Article Text

Abstract
Objective To describe the safety and effectiveness of CyPass supraciliary microstent implantation alone in eyes with open-angle glaucoma (OAG) followed up for up to 3 years.
Methods and analysis This registry study included subjects with primary or secondary OAG who underwent CyPass Micro-Stent implantation alone at 12 sites in four European countries to reduce intraocular pressure (IOP) and/or use of IOP-lowering medications. The primary safety outcome was the incidence of adverse events. Secondary efficacy outcomes included mean changes from baseline in IOP and IOP-lowering medications. Eyes were subgrouped into those with low (< 21 mm Hg) and high (> 21 mm Hg) baseline IOP.
Results This study included 225 eyes of 178 patients, with mean baseline IOP of 22.6 ± 6.7 mm Hg and a mean 2.2 ± 1.2 medications per eye. Common ocular adverse events included device obstruction (10.2%), IOP elevation > 10 mm Hg during follow-up (8.9%), retinal complications (4.4%) and loss of > 2 lines of best-corrected visual acuity (2.7%). Seventy-one eyes (31.6%) required secondary glaucoma surgery, with trabeculectomy (33 eyes) and second microstent implantation (13 eyes) being most common. At months 6–36, mean IOP reductions ranged from 4.4 to 5.1 mm Hg (15.8%–19.5%) and mean medication reductions from 0.2 to 1.2 (9.1%–54.5%). Mean IOP reduction was greater in eyes with higher than lower baseline IOP. Both subgroups showed reductions of 0.5–1.0 medication at 12–18 months.
Conclusion CyPass microstent implantation demonstrated a safety profile consistent with other minimally invasive glaucoma surgeries and effectively lowered IOP for up to 3 years in eyes with OAG.
- micro-stent
- open-angle glaucoma
- intraocular pressure
- hypotensive medication
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Implantation of the CyPass microstent into eyes with open-angle glaucoma (OAG) reduces intraocular pressure (IOP) by creating a permanent conduit for aqueous humour into the supraciliary and suprachoroidal spaces.
What are the new findings?
CyPass microstent implantation alone, without cataract surgery, demonstrated a safety profile consistent with other minimally invasive glaucoma surgeries and effectively lowered IOP for up to 3 years in eyes with OAG.
How might these results change the focus of research or clinical practice?
Real-world patients with OAG may benefit from implantation of the CyPass microstent.
Introduction
Medical therapy is the traditional first-line approach to management of open-angle glaucoma (OAG).1 Laser therapy is generally considered a second-line intervention, and surgery has historically been reserved for eyes refractory to less invasive approaches. This treatment pattern reflects the known risks of each treatment modality and progresses from lowest to highest risk. Traditional glaucoma surgical procedures—trabeculectomy and tube-shunts—are characterised by a host of potential complications that arise both from the surgery itself and from the creation of a subconjunctival filtering bleb.2 These complications can be sight-threatening and often require secondary surgical procedures to correct.
Recently, the advent of a variety of minimally invasive glaucoma surgeries (MIGS) has offered an array of procedures that, while generally less successful in lowering intraocular pressure (IOP) than trabeculectomy, have more favourable safety profiles.3 This trade-off—sacrificing efficacy for safety—is appropriate in several clinical settings, including in patients with early glaucoma, those with borderline IOP control, and those wishing to reduce their medication burden.
MIGS procedures use several strategies for IOP reduction.3 Some of these procedures were developed to bypass the trabecular meshwork—where aqueous outflow resistance arises in glaucomatous eyes—and deliver aqueous humour to Schlemm’s canal. Other procedures seek to access the uveoscleral outflow pathway by shunting aqueous humour into the supraciliary/suprachoroidal space. Among the latter is the CyPass supraciliary microstent (Alcon Laboratories, Fort Worth, Texas, USA), a 6.35 mm long polyimide tube, implanted via an ab interno approach through the anterior chamber angle into the supraciliary space, that reduces IOP by creating a permanent conduit for aqueous humour into the supraciliary and suprachoroidal spaces.4
This device has an inner diameter of 0.30 mm and an outer diameter of 0.43 mm, selected to ensure adequate flow while minimising the risks of hypotony arising from overfiltration. Three retention rings on the proximal end of the device secure its position once implanted. A pivotal randomised controlled trial showed that a combination of the microstent and cataract surgery resulted in significantly greater reductions in IOP and IOP-lowering medication use than cataract surgery alone at 24 months.5
The CyPass Clinical Experience (CyCLE) trial was a multicentre, open-label, long-term registry trial of European subjects with glaucoma who underwent implantation of the microstent with or without cataract surgery. The primary goal of this study was to characterise the real-world safety and effectiveness profiles of the procedure, for up to 3 years, when used outside the constraints of a clinical trial. This analysis reports the up to 3 year safety and efficacy of microstent implantation alone, without cataract surgery, in eyes with open-angle glaucoma.
Methods
This registry trial was performed at 12 centres in four countries in Europe (Germany, Spain, Bulgaria and Poland), in which the microstent has been approved for standalone use. Preoperative, intraoperative and postoperative data were collected using standardised forms. Surgeons were permitted to enrol preoperative subjects prospectively and postoperative subjects retrospectively. The study protocol was approved by the overseeing ethics committee of each participating institution, and all enrolled subjects (whether data were collected prospectively or retrospectively) provided written informed consent. This trial was registered at clinicaltrials.gov under the identifier NCT01097174.
Subjects
Eligible subjects included men and women aged ≥18 years, diagnosed with OAG, for whom supraciliary microstent implantation was determined to be the appropriate next step for glaucoma management. Surgery was performed to reduce IOP and/or to reduce the number of IOP-lowering medications, with no specific thresholds for either. Subjects with normal-tension OAG (untreated IOP <21 mm Hg), narrow-angle glaucoma (Shaffer grade <3), uveitic glaucoma and neovascular glaucoma were excluded, as were subjects with congenital abnormalities of the anterior chamber or angle, or intolerance or hypersensitivity to topical anaesthetics, miotics, mydriatics or polyimide. Data were collected from one or both eyes of eligible subjects.
Study design
Data were collected preoperatively and 1 day, 1 week and 1, 3, 6, 12, 18, 24 and 36 months postoperatively. Adverse events were also assessed intraoperatively. Subjects enrolled prospectively were seen according to this schedule. For subjects registered retrospectively, data were drawn from visits closest to these scheduled visits. Parameters assessed at each study visit for each eye included the number of current glaucoma medications, best-corrected visual acuity (BCVA), IOP, slit lamp examination results, and adverse events.
The microstent was implanted according to the manufacturer’s recommendations for use. Briefly, the procedure was performed in a surgical facility under topical anaesthesia and intracameral lidocaine. Miosis was achieved with a topical or intracameral miotic agent. The subject’s head and the microscope were adjusted to permit visualisation of the anterior chamber angle by intraoperative gonioscopy. A paracentesis was fashioned opposite the planned implantation site and the anterior chamber was filled with the ophthalmic viscosurgical device. The commercial microstent package contains the device, a handheld applier, and a loader to place the device onto the applier. Once the device was loaded onto the guidewire at the tip of the applier, it was inserted into the anterior chamber through the paracentesis and advanced to the opposite angle. The tip of the guidewire was placed at the junction of the ciliary body and scleral spur. The guidewire, curved slightly to match the contour of the perilimbal sclera, was smoothly advanced into the tissue plane between the ciliary body and the sclera until only the first of the three retention rings remained visible in the anterior chamber. A button on the applier was depressed to withdraw the guidewire from the implanted microstent, and the applier was withdrawn from the eye. As CyCLE was a registry study designed to mimic real-world clinical practice, there was no specific protocol-mandated postoperative care. Postoperative care was at the discretion of each investigator and included a regimen of antimicrobial and anti-inflammatory medications.
Study outcomes
The primary safety outcome was the incidence of intraoperative and postoperative adverse events. Investigators determined if adverse events were likely attributable to the study device or implantation procedure. Measures of surgical effectiveness, including mean changes in IOP and in IOP-lowering medications from baseline to each postoperative time point, were secondary outcomes and are presented using descriptive statistics. Some eyes underwent surgery with the primary goal of IOP reduction; in these eyes, a change in the number of medications would not necessarily be expected. Likewise, some eyes underwent surgery with the primary goal of reducing reliance on IOP-lowering medications; in these eyes, a change in IOP would not necessarily be expected. The goal of surgery (reduced IOP vs reduced medication burden) was not formally declared preoperatively. To better characterise these subject-specific goals, eyes on medication were divided into two subgroups, with baseline treated IOP <21 mm Hg and IOP >21 mm Hg, with the assumption that the former primarily sought medication reduction while the latter primarily sought IOP reduction. As this was planned as a descriptive study and no a priori hypothesis was evaluated, no formal power and sample size analyses were performed.
Results
The CyCLE study enrolled 470 eyes of 390 patients undergoing micro-stent implantation with or without cataract surgery. Of these, 225 eyes of 178 patients underwent microstent implantation alone and are included in this analysis. The baseline demographic and clinical characteristics of these subjects are shown in table 1. Subjects were of mean age 72 years, were evenly divided between men and women and almost all were Caucasian. Most were pseudophakic and required two or more IOP-lowering medications for glaucoma management at the time of surgery.
Demographic and baseline characteristics of study subjects
Of the 225 eyes, 112 were followed for a full 3 years. Reasons for shorter follow-up included secondary glaucoma surgery in 71 eyes, loss to follow-up in 13, subject decision in 13, subject death in 12, adverse event in 1 and other in 3.
Safety outcomes
The safety population included all 225 eyes that underwent standalone microstent implantation. Table 2 shows ocular adverse events and secondary surgical interventions in these eyes. The most frequently observed ocular adverse event was device obstruction, which occurred in 23 eyes (10.2%). Other adverse events noted in >2% of eyes included ≥10 mm Hg elevations in IOP from baseline at any postoperative time point (8.9%); retinal complications, including progression of age-related macular degeneration and cystoid macular oedema (4.4%); and loss of >2 lines of BCVA, usually related to retinal complications (2.7%).
Adverse events and second surgical interventions (n=225)
Device obstruction was predefined as CyPass obstructed by iris, vitreous, lens, fibrous overgrowth, fibrin or blood. All of the observed obstructions involved the proximal opening and not suprachoroidal scarring. Microstent placement was evaluated postoperatively by gonioscopic examination, with only the most proximal retention ring and the collar/device opening visible when the microstent was placed correctly. The overwhelming majority of device obstruction events (20/23, 86.9%) was related to incorrect device positioning; that is, the obstruction was related to the microstent being advanced too far into the supraciliary space, resulting in occlusion of the anterior device opening. Device placement in these eyes was more posterior than optimal, with either the entire device being not visible or only its collar being visible. In addition, three eyes experienced transient obstruction, caused by blood in the lumen, during the immediate postoperative period. YAG laser photolysis was successfully employed to remove stent blockage in five eyes. Of the 46 eyes experiencing obstruction in both the implantation plus cataract surgery and standalone implantation cohorts, 28 (61%) had IOP≤21 mm Hg at the last study visit.
Study eyes underwent a total of 105 secondary surgical procedures (table 2). Of these, glaucoma procedures were the most common (71 eyes; 31.6%); this included one eye that underwent two secondary glaucoma surgeries within 1 month, laser peripheral iridotomy and trabeculoplasty. Glaucoma procedures included trabeculectomy (33 eyes, 14.7%), implantation of a second microstent (13 eyes, 5.8%), cyclophotocoagulation (10 eyes, 4.4%), tube-shunt (5 eyes, 2.2%), deep sclerectomy (4 eyes, 1.8%), another MIGS procedure (4 eyes, 1.8%) and laser trabeculoplasty or iridotomy (3 eyes, 1.3%). Nineteen eyes (8.4%) underwent cataract surgery and seven (3.1%) underwent device-related procedures: three (1.3%) to lyse tissue obstructing the device, two (0.9%) to reposition the device and two (0.9%) to explant the device (one due to persistent hypotony and the other to persistent corneal oedema).
Most adverse events occurred within the first 12 months postoperatively; as reported previously, there were no serious adverse events, and the postoperative complications that did occur were minor and of mild to moderate severity.6Figure 1 presents the distribution over time of key adverse events.
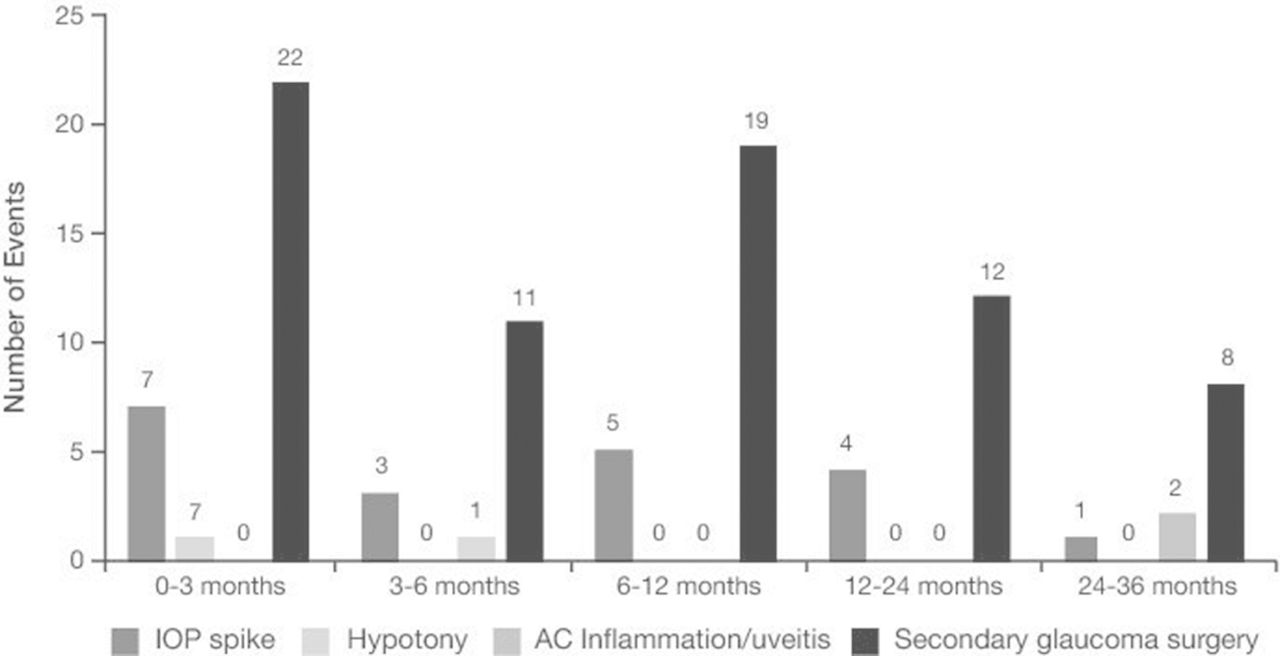
Distribution of occurrence of key adverse events between 0 and 36 months following CyPass implantation alone. IOP spike=IOP ≥10 mm Hg vs preoperative IOP. Hypotony=clinically significant as determined by the investigator. IOP, intraocular pressure.
Efficacy outcomes
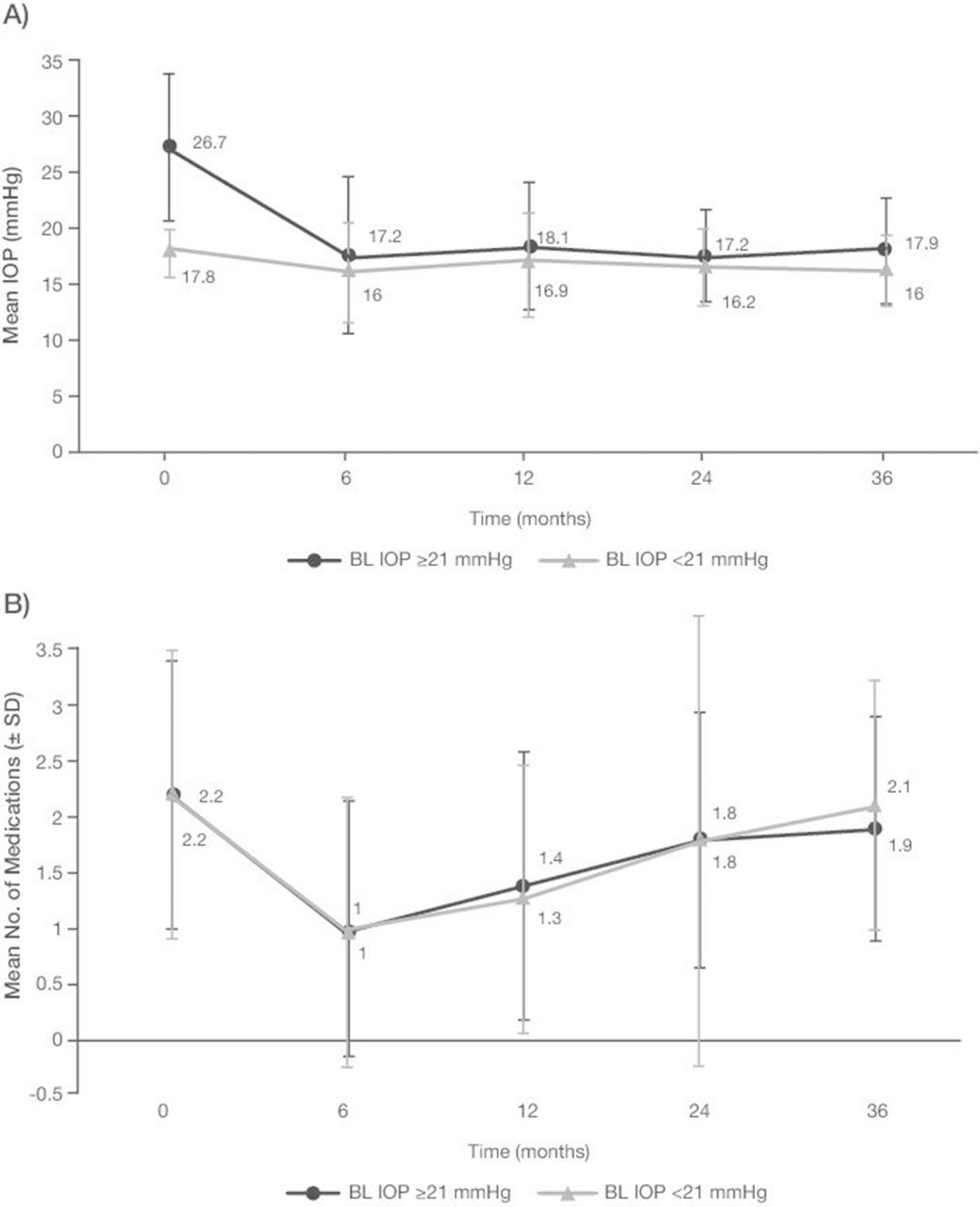
The efficacy population included the 224 eyes with known baseline IOP (one eye had no baseline IOP) that underwent standalone microstent implantation. The mean baseline IOP in these 224 eyes was 22.6±6.7 mm Hg (figure 2, table 3). At months 6, 12, 18, 24 and 36, mean IOP ranged from 16.6 to 17.5 mm Hg, representing mean IOP reductions of 4.4–5.1 mm Hg (15.8%–19.5%). The mean baseline number of IOP-lowering medications used in these eyes was 2.2±1.2 (figure 3A), with the mean numbers at months 6, 12, 18, 24 and 36 ranging from 1.0 to 2.0 (figure 3, table 3).
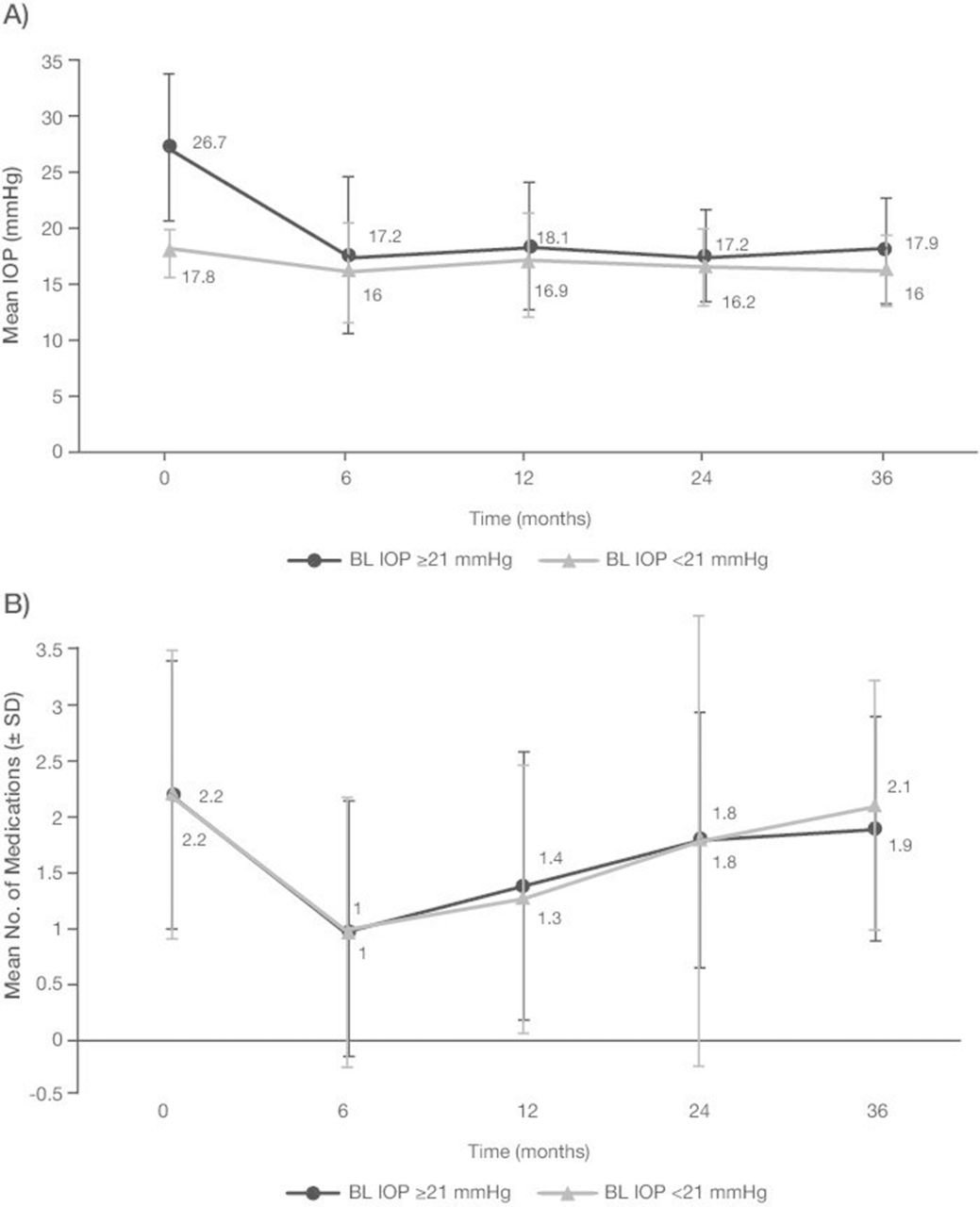
(A) Mean IOP and (B) mean glaucoma medication use over time following CyPass implantation alone in eyes with BL IOP ≥21 mm Hg and <21 mm Hg. BL, baseline; IOP, intraocular pressure.
{kind=link}
{kind=link}
{kind=link}
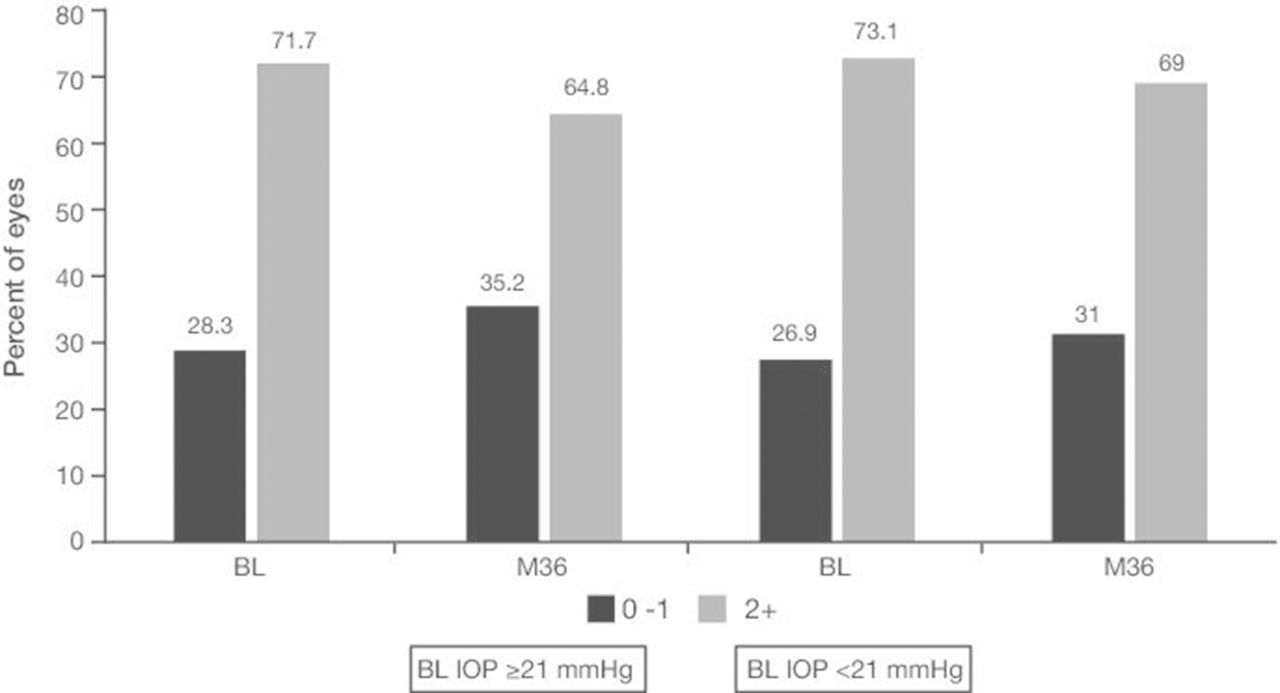
Percentages of eyes with BL IOP ≥21 mm Hg and <21 mm Hg using 0–1 and ≥2 ocular hypotensive medications at BL and 36 months after CyPass implantation. BL, baseline; IOP, intraocular pressure.
IOP and medication data at all time points
Of the 224 eyes that underwent standalone microstent implantation, 104 (46.4%) had baseline IOP <21 mm Hg, suggesting that they underwent surgery primarily to reduce medication use. The mean baseline IOP in these eyes was 17.8±2.3 mm Hg (figure 2, table 3). At months 6, 12, 18, 24 and 36, mean IOP ranged from 16.0 to 16.9 mm Hg, representing mean IOP reductions of 0.6–1.8 mm Hg (2.2%–8.7%). The mean baseline number of IOP-lowering medications used in these eyes was 2.2±1.3, with the mean numbers at months 6, 12, 18, 24 and 36 being 1.0–2.1 (figure 3, table 3). Of the 58 eyes in this group followed for the full 3 years, 16 (28%) achieved a >20% IOP reduction at 3 years while using the same number or fewer medications.
The other 120 eyes that underwent standalone microstent implantation had a baseline IOP >21 mm Hg, suggesting that they underwent surgery primarily to reduce IOP. These eyes had a mean baseline IOP of 26.7±6.5 mm Hg (figure 3, table 3). At months 6, 12, 18, 24 and 36, their mean IOP ranged from 17.2 to 18.1 mm Hg, representing mean IOP reductions of 7.8–8.6 mm Hg (28.3%–31.8%). The mean baseline number of IOP-lowering medications used in these eyes was 2.2±1.2, with the mean numbers at months 6, 12, 18, 24 and 36 being 1.0–1.9 (figure 3, table 3). Of the 54 eyes in this group followed for the full 3 years, 27 (50%) achieved a >20% IOP reduction at 3 years while using the same number or fewer medications.
The effectiveness of the microstent was similar for phakic and pseudophakic eyes. Table 4 shows the mean IOP, the proportion of eyes achieving a >20% IOP reduction, and medication usage at baseline and at 12, 24 and 36 months by preoperative lens status. Of 75 phakic eyes, 19 (25.3%) underwent subsequent cataract surgery, 16 within the first 12 months postoperatively.
Subgroup analysis of effectiveness data by preoperative lens status
Discussion
Implantation of the CyPass supraciliary microstent was generally safe and well-tolerated in these eyes, with no device-related sight-threatening complications. Although 31.6% of eyes required subsequent glaucoma procedures, this rate is consistent with reoperation rates following other MIGS procedures, including implantation of the iStent trabecular bypass (38%)7 and Trabectome trabecular ablation (27%).8
Standalone microstent implantation resulted in sustained 16%–20% reduction in IOP through 3 years of postoperative follow-up and reduced IOP-lowering medication use by an average of 0.5–1 medications through the first 12–18 months of follow-up. At month 36, mean IOP reduction was 4.5 mm Hg (16.9%), with subjects using slightly fewer medications than at baseline.
IOP reductions were greater in eyes with higher (≥21 mm Hg) than lower (<21 mm Hg) baseline IOP, while reductions in medication use were comparable in the two subgroups. IOP reductions in eyes with lower baseline IOP were modest, ranging from 2%–9%, with subjects using 0.5–1 fewer medications after 12–18 months. In eyes with higher baseline IOP, the IOP reductions were 25%–30% at all postoperative time points. These results compare favourably with those of a protocol-based, multicentre, single-arm study of standalone microstent implantation in eyes with medicated IOP >21 mm Hg.9 In that study, IOP at 12 months postoperatively was reduced 35%, with subjects using 0.8 fewer medications per eye. The magnitude of IOP reduction observed in the current study was greater than expected when adding a single IOP-lowering medication to prostaglandin monotherapy,10–12 and more consistent with the addition of a fixed combination of two medications to prostaglandin monotherapy.13 14 This IOP reduction was also consistent with those of other MIGS procedures performed as standalone surgery, including canal based approaches such as the iStent trabecular bypass15 and Trabectome trabecular ablation.16 17 MIGS devices targeting the subconjunctival space and forming a bleb are generally indicated for refractory glaucoma. It is therefore interesting to compare the 12-month outcomes for the ab interno Xen gel stent with the uncontrolled IOP cohort from the present study. Baseline IOP and medication usage were similar; mean medicated IOP was 25.1 mm Hg on an average of 3.5 medications for the gel stent and 26.7 mm Hg on 2.2 medications for the ≥21 mm Hg cohort in the present study. At 12 months (the duration of the gel stent study), mean changes from baseline in IOP were −9.1 mm Hg and −7.9 mm Hg for the gel stent and CyPass microstent, respectively.18 Our finding, that 50% of eyes with baseline IOP >21 mm Hg achieved a mean IOP reduction ≥20% on the same or fewer medications at 3 years, was clinically significant.
It is important to consider that, had they not been enrolled in this study, many of these eyes likely would have undergone traditional glaucoma surgery (ie, trabeculectomy or another filtering procedure). Forty-four per cent of the eyes enrolled for the standalone microstent procedure had a history of prior glaucoma surgery, 53% had preoperative IOP ≥21 mm Hg, and 72% were being treated with ≥2 ocular hypotensive medications. Despite the inclusion of eyes with more advanced disease, only 31.6% required additional glaucoma surgery over the 3-year follow-up period of this study.
The performance of cataract surgery was an anticipated event for some proportion of patients, given the possibility of pre-existing cataract at baseline and the 3-year duration of the study. Nineteen eyes underwent cataract surgery during the course of study participation, 16 during the first postoperative year and the remaining three between 12 and 24 months. This additional procedure may have contributed to some level of additional IOP reduction in this subgroup. However, patients undergoing cataract surgery were not excluded from the analysis as, in our opinion, the performance of cataract operations closely reflects real-world situations and supports the overall generalisability of the study outcomes.
As a registry study, CyCLE included some patients who were (and remain) outside the labelled indication of primary open angle glaucoma (POAG). Indeed, seven (3.9%) eyes enrolled in the standalone cohort had narrow angles. This subgroup showed no obvious differences in safety outcomes compared with the study cohort as a whole. One phakic eye with narrow angles experienced an IOP elevation >10 mm Hg above baseline; an incidence of 14% compared with 9% (20 eyes) in the entire group.
This study had several limitations, including those common to real-world studies. It did not include a control group. Moreover, the study protocol did not standardise patient selection beyond basic eligibility criteria, recommended but did not confirm adherence to the manufacturer’s recommended surgical technique, and did not specify postoperative care. These methodological differences can account for differences in outcomes when compared with more robust clinical trials. However, the results of these clinical trials may not be broadly generalisable to target patient populations likely to undergo these interventions. Clinical trials often have narrow eligibility criteria to ensure homogeneity of study subjects and may require multiple IOP measurements using a specified type of tonometer to more robustly estimate efficacy outcomes. In the real world, however, most clinical centres care for broadly heterogeneous populations, and IOP is measured using a variety of tonometers and is rarely the average of multiple measurements. Clinical trials also tend to enrol subjects with a narrower spectrum of disease severity than was included in this study. Our study is not intended to substitute for robust clinical trial data but should rather be considered complementary to such studies.
In conclusion, this real-world study found that implantation of the CyPass supraciliary microstent, performed as a standalone procedure, safely and effectively lowered IOP in eyes with OAG. This device resulted in greater reductions in IOP in eyes with baseline IOP >21 mm Hg than in those with baseline IOP <21 mm Hg. Adverse event rates and IOP reductions were consistent with those reported for other MIGS procedures.
References
Footnotes
Contributors Substantive intellectual contributions to the content of this manuscript were made by the authors in the following areas. SwG, SaG, EA and TI: drafting, critical revision and final approval. JG-F, HBD and FJM-N: critical revision and final approval.
Funding This study was funded by Alcon Research, Ltd. BelMed Professional Resources, Inc. provided editorial support, which was contracted and funded by Alcon.
Competing interests TI reports equity interest and compensation from Transcend Medical. All other authors report no conflicts of interest with the work reported here.
Patient consent Obtained.
Ethics approval IRB of all participating institutions.
Provenance and peer review Not commissioned; externally peer reviewed.