Article Text

Abstract
Objective To investigate the role of bandage contact lenses (BCL) and topical steroids as risk factors for the development of microbial keratitis after epithelium-off corneal collagen cross-linking (CXL).
Methods and Analysis Patients undergoing CXL between February 2011 and July 2017 were included. Patients were divided into two groups: those who were treated postoperatively with a BCL, topical antimicrobial and steroids (group 1) and those who received only a topical antimicrobial until healing of the epithelial defect before introduction of topical steroids (group 2).
Results 1273 eyes of 964 patients were included. Group 1 comprised 316 eyes and group 2 comprised 957 eyes. There were no significant differences in the presence of persisting corneal haze or scarring between the two groups (p=0.57). Microbial keratitis occurred in nine eyes (0.71% of eyes) of eight (0.83%) patients (one case was bilateral) out of 1273 eyes. Staphylococcus aureus was cultured from corneal scrapes in seven out of nine (77.8%) cases and from contiguous sites in the two cases. All cases occurred in group 1 (incidence=2.85%) and none in group 2 (p<0.0001). A greater proportion of patients who developed microbial keratitis were atopic (75%, p=0.4).
Conclusion The use of BCL and topical steroids prior to healing of the epithelium is a significant risk factor for microbial keratitis. S. aureus is the most common micro-organism and is likely to originate from an endogenous site. Not using a BCL and delaying the introduction of topical steroids until epithelial healing significantly reduce the risk of developing microbial keratitis without increasing the risk of persistent corneal haze.
- microbial keratitis
- bandage contact lens
- topical steroids
- corneal collagen cross linking
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Epithelial removal in epithelium-off corneal collagen cross-linking (CXL) may predispose to microbial keratitis.
Although the use of bandage contact lens and topical steroids is useful in the postoperative care, reducing pain and inflammation, there is currently insufficient evidence to which extent they may predispose to the incidence of microbial keratitis.
What are the new findings?
The results of our study, which is the largest to date series on microbial keratitis following epithelium-off CXL, demonstrate that postoperative treatment protocol plays a substantial role in preventing this possibly sight-threatening complication.
How might these results change the focus of research or clinical practice?
The use of bandage contact lens and topical steroids in the early postoperative period may increase the risk of developing microbial keratitis and should be avoided in terms of safety.
Introduction
Introduced by Wollensak et al in 2003, corneal collagen cross-linking (CXL) has become accepted as a useful technique to reduce the risk of progression of keratoconus and other types of corneal ectasia.1 2 Previous reports have demonstrated the efficacy of CXL to stabilise disease progression, to prevent deterioration of vision and to reduce the need for corneal transplantation.3–6
Although there are several reports of performing CXL with an intact epithelium (transepithelial or epithelium-on), CXL with epithelial removal (epithelium-off) is still considered to be the gold standard of treatment.1 2 6 7 Removal of the epithelium, however, is associated with a significant risk of epithelial healing problems and may increase the risk of corneal infections, as one of the main physical barriers to microbes and other pathogens is removed.8 9 Indeed, the development of microbial keratitis (MK) is one of the most serious complications following CXL.10 11
Several risk factors for the development of microbial keratitis following CXL have been proposed.8–11 These include the presence of an epithelial defect, use of a bandage contact lens (BCL), conditions that may prolong the epithelium healing process such as atopic conjunctivitis, diabetes mellitus or the use of anaesthetic eye-drops, and postoperative steroid use.8–11 There is also the potential temporary loss of immune cells in the cornea following treatment. In this study, we investigated the incidence of microbial keratitis in patients undergoing epithelium-off CXL for keratoconus with and without postoperative BCL and steroids, and associated micro-organisms.
Patients and methods
All patients who had undergone CXL for keratoconus from February 2011 to July 2017 at The Royal Liverpool University Hospital, UK were included. The main criterion for patients being offered CXL was an evident progression of keratoconus demonstrated by a change in the curvature within the cone area of at least 1 dioptre (D) on instantaneous map when measured at least 3 months apart. Exclusion criteria for CXL were minimal corneal pachymetry of less than 380 µm, recent history of corneal infection, concomitant ocular or systemic autoimmune disease, and pregnancy or breast feeding. A corneal infiltrate with an overlying epithelial defect, ocular discharge, anterior chamber inflammatory reaction, conjunctival injection and subjective symptoms were considered as clinically suspected microbial keratitis.
We previously described the CXL protocol used in our centre. Briefly, it involves removal of corneal epithelium with 20% alcohol followed by 15 min of 0.1% riboflavin (VibeX Rapid).12 Corneas were irradiated with Ultraviolet A 365 nm light using Avedro’s KXL (Avedro, Massachusetts, USA) machine at an irradiance of 6 mW/cm2 for 15 min, delivering a total of 5.4 J/cm2. The CXL procedures were performed in an aseptic room specially designed and used for CXL following strict hygiene and sterilisation rules. All instruments and materials used during each procedure were sterile, and povidone iodine was applied prior to CXL both to the conjunctival fornices (5%) as well as to the surrounding skin (10%).
Patients were divided into two groups according to the postoperative treatment that they received. Group 1 included cases in which postoperative management consisted of chloramphenicol 0.5% eye-drops every 2 hours for the first 2 days and then four times a day for 1 week, the use of a BCL (SB18, Menicon) and dexamethasone 0.1% eye-drops four times a day for 1 month starting from day 1. Patients were reviewed on days 2 and 7 and the BCL was removed subject to satisfactory epithelial healing. In group 2, patients received chloramphenicol 1% preservative-free ointment 2 hourly for the first 2 days and then four times a day for 1 week, followed by 0.1% dexamethasone eye-drops four times daily for 1 month. All patients were reviewed 2 and 7 days after CXL.
In patients who developed a clinically suspected microbial keratitis following CXL, corneal scrapes were collected for smear and culture. Swabs were also taken from the conjunctival fornices, anterior nares and pharyngeal arches for possible endogenous sources of infection. Patients were commenced on 1% teicoplanin eye-drops and 0.3% ciprofloxacin ointment hourly for 24 hours and then hourly only during waking hours according to the clinical response and microbiological results. Possible risk factors were recorded in every case and data were enrolled in a multivariate analysis. Confocal microscopy was performed in all cases.
Statistical analysis was performed with MedCalc Statistical Software V.14.8.1 (MedCalc Software bvba, Ostend, Belgium) and SPSS V.19.0 for Windows. Data are given as mean±SD. Normality was checked using the Kolmogorov-Smirnov test. When parametric analysis was possible, the Student’s t-test was used to compare the outcomes between two independent samples. Categorical variables were compared using the Fisher’s exact probability test. Non-parametric Kruskal-Wallis and Mann-Whitney tests were also used to examine the associations between categorical variables and continuous or ordered outcomes. A binary logistic regression model was used to test the proposed risk factors for significance. A p value of <0.05 was considered significant.
Results
The study included 1273 eyes of 964 patients treated with epithelium-off CXL between February 2011 and July 2017: 316 eyes of 215 patients (47% of bilateral treatment) in group 1 and 957 eyes of 749 patients (27.8% of bilateral treatment) in group 2. There were no significant differences between the two groups with regard to age, gender, atopic history, maximum simulated keratometric values, minimum corneal thickness and history of microbial keratitis (table 1). Following treatment, there were no significant differences in the presence of persisting corneal haze or scarring between the two groups (p=0.57), when cases of microbial keratitis were excluded. There were no non-infective-related serious adverse events or reactions.
Demographics and clinical characteristics data of patients undergoing CXL: comparison between group 1 and group 2, as well as between total and cases with microbial keratitis (MK)
A microbial keratitis occurred in 9 eyes (0.71% of eyes) of 8 (0.83%) patients (1 case was bilateral) out of 1273 eyes. All the nine cases of microbial keratitis occurred in group 1 (incidence of 2.85%) and none in group 2 (p<0.0001; table 1). Of the eight patients who developed a microbial keratitis, five had undergone bilateral simultaneous CXL and three patients had had unilateral treatment in one eye only at the time of the development of microbial keratitis. The main characteristics of these patients are shown in tables 2 and 3. There was a 7:1 male preponderance and the average age was 21.5 years (range: 12–28 years). All were diagnosed between 1 and 5 days (mean 3.75 days) after CXL (table 3). An epithelial defect with surrounding infiltrate was present in all cases (figure 1). Six eyes had central ulcers (66.7%), and a hypopyon was present in three eyes (33.3%). The only type of micro-organism isolated was Staphylococcus aureus, which was isolated from the cornea in seven cases, from the conjunctiva in two patients, the nose in three patients and the pharynx in one patient (table 3). No specific findings were identified on confocal microscopy. The mean ulcer healing time was 5.3 days (range: 2–20 days). The presence of atopic disease was higher, although not statistically significant (p=0.4), in those patients who developed a microbial keratitis (six out of the eight patients, ie, 75%) as compared with those who did not (48%). The mean change in visual acuity (converting Snellen to logarithm of the minimum angle of resolution [logMAR] estimate) between pre-CXL and their most recent appointment post-CXL was a worsening of 0.3 logMAR (an improvement of −0.78 logMAR at best and a worsening of 0.48 logMAR at worst). No case of reduced compliance to the postoperative treatment protocol was noted among patients with keratitis.
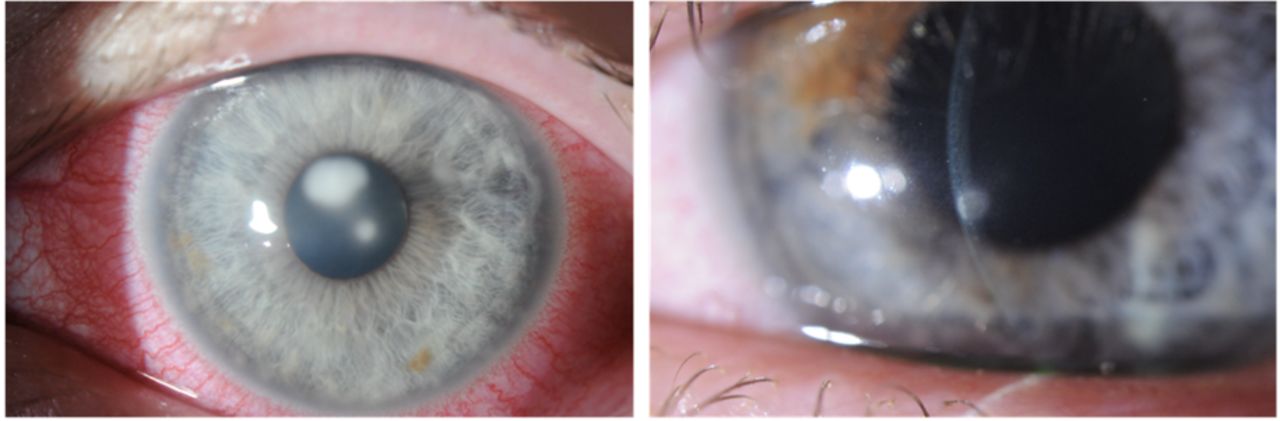
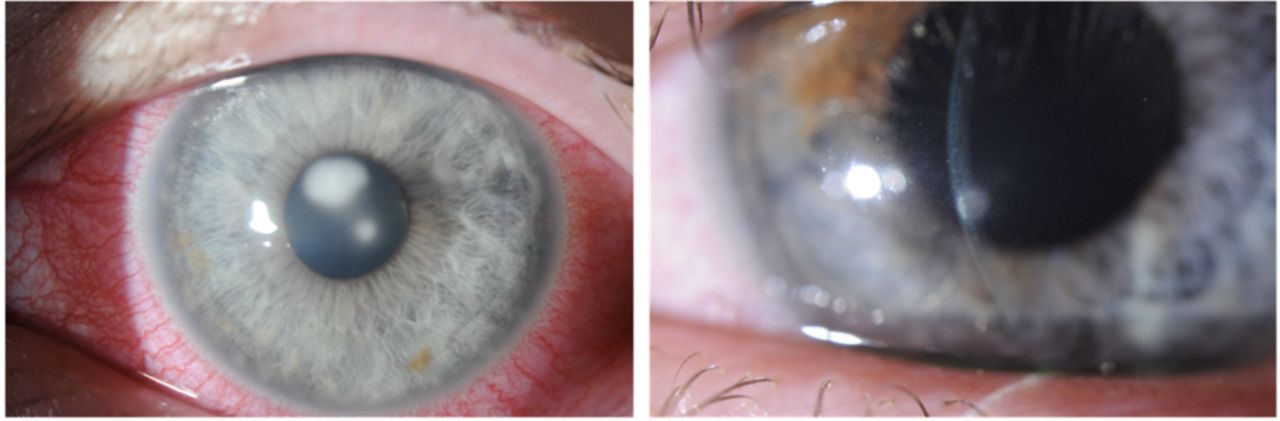{kind=link}
Corneal photographs of eyes with post-CXL keratitis. The left image shows a central corneal ulcer with infiltrate (case 3), while the right image shows a small early inferior paracentral corneal ulcer with respective infiltrate (case 6). CXL, corneal collagen cross-linking.
Detailed demographics of individual cases with microbial keratitis following CXL
Clinical characteristics and microbiology profile of microbial keratitis cases following CXL
Age, gender, preoperative minimum corneal thickness, history of atopic disease, bilaterality of treatment and preoperative maximum simulated keratometric value were not found to be significant risk factors associated with the development of microbial keratitis (table 4). The only variable that yielded statistical significance was the use of BCL and steroids before epithelial healing (p=0.005).
Univariate analysis of the association between risk factors and development of microbial keratitis after CXL
Discussion
Although CXL is considered a relatively safe procedure, rare but sight-threatening complications may occur, including microbial keratitis, presumed sterile corneal infiltrates, corneal melting, corneal haze, scarring, herpes simplex virus keratitis and corneal endothelial damage.10 11 13–20 Until modifications can be made to improve the efficacy of transepithelial CXL, removal of the corneal epithelial barrier remains a risk factor for the development of microbial keratitis following standard CXL treatment.
Previous reports have identified poor postoperative treatment compliance and hygiene and the use of a BCL as possible risk factors for the development of microbial keratitis following CXL.8–11 17 18 Maharana et al 21 published a case series of seven microbial keratitis cases (incidence 1.3%) after accelerated CXL with the use of a BCL, and concluded that younger age, atopic history, poor compliance and postoperative treatment may contribute to the development of keratitis.21 It is likely that changes in ocular flora and the use of topical steroids in patients with atopic or vernal conjunctivitis further increase the risk of postoperative keratitis.22 Shetty et al 11 used a regimen in which a BCL was placed at the end of treatment, but steroids were deferred until epithelial healing had taken place.11 Despite the deferral of steroids, four patients still developed microbial keratitis, suggesting the BCL may have been a greater risk factor for the development of microbial keratitis relative to the use of steroids.
The results of our study, which represents the largest up-to-date cohort on microbial keratitis following CXL, indicate that not using a BCL and withholding the use of topical steroids until the epithelium had healed after CXL (usually 2–5 days) were not associated with any cases of microbial keratitis. The limitations of the present study include its retrospective nature and the lack of a comparative measure of postoperative pain evaluation between the two study groups. Furthermore, due to the retrospective design of the study, it is not possible to discern whether the use of BCL, topical steroids or their combination has led to the increase in the incidence of microbial keratitis. Both of them have been identified so far in the literature as possible risk factors for the development of microbial keratitis after CXL.10 11 17–21 In all of the cases described in the systematic review of Abbouda et al,10 the postoperative treatment included steroids, and in most of them also the use of a BCL. In two large retrospective cohorts using a BCL in all patients but deferring the use of steroids until complete epithelial healing, the incidence of MK after CXL varied between 0.17% (4/2350) and 1.3% (7/532). Further prospective randomised studies are needed in order to independently evaluate the risk and benefits of postoperative use of topical steroids and BCL.
It is of note that, in the original description, Wollensak et al 1 did not describe the use of either topical steroid nor of a BCL, but rather only topical antimicrobial therapy until the epithelium had healed. The results of this study would support that view. A variety of micro-organisms have been reported in cases of post-CXL microbial keratitis, with the spectrum including Escherichia coli, Aspergillus fumigatus, Pseudomonas aeruginosa, Streptococcus and Staphylococcus species, as well as Acanthamoeba spp.,17–21 herpes simplex virus and fungi.10 It is of note, therefore, that in this study and in contrast to these reports, S. aureus was the only micro-organism isolated. In fact, S. aureus was cultured from corneal scrapes in seven out of nine cases and from contiguous sites in the remaining two cases. The clinical features in these two cases were consistent with microbial keratitis rather than sterile infiltrates.
Infections with S. aureus usually arise from endogenous sources and nasopharyngeal colonisation with S. aureus is a well-recognised risk factor.23–25 Approximately 20% of the healthy human population are persistently colonised with S. aureus and the same strain can persist over months or years.26 27 A key feature of non-ocular S. aureus infection is its recurrence, which occurs in approximately 30% of all cases.28 29 It is also of importance to note that S. aureus has been found to be associated with recurrent microbial keratitis significantly more frequently than with other bacteria.30 In addition to the nose, in some of our patients S. aureus was isolated from the ipsilateral conjunctiva. It is possible, therefore, that S. aureus may have persisted at or around the conjunctiva or lid margin in these patients as small colony variants,29 as these have been associated with persistent and recurrent infections at other sites.31 32
Persistent carriage of S. aureus in patients with keratoconus might therefore predispose these individuals to recurrent keratitis, especially in those with ocular surface disease such as atopic conjunctivitis, which was present in six of the eight patients who developed microbial keratitis. In patients with atopic or other ocular surface disease who are at an increased risk of microbial keratitis, collection of samples from the nose and conjunctiva prior to CXL followed by S. aureus decolonisation treatment prior to surgery is a consideration.
Interestingly, the combination of a large diameter BCL, antibiotics and steroids is often the treatment regimen of patients undergoing photorefractive keratectomy (PRK), and yet the keratitis rates in this group have been reported to be much lower, even less than 0.02%.33 34 As a matter of fact, Yuksel et al 35 have reported comparable colonisation rates of BCLs after PRK and CXL, with coagulase-negative staphylococci being the most frequent micro-organism.35 Although CXL can also have a presumed antimicrobial effect on corneal stroma, the difference in microbial keratitis rates could be attributed to variations in aseptic surgical conditions and, moreover, to the increased incidence of atopy among patients with keratoconus in comparison with subjects undergoing refractive surgery.
In conclusion, our results would suggest that not using a BCL and delaying the introduction of topical steroids until epithelial healing may significantly reduce the risk of developing microbial keratitis and do not seem to increase the risk of persistent corneal haze. The role of preoperative sampling of the conjunctiva and nose and prophylactic antimicrobials requires further study.
References
Footnotes
Contributors Concept and design of the study: AT, VR, MB, CW, SA, SK. Data acquisition: AT, VR, RC, RV, TN. Data analysis/interpretation: AT, VR, RC, SA, SK. Drafting of the manuscript: AT, RC, VR, SK. Critical revision of the manuscript: AT, VR, RC, RV, MB, CW, TN, SA, SK. Statistical analysis: AT, SK. Admin, technical or material support: TN, VR, RV. Supervision: MB, CW, SK. Final approval: AT, VR, RC, RV, MB, CW, TN, SA, SK.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval This retrospective cohort study was performed in adherence with the Declaration of Helsinki for research involving human subjects and after approval from the Institutional Review Board of The Royal Liverpool University Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.