Article Text

Abstract
Background/aims To monitor treatment-naïve patients with wet age-related macular degeneration (wet AMD) receiving intravitreal aflibercept (IVT-AFL) in France.
Methods RAINBOW (Real life use of intravitreal Aflibercept In FraNce - oBservatiOnal study in Wet age-related macular degeneration) is an ongoing, observational, retrospective and prospective 4-year study to assess visual (primary), anatomical and safety outcomes following IVT-AFL treatment in wet AMD patients. We report the interim 12-month outcomes in patients who have already been enrolled.
Results Safety data were analysed from 586 patients (safety analysis set); and effectiveness data were analysed from 502 patients with at least one follow-up (full-analysis set) and from 353 patients with visual acuity data at baseline and month 12. The mean (SD) best-corrected visual acuity (BCVA) was 56.7 (18.2) letters and the mean (SD) central retinal thickness (CRT) was 395.6 (140.5)µm at baseline. Most patients (76.9%) received a loading dose (first three injections within 90 days). The mean (SD) number of IVT-AFL injections over 12 months was 6.0 (2.1) and 6.6 (1.8) (patients who received a loading dose). The mean (SD) change in BCVA was 5.5 (15.0) letters and 6.8 (14.5) letters (patients who received a loading dose) at month 12 (p<0.001 vs baseline). The mean (SD) CRT reduction was –108.7 (146.8)µm and –116.4 (150.4)µm (loading dose) at month 12 (p<0.001 vs baseline). Overall, 118 (20.1%) patients experienced at least one treatment-emergent adverse event (TEAE), 1.2% experienced ocular TEAEs and 3.9% experienced serious AEs.
Conclusion This 12-month interim analysis showed that IVT-AFL was associated with sustained improvements in a real-world setting. The RAINBOW results are consistent with the VIEW clinical studies.
Trial registration number NCT02279537 Pre-results.
- intravitreal aflibercept
- wet age-related macular degeneration
- real-world evidence
- RAINBOW
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Most published observational studies in wet age-related macular degeneration (AMD) have largely been in patients treated with ranibizumab, mainly due to its earlier European approval in 2007. However, there is underdosing in clinical practice; this has been reported in several large-scale studies.
What are the new findings?
This observational study of patients with wet AMD treated with intravitreal aflibercept in France showed that visual and anatomical outcomes were improved over a 12-month period. The outcomes were consistent with the VIEW randomised studies.
How might these results change the focus of research or clinical practice?
These findings indicate that outcomes achieved in randomised studies can be achieved under real-world settings.
Introduction
It is estimated that 69 million adults in Europe will have age-related macular degeneration (AMD) by 2040.1 Most vision loss associated with AMD is caused by the neovascular/wet form of the disease.2 Anti-vascular endothelial growth factor (VEGF) agents have become increasingly popular in the treatment of this form of AMD. Intravitreal aflibercept (IVT-AFL) was approved for use in wet AMD in Europe in 2012, with bimonthly dosing (after three initial doses) and extension after 12 months. IVT-AFL is known to target VEGF and placental growth factor, which are key mediators in the progression of neovascularisation underlying wet AMD.3 4 IVT-AFL 2 mg every 8 weeks (2q8) after three initial doses was shown to be noninferior to ranibizumab 0.5 mg monthly, with comparable ocular safety, in the VIEW studies.5 6 However, the results achieved under strict protocols in randomised studies may not always be achieved in routine practice; this has prompted an interest in real-world studies.
Most published observational studies have largely been in patients treated with ranibizumab, mainly due to its earlier European approval in 2007. Ranibizumab 0.5 mg was initially approved with monthly or as-needed dosing after a loading dose (induction) coupled with regular monitoring. However, these regimens may have contributed to underdosing in clinical practice; this has been reported in several large-scale studies.7–9
The aim of this is to report the 12-month outcomes from the RAINBOW (Real life use of intravitreal Aflibercept In FraNce - oBservatiOnal study in Wet age-related macular degeneration) study. RAINBOW is an observational study to monitor the effectiveness and safety of IVT-AFL when used in treatment-naïve patients with wet AMD in routine clinical practices across France.
Materials and methods
RAINBOW is an ongoing, observational, 4-year study to monitor the effectiveness and safety of IVT-AFL in treatment-naïve patients with wet AMD. Patients were included retrospectively and prospectively. The study was conducted in 55 centres across France. Patients who received their first IVT-AFL injection between January 2014 and March 2015 were screened and will be followed for a period of 4 years or until study discontinuation. Herein, we report the 12-month outcomes. No independent ethics committee and institutional review board approval was obtained due to its observational design in accordance with the requirements of local law and regulations in France; however, the protocol was reviewed and approved by a French data privacy committee (Comité Consultatif sur le Traitement de l’Information en Matière de Recherche dans le Domaine de la Santé and Commission Nationale de l’Informatique et des Libertés). All patients provided written informed consent to participate.
Participants
Patients aged ≥50 years diagnosed with wet AMD and prescribed IVT-AFL by their physician were eligible. Prior or current treatment with any anti-VEGF agent or macular laser in the study eye was not allowed. The study eye was defined as the worst-seeing eye of each patient, but the second eye was also considered if it was treatment naïve. Patients were excluded if they did not meet the indication criteria for IVT-AFL, if they had another retinal disease (diabetic retinopathy, diabetic macular oedema, myopic choroidal neovascularisation, retinal vein occlusion, central serous chorioretinopathy or angioid streaks) or if they were participating in any other interventional study.
Assessments
The primary aim was to evaluate the mean change in best-corrected visual acuity (BCVA) from baseline to 12 months. Other assessments included mean change in central retinal thickness (CRT) and safety outcomes at month 12. Patient medical records were evaluated for demographic and clinical characteristics. For retrospectively enrolled patients, resource use, tests, treatment(s) and outcomes were also obtained from medical records. For prospectively enrolled patients, this information was recorded at routine follow-up visits. All adverse events (AEs) occurring after the first injection of IVT-AFL were documented in the electronic case report form.
Statistical analyses
It was estimated that 600 patients should be screened in order to achieve approximately 390 usable patient datasets at 4 years. These estimates were based on the VIEW studies, using a 10% annual dropout rate.5 Safety analyses were based on data from patients who received at least one IVT-AFL injection (safety analysis set). Effectiveness analyses (resource use and anatomical outcomes) were based on patients who also had documented assessments in the study eye at baseline and at least one follow-up visit (full analysis set, FAS), and visual acuity analyses were based on patients who had documented visual acuity assessments at baseline and month 12 (FAS targeted). Outcomes were also assessed in patients who received a loading dose (the first three IVT-AFL injections within 90 days).
Visual acuity was measured using the Early Treatment Diabetic Retinopathy Study (ETDRS) letter chart or any visual scale. The visual acuity readings were then converted to a standardised score using a conversion chart (online supplementary table 1). Final visual outcomes were also categorised by the percentage of patients who gained 0–4, 5–9, 10–14 or ≥15 letters, the percentage of patients who lost >15 letters, and by visual acuity categories (<50, [50–55], [55–70] and ≥70 letters) at month 12. Outcomes were also assessed in subgroups based on presence of fluid or pigment epithelium detachment (PED) at baseline and injection (<7, ≥7) categories; the injection categories were used to compare with other real-world studies, such as LUMINOUS.10 Lesion type was defined according to fluorescein angiography and indocyanine green examinations.
Supplemental material
The statistical analyses were exploratory and descriptive. The mean changes in BCVA and CRT from baseline to month 12 were analysed using t-tests, with a significance level of 5%. Sensitivity analyses were also performed on visual acuity outcomes using a last observation carried forward (LOCF) approach to account for missing data and replacement by the median population values; these were performed using the FAS population. All statistical analyses were performed using SAS Enterprise Guide V.7.13 (SAS Institute).
Results
Participants
A total of 615 patients were screened. Safety data were analysed from 586 patients (safety analysis set). Resource use, anatomical outcomes and sensitivity analyses were determined using data from 502 patients (FAS) and visual acuity outcomes were analysed from 353 patients with visual acuity data at baseline and month 12 (FAS targeted) (see online supplementary figure 1). The baseline characteristics are shown in table 1. Most patients underwent fluorescein angiography examination (75.4%; n=377/500) and indocyanine green examination (56.4%; n=282/500) at baseline. Most patients (76.9%; n=386/502) also received an IVT-AFL loading dose. The mean (SD) number of IVT-AFL injections over 12 months was 6.0 (2.1) (n=502) and 6.6 (1.8) in patients who received a loading dose (n=386). Most patients were treated with ‘as-needed’, ‘treat and extend (T&E)’ or ‘observe and plan’ protocols; 9.8% (n=49/502) of patients received three initial IVT-AFL injections followed by treatment every 8 weeks.
Demographic and baseline characteristics
Only 13.5% of patients (n=68/502) switched treatment during the study, with most switching to another anti-VEGF agent (82.4%; n=56/68), predominantly ranibizumab (96.4%; n=54/56). The main reasons for switch included lack of effectiveness (73.5%; n=50/68), AEs/serious AEs (SAEs) (2.9%; n=2/68) and other/unknown reason (23.5%; n=16/68). Some patients switched back from ranibizumab to IVT-AFL (38.9%; n=21/54) (reasons not recorded). The mean (SD) number of clinic visits was 9.4 (2.3) and 9.8 (2.0) (patients who received a loading dose).
Visual and anatomical outcomes
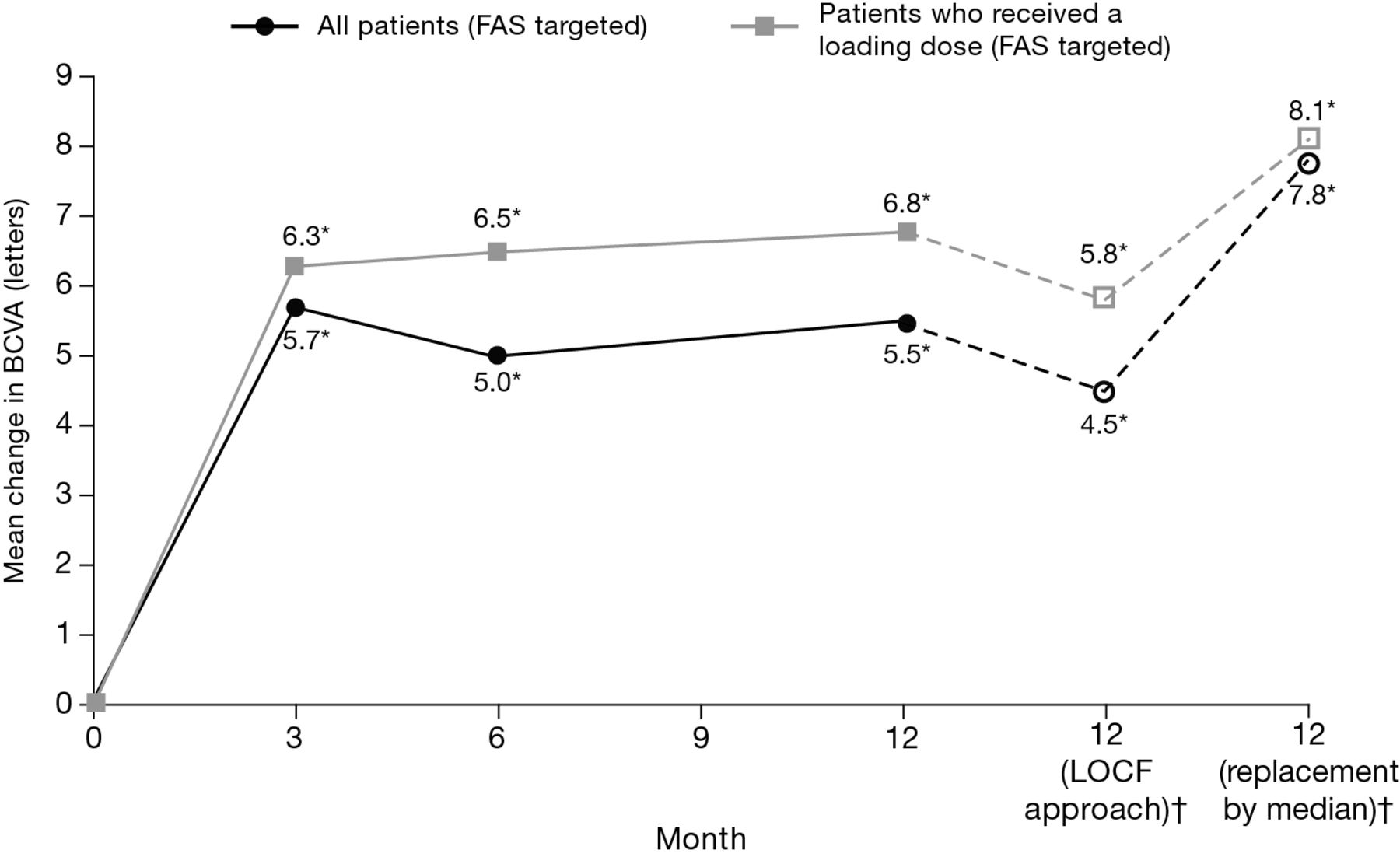
The mean (SD) change in BCVA was 5.5 (15.0) letters (n=353) and 6.8 (14.5) letters in patients who received a loading dose (n=284) (both p<0.001) at month 12 (figure 1). The mean (SD) change in BCVA using an LOCF approach was 4.5 (15.9) letters (n=502) and 5.8 (15.2) letters in patients who received a loading dose (n=386) (both p<0.001 vs baseline) at month 12. The mean (SD) change in BCVA using replacement by the population median was 7.8 (16.7) letters (n=502) and 8.1 (15.7) letters in patients who received a loading dose (n=386) (both p<0.001 vs baseline) at month 12.

Mean change in BCVA (letters) from baseline to month 12 in patients receiving IVT-AFL. All patients (FAS targeted): n=360 (month 3) and n=353 (months 6, 12); for patients who received a loading dose (FAS targeted): n=290 (month 3), n=276 (month 6) and n=284 (month 12) (treatment decisions were made by the physician). LOCF and median replacement analysis (FAS) n=502 (all) and n=386 (patients who received a loading dose). *P<0.001 versus baseline. FAS population. BCVA, best-corrected visual acuity; FAS, full analysis set; IVT-AFL, intravitreal aflibercept; LOCF, last observation carried forward.
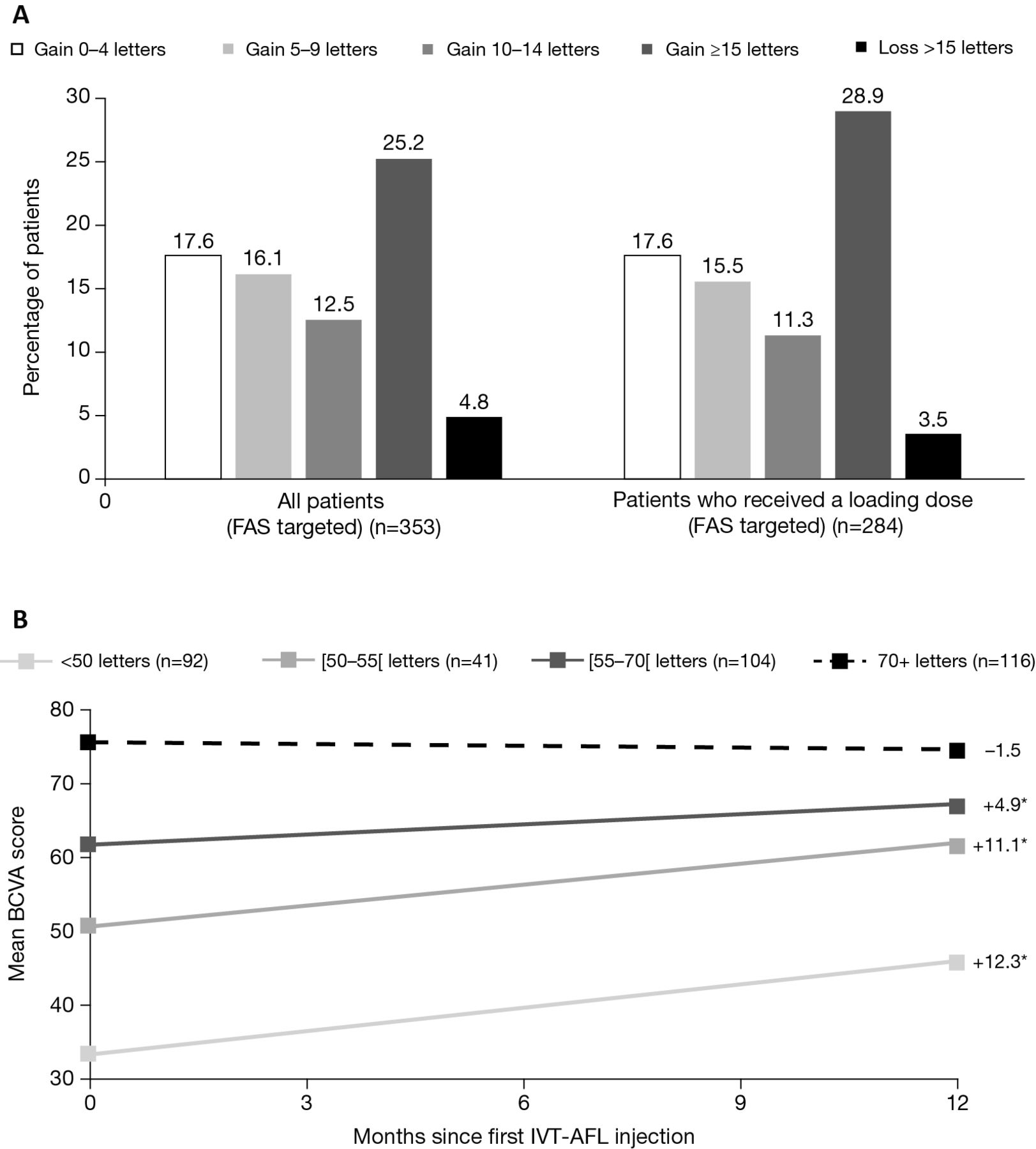
The proportions of patients who gained ≥15 letters were 25.2% (n=89/353) and 28.9% in patients who received a loading dose (n=82/284) (figure 2A). When patients were stratified according to baseline visual acuity categories (<50, [50–55], [55–70] and ≥70 letters), the mean (SD) numbers of injections in these categories were 6.3 (1.9), 6.9 (2.0), 6.2 (1.9) and 6.1 (2.0), and the mean (SD) letter changes were 12.3 (16.7), 11.1 (15.3), 4.9 (13.4) and –1.5 (11.3), respectively (figure 2B). The percentages of patients with BCVA ≥70 letters were 45.9% (n=162/353) and 45.4% (patients who received a loading dose; n=129/284) at month 12 (online supplementary figure 2).

Visual acuity outcomes in patients (FAS targeted) receiving IVT-AFL based on (A) 0–4, 5–9, 10–14 and ≥15 letter gains or >15 letter loss at month 12 and (B) the mean letter gains when patients were stratified by final visual acuity groups at month 12 (treatment decisions were made by the physician). *P<0.001 versus baseline. BCVA, best-corrected visual acuity; FAS, full analysis set; IVT-AFL, intravitreal aflibercept
There was also a significant mean (SD) reduction in CRT at month 12; the mean (SD) change was –108.7 (146.8) (n=333) and –116.4 (150.4) µm in patients who received a loading dose (n=275) (both p<0.001 vs baseline) (figure 3). These improvements were evidenced by month 3, and maintained through month 12.

{kind=link}
{kind=link}
{kind=link}
Mean change in CRT (µm) from baseline to month 12 in patients receiving IVT-AFL. All patients (FAS): n=334 (month 3), n=338 (month 6) and 333 (month 12); for patients who received a loading dose (FAS): n=267 (month 3), n=278 (month 6) and n=275 (month 12) (treatment decisions were made by the physician). *P<0.001 versus baseline. CRT, central retinal thickness; FAS, full analysis set; IVT-AFL, intravitreal aflibercept.
Subgroups
The mean change in BCVA (letters) was significantly improved in patients (n=353) with intraretinal or subretinal fluid or PED at baseline (all p<0.001). There were mean BCVA improvements of 6.8 letters in patients who received ≥7 injections (n=165) and 4.3 letters in patients who received <7 injections (n=188) (online supplementary table 2). There was also a reduction in the proportion of patients (n=474) with fluid (intraretinal, subretinal and subretinal pigment epithelium) and PED over the 12-month study (online supplementary table 3). Choroidal neovascularisation leakage reduction was also observed.
Safety
Overall, 20.1% (n=118/586) of patients experienced at least one treatment-emergent AE (TEAE), and 1.9% experienced at least one treatment-related TEAE (table 2). The most common ocular AEs were vitreous floaters (1.9%), lacrimation increased (1.0%) and eye pain (0.9%). The most common nonocular AEs included product use issue (2.9%), cardiac failure (0.9%), bronchitis (0.9%) and drug hypersensitivity (0.9%). Serious AEs were reported in 3.9% of patients. There was one treatment-related transient ischaemic attack.
Safety outcomes at month 12
Discussion
This 12-month interim analysis of the RAINBOW study showed that visual and anatomical improvements were achieved in treatment-naïve patients with wet AMD receiving IVT-AFL in a real-world setting. The outcomes observed in patients who received a loading dose (first three injections within 90 days) were favourable compared with those achieved in randomised studies. In the VIEW studies, the mean change in BCVA was 8.4 letters, the percentage of patients gaining ≥15 letters was 30.9% and the percentage of patients maintaining visual acuity (losing <15 letters) was 95.3% at month 12 in the combined IVT-AFL 2 mg bimonthly group (2q8) after three loading doses.6 These patients received ~7.5 IVT-AFL injections over 12 months. There were, however, some differences in baseline characteristics between RAINBOW and VIEW. The mean age and baseline BCVA were both higher in RAINBOW than VIEW, and the BCVA was outside the VIEW inclusion criteria in about 20% of patients enrolled in RAINBOW (<25 letters in 7.9% and >73 letters in 13.2%, respectively). The IVT-AFL regimen in the RAINBOW study was also different from VIEW, with only 10% of patients receiving the same protocol. Another observational study in the UK, which monitored treatment-naïve patients with wet AMD (58 eyes) receiving IVT-AFL bimonthly treatment (after a loading dose), reported similar visual outcomes to RAINBOW.11 The baseline BCVA was 54.1 ETDRS letters, and the mean improvement in BCVA was 4.67 letters at month 12; 17.2% of patients gained ≥15 letters, and 96.6% of patients avoided losing >15 letters at month 12. The mean reduction in CRT was lower (–35.36 µm) than in RAINBOW, but the baseline CRT was also lower (284.2 µm). The mean number of IVT-AFL injections was similar (7.1), but the mean number of clinical visits was lower (4). These authors used fixed IVT-AFL dosing. The IVT-AFL regimen used in RAINBOW was more variable and may warrant further investigation.
RAINBOW also highlighted an improvement in outcomes with IVT-AFL compared with earlier observational studies (such as AURA) that monitored ranibizumab.7 There may be a number of reasons for this, including improvements in patient management (a number of ranibizumab studies were published several years ago) and differences in dosing regimens between the two agents. For example, in the AURA study, which monitored outcomes in 2227 patients with wet AMD, visual acuity declined over time to 2.4 letters at year 1 and 0.6 letters at year 2, and the mean number of ranibizumab injections was 5.0 at year 1 and 2.2 at year 2.7 In the French cohort of AURA, which comprised 398 patients, the mean change in visual acuity was 0.8 letters at year 1 and –1.1 letters at year 2, the mean number of ranibizumab injections was 4.4 (year 1) and 1.9 (year 2), and the mean number of visits was 8.5 (year 1) and 4.9 (year 2). More recent ranibizumab studies have reported variable results. A larger analysis of 18 358 eyes from 20 real-world studies also found that outcomes did not reflect those reported in randomised studies. In this analysis, the mean change in visual acuity was 2.9 letters at year 1 and the mean number of ranibizumab injections was 5.5.8 In comparison, interim findings from the ongoing LUMINOUS study showed that the mean change in BCVA was 4.4 letters at month 12, and the mean number of ranibizumab injections was 4.7 in 706 treatment-naïve patients with wet AMD.10 A recent meta-analysis of ~26 360 patients from 42 real-world studies reported better outcomes with ranibizumab T&E compared with as-needed, which was used in some earlier studies. The mean change in visual acuity was 8.8 versus 3.5 letters and the mean number of injections was 6.9 versus 4.7 at year 1, respectively.9 Unfortunately, outcomes by IVT-AFL regimen (as-needed, T&E or observe and plan) were not explored in this interim analysis of RAINBOW.
RAINBOW also showed that IVT-AFL was well tolerated in clinical practice. However, the incidence of ocular AEs was generally lower in RAINBOW than in VIEW, which may be due to differences in reporting of AEs between randomised and observational studies, with the possibility of under-reporting. These findings were; however, consistent with the known safety profile of IVT-AFL in wet AMD.5 6
It must be noted that there are a number of limitations inherent with the observational design of the RAINBOW study. Evaluation of visual acuity was performed using EDTRS letter charts or any other visual scale in this study. However, the use of different charts may introduce bias, especially in the measurement of the number of letters gained or lost after treatment. The findings are also based on one European country, which may not be representative of other European countries and their respective reimbursement strategies.
In conclusion, this 12-month analysis highlights the effectiveness and safety associated with IVT-AFL in treatment-naïve patients with wet AMD in routine practice. Patients who received a loading dose also experienced better outcomes at month 12, although the correlation needs to be established by a multivariate analysis as these patients also received a mean of 0.6 more IVT-AFL injections. Ocular TEAEs were also consistent with the known safety profile of IVT-AFL. RAINBOW showed that outcomes achieved with IVT-AFL (after a loading dose) in randomised studies, such as VIEW, can be achieved in a real-world setting.
Acknowledgments
Medical and scientific coordination were performed by Armelle Baillou-Beaufils, Head of Ophthalmology Department (Bayer France) and Ingrid Dufour, Clinical Research and Medical Advisor (Bayer France). Operational coordination was performed by Anne Marie Delaunay, Head of PMS Group (Bayer France).
Footnotes
Contributors MW contributed to the design; data acquisition, analysis and interpretation; and preparation and final review of the manuscript. LV contributed to the design; data acquisition, analysis and interpretation; and preparation and final review of the manuscript. FC contributed to the design; data acquisition, analysis and interpretation; and preparation and final review of the manuscript.CF contributed to the design; data acquisition, analysis and interpretation; and preparation and final review of the manuscript. IA contributed to the design; data acquisition, analysis and interpretation; and preparation and final review of the manuscript. S-Y C contributed to the design; data acquisition, analysis and interpretation; and preparation and final review of the manuscript.
Funding The RAINBOW study was funded by Bayer Pharmaceuticals. The funding organisation participated in the design and conduct of the study, analysis of the data and preparation of the manuscript.
Competing interests MW: Alcon, Alimera, Allergan, Bayer, Novartis, Thea; FC: Allergan, Bayer, Novartis, Roche; CF: Alcon, Bayer, Novartis; IA: Bayer; Novartis; S-YC: Alcon, Allergan, Bayer, Novartis, Thea.
Ethics approval CCTIRS and CNIL.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Availability of the data underlying this publication will be determined according to Bayer’s commitment to the EFPIA/PhRMA "Principles for responsible clinical trial data sharing". This pertains to scope, time point and process of data access.
As such, Bayer commits to sharing upon request from qualified scientific and medical researchers patients-level clinical trial data, study-level clinical trial data, and protocols from clinical trials in patients for medicines and indications approved in the United States (US) and European Union (EU) as necessary for conducting legitimate research. This applies to data on new medicines and indications that have been approved by the EU and US regulatory agencies on or after January 01, 2014.
Interested researchers can use to request access to anonymized patient-level data and supporting documents from clinical studies to conduct further research that can help advance medical science or improve patient care. Information on the Bayer criteria for listing studies and other relevant information is provided in the Study sponsors section of the portal.
Data access will be granted to anonymized patient-level data, protocols and clinical study reports after approval by an independant scientific review panel. Bayer is not involved in the decisions made by the independant review panel. Bayer will take all necessary measures to ensure that patient privacy is safeguarded.
Collaborators The RAINBOW study investigators: Professor Salomon Yves Cohen, Dr Patrick Simon, Dr Alain Donati, Dr Valérie Krivosic, Dr Martine Mauget Faysse, Dr Frédéric Queguiner, Dr Sophie Navarre, Dr Concetta Li Calzi, Dr Elodie Bousquet, Dr Frédéric Chiambaretta, Dr Sylvia Nghiem-Buffet, Professor Catherine Creuzot Garcher, Dr Isabelle Aknin, Professor Michel Weber, Dr Sébastien Bruneau, Dr Bertille Tourame de Massiac, Dr Jean-François Boulet, Dr Aude Danan Husson, Dr Mathieu Lehmann, Dr Eve Rousseau, Dr Franck Fajnkuchen, Dr Joël Uzzan, Dr Saddek Mohand Said, Dr Olivier Lebreton, Dr Houiem Jeguirim, Professor Carl Arndt, Dr Bénédicte Briend Joulain, Dr Corinne Gonzalez, Professor Frédéric Matonti, Dr Isabelle Sillaire Houtmann, Dr Gabriel Quentel, Dr Amélie Lecleire-Collet, Dr Jean-François Girmens, Dr Hélène Masse, Dr Claire Scemmama, Dr Jonathan Benesty, Dr Anne Robinet Combes, Professor Corinne Dot, Dr Jean-Christophe Courjaret, Dr Stéphane Dumas, Dr Vincent Parier, Dr Christian Delhay, Dr Martine Ullern, Professor Stéphanie Baillif, Dr Ghislaine Ducos de Lahitte, Dr Tony Garcia, Dr Joël Gambrelle, Dr Emilie Agard, Dr Bernard Joannot, Dr Sylvain Blanchard, Dr Valérie Le Tien, Professor Jean-Claude Quintyn, Dr Franck Becquet, Dr Abdelghani Asrarguis, Dr Laurent Velasque, Dr Mickaël Afriat, Dr Christiane Ramahefasolo, Dr Hussam El Chehab, Dr Arnaud George, Dr Philippe Verdier, Dr Dagmar Kuhn, Professor Laurent Kodjikian, Dr Cécilia Leal, Dr Laurence Rosier, Professor Solange Milazzo, Dr Olga Kirsch, Dr Aurélie Russo, Dr Charles Pêcheur, Professor Christophe Chiquet, Dr Isabelle Aubry Quenet, Dr Nabil Salame, Dr Zainab Bentaleb, Dr Violaine Colasse Marthelot, Dr Marcel Dominguez, Dr Mounir Benzerroug, Dr Laurent Khaitrine, Dr Nicolas Alfonsi, Dr Alain Simoni, Professor Florent Aptel, Dr Caroline Serny, Professor Jean-François Korobelnik, Dr Thibaud Mathis, Dr Maddalena Quaranta-El-Maftouhi, Dr Eric Fourmaux, Dr Andrei Drimbea, Dr Benjamin Guigui, Dr Vincent Paoli, Dr Frédéric Sanian, Dr Thierry Zhou, Dr Florence Coscas, Dr France Combillet, Dr Olivier Jankowski, Professor Maher Saleh, Dr Hassiba Oubraham, Dr Karim Atmani, Dr Virginie Martinet, Dr Addel Chibani, Dr Nicolas Chobeaux, Dr Ralitsa Hubanova, Dr Catherine Francais, Professor Marie-Noëlle Delyfer, Professor Ramin Tadayoni, Dr Sébastien Guigou, Professor Nicolas Leveziel, Dr Sandrine Allieu, Dr Henrik Sagnieres, Professor Thi Ha ChauTran, Dr Nathalie Massamba, Dr Catherine Favard, Dr Marie-Bénédicte Rougier, Dr Ali Erginay, Dr Caroline Marc, Dr Michèle Boissonnot, Dr Charlotte Rohart, Dr Hatem Zeghidi, Professor Gisèle Soubrane and Dr Piotr Krawczyk.
Presented at Annual Meeting of the Association for Research in Vision and Ophthalmology (ARVO) (1–5 May 2016, Seattle, Washington). 16th European Society of Retina Specialists Congress (16th EURETINA) (08–11 September 2016 / Copenhagen, Denmark). Imaging & Managing Macular Diseases (Maculart) meeting (2–4 July 2017; Paris, France). 123e Congres de la Societe Francaise d’Ophtalmologie (SFO 123rd) Congress (05-09 May 2017, France, Paris). 49th Annual Congress of the Royal Australian and New Zealand College of Ophthamologists (RANZCO) (28 October to 01 November 2017, Perth, Australia).
Patient consent for publication Obtained.