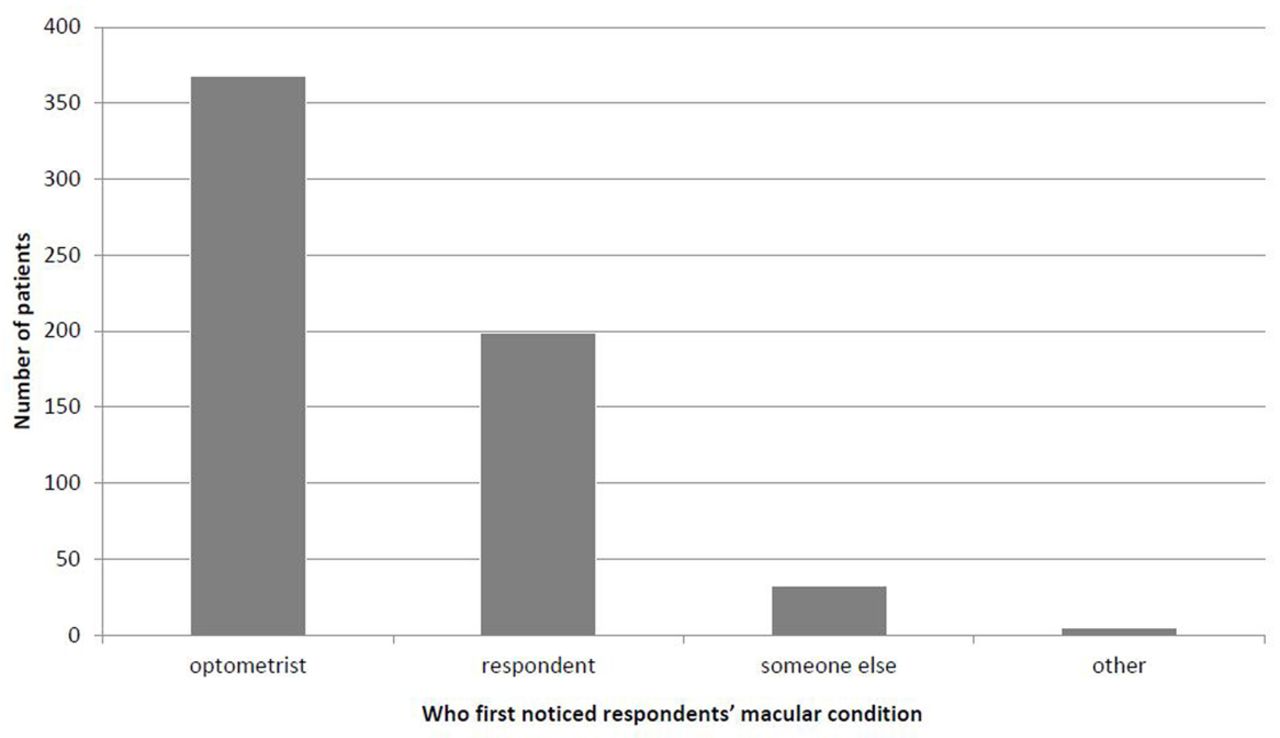
Of 621 respondents, 612 answered how their macular condition was first noticed: 368 by their optometrist, 199 themselves and 32 by someone else, while five ticked ‘other’ and eight ticked two options (see figure 2). ‘Someone else’ and ‘other’ responses included the hospital eye specialist during consultation for another eye condition and the GP.

Who first noticed respondent’s macular condition?. *‘Someone else’ responses included the hospital eye specialist during consultation for another eye condition (n=34) and the GP (n=1); two respondents giving ‘other’ responses left the free-text response blank.
For respondents who reported that the symptoms (or signs) were first noticed by themselves, by ‘someone else’ or ‘other’ (n=236), 230 indicated where they first sought help (127 optometrist, 51 hospital eye clinic, 35 GP, 6 other and 11 ticked two options).
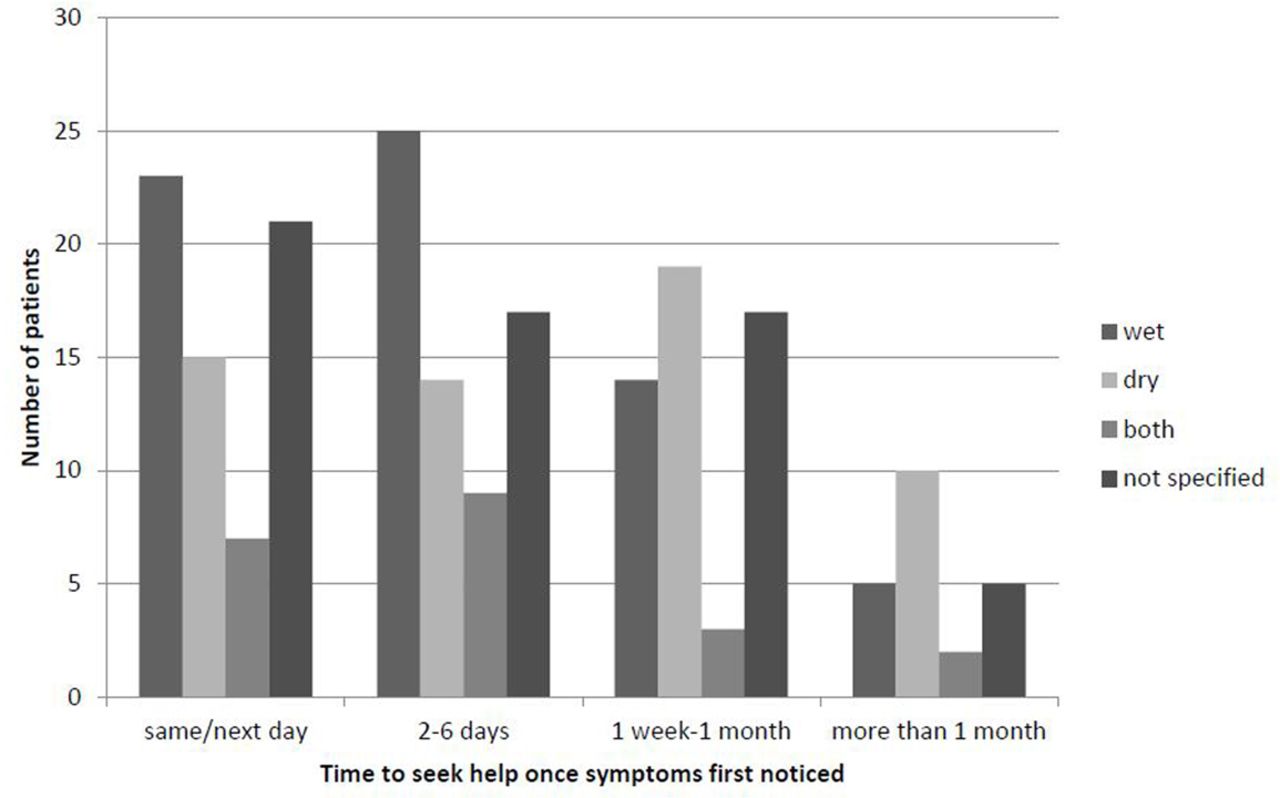
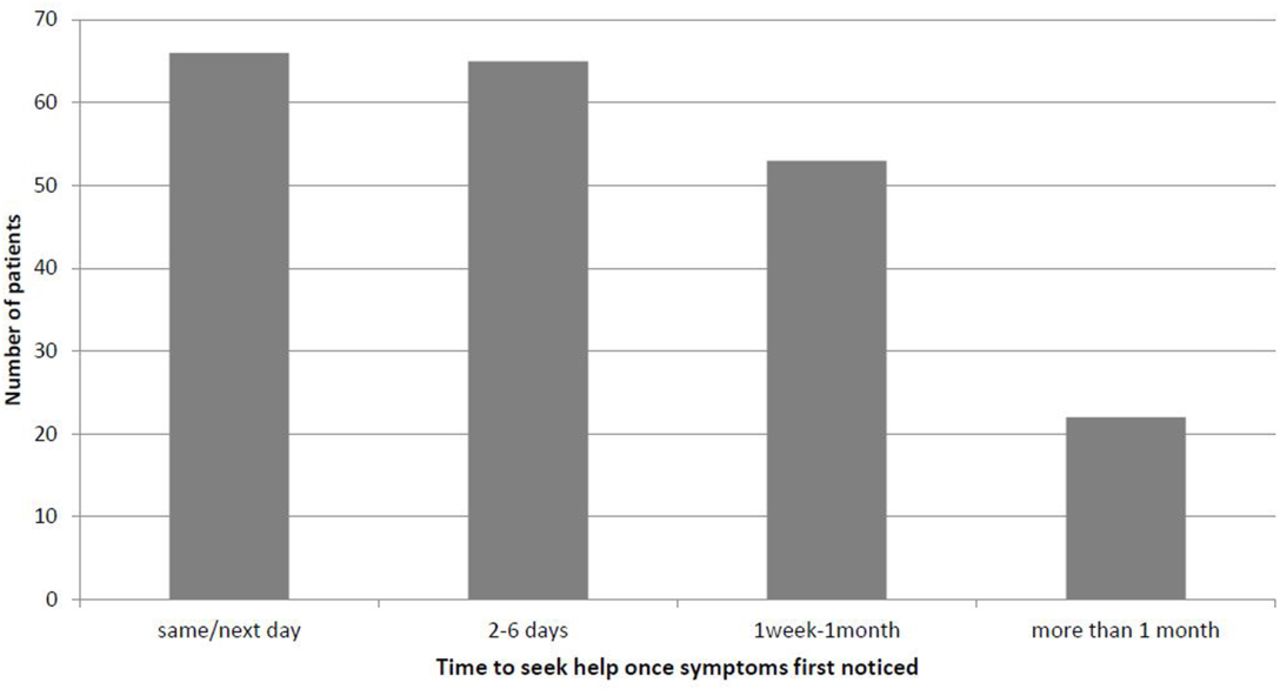
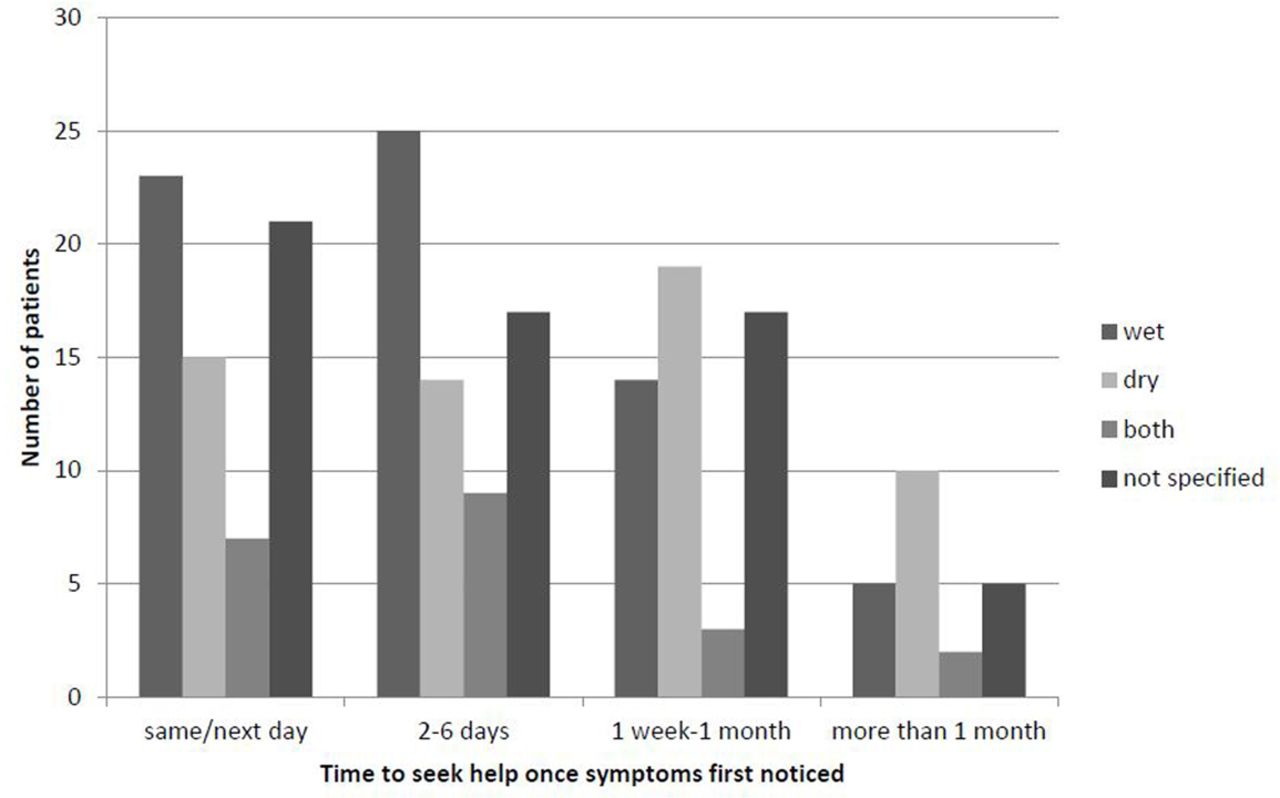
A total of 206 reported the time it took for them to seek help (including 66 same or next day, 65 2–6 days, 53 1 week–1 month, 22 more than 1 month) (see figure 3). Those experiencing a delay of more than 1 week included 19 (of 67) respondents with wet AMD, and 5 (of 21) with both wet and dry AMD (see figure 4).

Time to seek help once symptoms first noticed.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time to seek help once symptoms first noticed; sorted by age-related macular degeneration type at diagnosis.
There was a significant association between time taken to seek help and sex (χ2 (1, n=206)=3.848, p=0.050) with women being almost twice as likely as men to seek help within 0–6 days (OR=1.84). There was also a significant association between time to seek help and the type of AMD at diagnosis (χ2 (1, n=182)=8.78, p=0.003), with respondents having wet AMD being twice as likely as those with dry AMD to seek help in 0–6 days (OR=2.72). There was no significant association between time to seek help and respondents’ age, previous awareness of AMD, general health status or living alone.
Symptoms
Symptom(s) leading to help-seeking were reported by 217 respondents: for a full list, and respondent quotes see table 2.
Symptoms that led to help seeking. Listed in rank order (n=217)
The most common symptom cited as a reason for help seeking for patients with either type of AMD was visual distortion (n=87) (eg. straight lines becoming distorted). The second most cited symptom was deterioration in vision (n=83) (eg. blurred vision, loss of VA or difficulty focusing), which some attributed to difficulty with their current spectacles. Patients with either type of AMD reported help seeking action because AMD symptoms led to difficulty carrying out activities (n=34) or because they experienced central-field defects (scotomas) (n=34). Central-field defects (including black spots, blind spots or loss of central vision) were primarily reported by respondents with wet AMD.
Nineteen respondents listed symptoms that were not indicative of AMD, including eye discomfort/pain, double vision, shadows in vision, flashing lights or a transient loss of vision. In addition patients with wet AMD reported misattributing symptoms of AMD to another eye condition (n=13), namely cataracts, glaucoma or an eye infection, more often than patients with dry AMD. Two other symptoms listed by patients in both groups were difficulty with dark adaption (n=11) and problems with far vision/judging depth (n=6). Finally, additional symptoms included loss of chromatic sensitivity with certain colours disappearing (n=6) or witnessing no improvement following treatment for another eye condition (n=3). Fear of blindness was reported by two respondents (n=2) who had dry AMD.
Reasons for delay
Reasons for delay in having the appointment about symptoms were reported by 97 respondents: for a full list and supporting quotes see table 3. Patients reported delay from symptom onset to formal diagnosis and referred to delays in getting an initial appointment with various professionals, including the hospital eye specialist, GP and optometrist, as well as delays in subsequent appointments at the macular clinic.
Reasons for delay to diagnosis. Listed in rank order (n=97)
Service/healthcare professional-related factors
The most commonly cited reasons for delay in their first ophthalmologist assessment among respondents with either type of AMD related to inability to get an earlier appointment ((n=39): with the hospital (n=28), GP (n=2) or optometrist (n=9)), or AMD not being detected or labelled as such in the initial consultation ((n=30): by the hospital eye specialist (n=6), by the GP (n=7) and by the optometrist (n=17)). Delay in obtaining an appointment was more commonly reported by those with wet AMD. Respondents who reported that AMD was not detected/labelled at the consultation (similarly split between those with wet/dry AMD) often reported leaving the consultation unclear as to whether they had AMD, resulting in further delay to receiving a diagnosis. For some the diagnosis was missed ((n=20): by the hospital eye specialist (n=2), by the GP (n=4) and by the optometrist (n=14)) or only detected following cataract removal (n=8). Another commonly cited reason for delay, particularly among those with wet AMD, was delayed referral due to being passed between HCPs (n=4) or referred to the hospital via the GP (n=13) despite guidance15 that optometrists should refer directly to hospital.
Other patients, including two with wet AMD, were told that ‘nothing could be done’, were refused a further appointment, or asked to make their own follow-up appointments at a later date resulting in a delayed diagnosis ((n=8): by the hospital eye specialist (n=4), by the GP (n=1) and by the optometrist (n=3)). Several respondents including four with wet AMD, reported that they felt their HCP did not realise or stress the urgency of help seeking for AMD symptoms ((n=7): by the hospital eye specialist (n=3), GP (n=2) and the optometrist (n=2)). This led to delayed communication with other HCPs or the respondent feeling there was no urgency in following up their symptoms. Some respondents with wet AMD (n=6) cited delays in getting an appointment due to issues with correspondence (eg. appointment letters being lost or arriving after the offered appointment). Finally several respondents reported that they assumed waiting over 1 week for an appointment was normal NHS procedure (n=4).
Patient-related factors
The most common patient-related factor cited, primarily by patients with wet AMD, was that they did not attribute their symptoms to AMD as they either lacked knowledge about AMD symptoms and their risk for developing the condition, or attributed their symptoms to another eye problem (eg. needing stronger spectacles) (n=20). In addition several respondents, most commonly those with wet AMD, did not perceive their symptoms as urgent or important (n=13): such patients waited until their next routine appointment or until symptoms worsened before seeking help. Some respondents, predominantly those with wet AMD, reported inability to make an early appointment because they were too busy, on holiday, or had other health conditions or their family’s health taking precedence (n=11). One respondent with dry AMD reported not seeking help initially because of the shock about symptoms. These factors are summarised in table 3.
Discussion
This study found that only a third of patients were able to self-detect AMD signs/symptoms while the majority were detected by an optometrist. This finding supported the RCOphth guidelines, which suggested that AMD symptoms are often subtle and difficult to self-detect.1 Common symptoms experienced particularly among those with wet AMD were distorted vision, deterioration/loss of vision including blurred vision and central field defects/scotomas, in line with previous findings.16 Interestingly, however, we noted overlap in symptoms reported by those with wet and dry AMD and that it was often only when symptoms interfered with patients’ activities that they sought help. Most respondents who self-detected symptoms first sought help from their optometrist (56%). The majority of respondents (64%) sought help within the recommended time frame of 1 week.1 Women and those diagnosed with wet AMD were more likely to seek help within the recommended time frame. However, there was a delay in diagnosis for 36% of patients, including 27% with wet AMD with consequent risk of sight loss. For those reporting their first appointment with an HCP was delayed for more than 2 days after first noticing symptoms, reasons for delay reflected individual/service-related issues, most commonly difficulties obtaining appointments, AMD not being detected in the initial consultation and, particularly for those with wet AMD, respondents not attributing their symptoms to AMD.
This is the first large-scale nationwide study to examine the help seeking behaviours of patients with wet and/or dry AMD, including questions about how AMD was first detected, initial symptoms, the time taken to seek help and reasons for any delay. Furthermore this study is one of the first to obtain qualitative data on the symptoms and reasons for delay patients report. The response rate of 39% was low, but not dissimilar to other recent surveys including a Macular Society survey in 2014 (response rate=31%).17Analysis was conducted with single variables; therefore, there is the possibility of confounding by variables which may have been related to each other or unmeasured such as VA, which, although beyond the scope of this paper, are important to acknowledge, and may benefit from future research. The sample was self-selecting and may, therefore, have included those whose experiences differed from the wider population of people with AMD. As reported elsewhere, 76% of the total sample responding to the 2013 Macular Society survey were satisfied with the diagnostic consultation.11 It may be that those who were dissatisfied with the diagnostic consultation experienced more delays in diagnosis and/or treatment and were less likely to complete the survey. In addition Macular Society members may be a more proactive group than the population as a whole and perhaps likely to seek help and obtain support earlier. These possible sources of bias may influence the external validity of the findings. Nevertheless, there was still delay in help-seeking for initial symptoms, which several respondents attributed to a lack of knowledge of AMD prior to diagnosis. Therefore, the results are likely to generalise to a wider population and, if anything, may underestimate the true scale of the problem.
Our finding that those with wet AMD were twice as likely as those with dry AMD to seek help within 1 week provides a more positive picture than previous studies. Earlier research by Varano and colleagues reported that for those with wet AMD, only 23% sought help within 1 week of first noticing a change in vision.18 This compares with 72% of respondents with wet AMD in the present study. However, Varano et al’s18 study was conducted across nine countries, where time to seek help may differ between countries due to variation in access to, and provision of, eye-care services, particularly as this study indicated delays in obtaining an appointment was a primary reason for delay. In addition, Sim et al10 suggested that a lack of awareness of AMD could account for substantial delays. It may be that the smaller percentage of respondents delaying help seeking in this study is attributable to greater awareness of AMD. Although respondents in this study were recruited from the Macular Society, 57% reported no prior awareness of AMD (table 1), and further quantitative analyses indicated no significant link between prior awareness of AMD and time to seek help. We noted, however, that qualitatively several respondents reported lack of awareness of AMD symptoms and risk factors as a reason for delayed help seeking (table 3).
Sim et al’s10 additional finding that only 37.3% of patients could describe AMD symptoms correctly was also echoed in this study as several patients listed symptoms not indicative of AMD, reported a lack of knowledge about AMD symptoms/risk factors or misattributed symptoms of AMD to other eye conditions (eg. cataract or glaucoma). This highlights the need for public and patient education about symptoms of AMD and how to distinguish these from symptoms of other eye conditions, particularly in an elderly population, likely to have more than one eye condition.
The most commonly cited reason for delay, primarily by those with wet AMD, of difficulty obtaining an earlier hospital, optometrist or GP appointment, is consistent with previous research that among people with eye conditions, including AMD (23%), a large proportion (72%) experienced permanent reduction in VA due to service-related delays.19 Of these service-related delays, 76% were due to delayed follow-up appointments for monitoring, a problem reported primarily by patients with wet AMD in this study. Shared care between community optometrists and hospital ophthalmologists has been suggested as a possible solution to such delays, with optometrists monitoring more stable cases of wet AMD and freeing up ophthalmologists to diagnose and treat new cases of wet AMD more promptly.20 Several patients in the current study, particularly with wet AMD, reported that they were passed between HCPs or referred from their optometrist to the hospital via their GP. This is despite RCOphth guidance since 200915 that optometrists should refer straight to the hospital and suggests that this message needs to be highlighted again to reduce delay, particularly as referral via the GP has been found to extend delay by an average of 7.5 days.10 The RCOphth guidelines further suggest that patients should be given a clear diagnosis and suggestions for treatment, including signposting to support services where medical treatment is not possible. However, in this study, 31% of patients reported that a diagnosis of AMD was not labelled in the initial consultation (by a hospital eye specialist in 20% of cases, 23% by a GP and 57% by an optometrist), and 8% reported that they were told ‘nothing can be done’, with 42% of these patients having wet AMD. This is in line with previous research, which suggested only 43% of patients were diagnosed during their first visit.18 Delay in diagnosis has already been shown to be associated with likelihood of registration as sight impaired or severely sight impaired and to cause delay in accessing support services.11 Clearly interventions are needed to improve the skills of practitioners in detecting and managing AMD symptoms and awareness of the urgency for treatment of wet AMD. For several patients AMD was only detected following cataract removal. Although there is consensus that cataract surgery does not cause AMD progression, the presence of co-existing cataract may mask AMD detection.21 22 The current study, therefore, highlights the importance of evaluating patients for AMD symptoms before and following cataract surgery.
Patient-related reasons for delayed assessment included patients, commonly with wet AMD, not attributing their symptoms to AMD due to lack of knowledge about the symptoms and risks for the condition, or that they did not perceive their symptoms to be urgent or serious, and therefore waited for their next ‘routine’ appointment. This highlights the need for a public health campaign educating the general population about the symptoms and risk factors for developing AMD and the importance of prompt help seeking with an urgent self-referral to eye emergency care services if symptoms are noticed.
In summary, although most patients sought help within 1 week, there was a delay from symptom onset to assessment for 27% and 50% of patients with wet and dry AMD, respectively. These are in addition to the number of patients whose care was delayed following their initial presentation to a HCP who did not refer appropriately to the Macular Clinic. For those with wet AMD this delay has been linked with poorer treatment outcomes, while with dry AMD the diagnostic consultation is a key time for providing education about how to monitor their symptoms for possible change to wet AMD, aiding prompt future help-seeking and reducing likelihood of being registered as sight impaired.11 A number of suggestions have been provided above for reducing delay, primarily in reference to:
Interventions for example, TV/poster campaigns to increase general population and practitioner awareness of AMD symptoms including how to detect AMD and the importance of early help seeking (without first visiting the GP).
Education for newly diagnosed patients in Amsler grid use and ongoing monitoring for wet AMD by patient and practitioner, particularly following treatment for other eye conditions.
Signposting patients with dry/wet AMD to appropriate support services following the initial consultation. For example, charities can provide additional information to reinforce HCP advice about ongoing monitoring for potential signs of wet AMD and visual rehabilitation/counselling services to support adjustment to acquired visual difficulties; such support services could also help patients with dry AMD understand why they have not been referred for medical treatment. Signposting to support services is recommended in the NICE guidelines for those with wet AMD currently12 but our findings suggest this is also beneficial for those with dry AMD.
Informative interventions targeting the general population will need pilot work to ensure optimal design but have the potential for saving the eyesight of a substantial proportion of people with wet AMD currently not receiving sufficiently prompt diagnosis and treatment, and even more people who will go on to develop treatable wet AMD.
Supplemental material
References
Footnotes
Contributors CB prepared the research proposal in response to a request from the Macular Society for a follow-up survey. CB was responsible for supervision of the 2013 survey and the previous 1999 survey and associated studies. CB and EB designed the 2013 survey with valuable input from WMA. EB managed data preparation of the 2013 survey data with assistance from AP. EB and AP planned the present statistical analysis, carried out by AP. Qualitative data were coded by AP, EB and WMA and any discrepancies were discussed and resolved. AP drafted the manuscript, which was revised and approved by all authors. EB is the guarantor.
Funding EB was supported by a PhD studentship funded by the Macular Society to CB via Royal Holloway, University of London. The Macular Society reviewed and commented on the 2013 survey resulting in the addition of one item to be reported elsewhere. The Macular Society was responsible for printing and posting the surveys. AP was funded by Health Psychology Research Ltd, a spin-out company that licenses CB’s questionnaires and drives their linguistic validation into other languages.
Patient consent for publication Not required.
Ethics approval Ethical approval was obtained from the ethics committee of Royal Holloway, University of London (Ref: 05-13).
Provenance and peer review Not commissioned; externally peer reviewed.
Author note The proposal for this survey, a follow-up to an earlier survey funded by the Macular Society, was commissioned by the Macular Society.