Article Text

Abstract
Objective This validation study investigates the treatment of cornea organ culture medium (Modified Eagle Medium, Biochrom GmbH, Berlin, Germany) with RESEP, a new medical device for antibiotics removal, before microbiological testing with BACTEC TM blood culture bottles.
Methods and analysis 10–100 colony forming units of Staphylococcus aureus, Pseudomonas aeruginosa, Candida albicans, Bacillus subtillis, Aspergillus brasiliensis, Clostridium sporogenes, Enterobacter cloacae and Staphylococcus epidermidis were inoculated in 9mL of cornea organ culture medium. In group A, the medium was withdrawn with RESEP and treated for 20 min at room temperature, and then inoculated in BACTEC Plus Aerobic/F/Anaerobic/F blood culture bottles. In group B, the medium, spiked by the inoculation of microorganism, was injected directly. For each strain, a growth control was performed, by direct inoculation of the microorganisms in BACTECTMvials (positive control). All samples were incubated in the automated BACTECTMblood culture system at 36°C ±1°C for maximum of 14 days or until a positive reading. The elimination of antibiotics from the medium by RESEP was determined by high-performance liqiud chromatography.
Results After 20 min of RESEP treatment, 100% (n=9) of streptomycin, 100% (n=9) of amphotericin B and 99.7% (n=9) of penicillin G were eliminated. In group A , all microorganisms were detected within 3 days of incubation with a sensitivity of 100% (n=99) and showed no significant delay compared with the positive controls. In group B, the overall sensitivity was 67.9% (n=96) with a significant delay until detection of microbial growth for all tested microorganisms except for A. brasiliensis.
Conlclusion The use of RESEP to eliminate the antibiotics from cornea organ culture medium increases the sensitivity of the microbiological testing with BACTECTMPlus blood culture bottles significantly and fulfils the requirements of the European Pharmacopoeia method suitability test.
- microbiology
- eye (tissue) banking
- cornea
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The use of resins contained in blood culture bottles for microbiological testing of cornea culture medium is an established gold standard. Nevertheless, the antibiotics in the medium can cause false negative test results, what might be a risk of infection for the recipient of the corneal graft.
What are the new findings?
This study shows that an additional treatment of the cornea organ culture medium with the RESEP device to further remove antimicrobials from the medium increases the sensitivity of microbiological testing up to 100%.
How might these results change the focus of research or clinical practice?
The demonstrated method of microbiological testing of cornea organ culture medium using an additional resin treatment can easily be implemented in the routine of an eye bank. We believe that it improves the established gold standrad of microbiological testing with blood culture bottles.
Introduction
Human donor corneas are one of the most commonly transplanted tissue worldwide and different corneal transplantation techniques are now well established as routine surgical procedures.1 2
Even though the risk of endophthalmitis and infectious keratits is low in the recipient, it remains a serious complication in keratoplasty.3–7 Consequently, the absence of microbial contamination of the graft is one of the necessary conditions for establishing cornea suitability for transplantation. This lies in the responsibility of the eye bank. It is a fact that most donor corneas bear microbial colonisation or contamination at the time of retrieval.8 9 Therefore, disinfection with povidone–iodine solution, usually performed prior to corneal excision, and storage in a medium containing antimycotics and antibiotics in order to control microbial growth are necessary.
The presence of antibiotics in the cornea storage media is a major challenge for their microbiological testing as these substances could inhibit microbial growth and then lead to false negative (FN) results with possible subsequent devastating clinical effects on the tissue recipients.
Each eye bank should select and validate an appropriate method for microbiological testing of the cornea storage media in order to guarantee the reliability of the microbiological result. Our eye bank performs the microbiological testing of the cornea organ culture medium (CM) with the automated BACTECTM Blood Culture System and BACTECTM Plus Aerobic/F and Anaerobic/F culture vials (Becton, Dickinson and Company, Franklin Lakes, New Jersey, USA). This blood culture system, which is widely used by European eye banks, contains resins in the growth media to inactivate antibiotics. The system is specifically designed and validated by the manufacturer for use with patient blood samples, which contain rather low concentrations of antibiotics. Using other samples containing high concentrations of antibiotics could lead to FN results, as antibiotics elimination is incomplete.10–12 Therefore, the system also needs to be validated for samples other than blood. Previous studies evaluated the suitability of automated blood culture systems for microbiological testing of cornea storage media.10–15 We have previously investigated the microbiological testing of our cornea organ CM using BACTECTM and demonstrated its limitations.12
In the presented study, we investigate an innovative approach for eliminating antibiotics from samples for microbiological testing using RESEP (AL.CHI.MI.A. S.r.l., Ponte San Nicolò – Padova, Italy). RESEP is an in vitro diagnostic medical device that contains resins for removal of antibiotics from liquid samples. The study employs the method suitability test described in the European Pharmacopoeia (EP) chapter 2.6.1 as well as the method validation in chapter 2.6.27.16
Materials and methods
Preparation of microorganisms and inocula
The EP reference strains: Pseudomonas aeruginosa (PA) (ATCC 9027), Candida albicans (CA) (ATCC 10231), Aspergillus brasiliensis (AB) (ATCC 16404), Staphylococcus aureus (SA) (ATCC 6538), Clostridium sporogenes (CS) (ATCC 19404) and Bacillus subtilis (BS) (ATCC 6633), and the strains: Staphylococcus epidermidis (SE) (ATCC 12228) and Enterobacter cloacae (EC) were obtained from the American type culture collection (ATCC, Manassas, Virginia, USA) and from Labor Berlin – Charité Vivantes GmbH (Berlin, Germany).
For inocula preparation, lyophilised pellets (PA, CA, AB) or fresh colonies isolated on blood agar plates (SA, CS, SE, EC), were subcultured under optimal growth conditions, according to the manufacturer’s instructions, and their concentrations were measured according to the McFarland turbidity standards. Serial dilutions were performed to obtain an inoculum concentration of 10–100 colony-forming units (CFU) in 1 mL of Tryptone Soya Broth (TSB) (OXOID Deutschland GmbH, Wese, Germany). Only for AB, the inoculum was prepared directly from the lyophilised pellet without previous subculture. Inocula were then plated on Columbia-blood-agar plates (OXOID Deutschland GmbH, Wese, Germany), incubated at 35°C, and CFU were counted after 48 hours in order to determine the actual microbial concentration of each inoculum.
From each microbial strain, 10–100 CFU were inoculated in 9 mL of cornea organ CM (Biochrom GmbH, Berlin, Germany), which contains 2% of Australian fetal calf serum, penicillin G 62.5 µg/mL, streptomycin 100 µg/mL and amphotericin B 2.5 µg/mL in Modified Eagle’s Medium (MEM) with Earl’s salt.
For each tested condition, CM samples, positive and negative controls were assessed at least in triplicate and repeated in three different experiments (n=9).
Group A
The spiked CM was gently withdrawn with RESEP, incubated at room temperature for 20 min under continuous stirring and finally injected into BACTECTM blood culture bottles. RESEP is a syringe-like, patented, CE-marked device containing a resin mixture to remove antibiotic residues from liquid samples before performing microbiological test. After treatment, the CM samples containing CS were injected in BACTEC Plus Anaerobic/F culture vials, and the samples containing AB, BS, CA, PA and SE in BACTEC Plus Aerobic/F culture vials. The samples containing SA were tested in both BACTEC Plus Anaerobic/F and Aerobic/F culture vials. Finally, the bottles were incubated in BACTEC 9120-FX System at 36°C±1°C until a positive reading or for at least 14 days. The time to detection of microbiological growth was automatically recorded by the BACTEC 9120-FX system. Each positive culture bottle was analysed for the presence of pure culture by subcultivation on blood agar plates, and the detected germs were identified by morphological analysis and mass spectrometry (MALDI-TOF MD, Bruker, Billerica, Massachusetts, USA).
Group B
In group B, the spiked CM samples were directly injected into the respective BACTEC Plus culture vials.
Positive controls (growth controls)
Inocula with 10–100 CFU in 1 mL TSB served as positive controls (growth control). CS inocula were directly injected in BACTEC Plus Anaerobic/F; AB, BS, CA, PA and SE inocula were injected in BACTEC Plus Aerobic/F culture vials. Also here SA inocula were assessed in both BACTEC Plus Aerobic/F and Anaerobic/F culture vials. All BACTEC bottles were subsequently incubated and processed as described for group A.
Negative controls
Nine millilitres of sterile TSB withdrawn in RESEP, incubated under continuous stirring at room temperature for 20 min, and then inoculated in BACTEC Plus Aerobic/F and BACTEC Plus Anaerobic/F culture vials, were used as negative control for group A. As negative controls for group B, a direct inoculation of 9 mL of TSB in BACTEC Plus Aerobic/F and BACTEC Plus Anaerobic/F Culture bottles was performed. All blood culture bottles were incubated in the BACTEC 9120-FX system as described before.
UHPLC determination of antibiotic and antimycotic residues
The antibiotic and antimycotic content in the sterile CM, before and after treatment with RESEP, was determined by UltiMate 3000 Ultra High Liquid Chromatography (UHPLC) (Dionex, Sunnyvale, California, USA). Penicillin G and streptomycin sulfate concentration were determined using UHPLC column Poroshell 120 SB-C18 2.7 µm, 4.6×100 mm (Agilent, Santa Clara, California, USA), and amphotericin B concentration with UHPLC column ULTRA C18 3 µm 150×2.1 mm (Restek, Bellefonte, Pennsylvania, USA). For these measurements, CM was quickly thawed at 37°C in a water bath, 9 mL of CM were withdrawn with RESEP in triplicate, incubated under continuous stirring at room temperature for 10, 20, 30 and 60 min, and immediately processed and injected in UHPLC system.
Initial content and the content after 20 min of RESEP treatment were determined on three different CM batches.
Data analysis and statistics
For each group and each tested microbial strain, the percentage of positive BACTEC readings, the mean time to detection and standard errors of the means were calculated and represented by box plot generated by BoxPlotR web-tool, http://boxplot.tyerslab.com. For each microorganism, Fisher’s exact test was used to compare the number of positive BACTEC readings between the positive controls and groups A and B, respectively, in 2 by 2 contingency tables. The time to detection differences between groups were analysed by Kruskal-Wallis one-way analysis of variance by ranks and Dunn’s post hoc test for non-parametric pairwise multiple comparisons in independent groups. A p value <0.05 was considered statistically significant. In addition, results for microorganisms with differences >50% in sample size between groups (A, B and control) due to FN results were excluded from Kruskal-Wallis and Dunn’s analysis.
UHPLC peak areas for penicillin G, streptomycin sulfate and amphotericin B were compared with the standard area and mean concentration; SD and percentage of initial content were calculated.
The sensitivity in groups A and B was calculated as the true positive (TP) results divided by the TP plus FN result [(TP)/(TP +FN)] and expressed as a percentage. The specificity was calculated as the true negative (TN) results divided by the TN plus false positive (FP) results [(TN)/(TN +FP)] and expressed as a percentage.
Results
Removal of antibiotics from CM
The concentration of streptomycin sulfate, penicillin G and amphotericin B at different time intervals of RESEP treatment is reported in table 1. A removal of >99.9% (n=3) of initial streptomycin sulfate and 100.0% (n=3) of amphotericin B content was observed after 10 min of treatment with RESEP. 100% (n=9) of amphotericin B, 100.0% (n=9) of streptomycin sulfate and 99.7% (n=9) of penicillin G were removed after 20 min. A 99.9% (n=6) removal of penicillin G was obtained after 60 min.
Antibiotic concentration in the CM (µg/ml) after different RESEP treatment intervals
Detection of microbial growth by BACTEC
Table 2 shows the percentage of positive samples for each microbial strain and for each group detected by BACTEC 9120-FX System on the spiked CM samples. As in the positive controls, the treatment of CM with RESEP (group A) resulted in 100.0% (n=99) detection of microbial growth for all tested strains. These two groups were statistically equivalent according to Fisher’s exact test. In group B, an overall sensitivity of 67.9% (n=96) was observed: 100.0% microbial growth was observed only for AB (n=9), CS (n=9) and PA (n=12) while significant percentages of FN results (p<0.05, Fisher’s exact test between group B and positive controls) were observed for BS (16.67%, n=12), CA (50%, n=12) and SA (33%, n=12 in BACTECTM Plus Aerobic/F vials and 83.33% n=12 in BACTECTM Plus Anaerobic/F vials). All negative control samples showed no positive reading after 14 days of incubation in the BACTEC system.
Percentage of samples detected positive by BACTEC 9120-FX System out of the total number of inoculated samples for each strain and for each group (overall sensitivity)
Time to detection
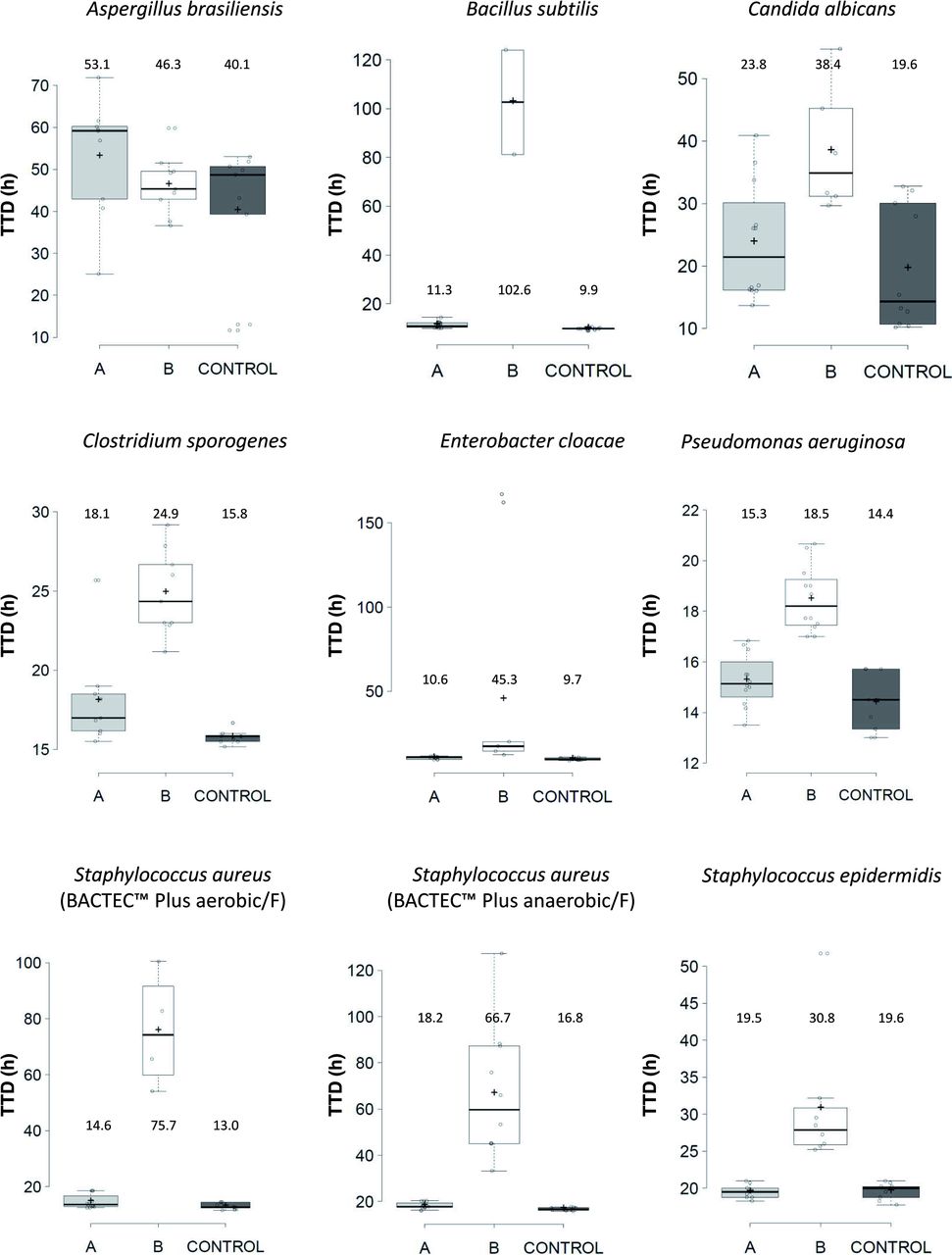
The results for time to detection observed for each strain in group A, B and the positive controls are reported in figure 1.
{kind=link}
Box plots show the data distribution of the TTD values of microbial growth recorded by BACTECTM 9120-FX System for group A, group B and positive control. The reported values correspond to mean TTD values (+). TTD, time to detection.
According to Kruskal-Wallis and Dunn’s tests, the time to detection was significantly shorter (p<0.01) in group A (with RESEP treatment) compared with group B (without RESEP treatment) for PA, CS, SA and SE, whereas it was not statistically different between the two groups for AB. The results for BS, CA and SA were excluded from the statistical analysis due to a difference in sample size >50.0% between groups.
For all tested microorganisms, the time to detection observed in group A was not statistically different from the positive controls. This was different in group B, where we found a statistically significant difference compared with the positive controls for all strains except AB (p<0.01).
Method sensitivity and specificity
The average sensitivity in group A resulted to be 100.0%. In contrast, we found a lower sensitivity of 67.9%±11.0% in group B. The specificity was 100.0% in both groups.
Discussion
Multiple validation studies on sterility testing of tissue and cell processing products with automated blood culture systems including resin-containing bottles have been published,17–20 all of which show no specific need for antibiotic elimination from samples. However, the efficacy of neutralisation depends on the type and concentration of antimicrobials. Spaargen et al showed that the antibiotic activity decreased by 80.0% to 90.0% after 2 hours of incubation in resin-containing BACTECTM Plus bottles.21 Other authors22 showed that some of the investigated antibiotics were only partially or not at all neutralised in BACTECTM Plus bottles. In agreement with that, relevant limitations for the sterility testing of cornea organ CM with blood culture bottles were shown.12 The use of an automated blood culture bottle system is the gold standard for microbiological testing of corneal organ culture media in Europe.10–14 We have investigated the effect of an additional treatment of a medium with RESEP on the sensitivity of microbial detection. In group A, with additional resin treatment, the sensitivity was 100.0% with no statistically significant difference of the time to detection of microbial growth compared with the positive controls. In group B, where the microbial spiked cornea CM was given directly to the blood culture bottles, the overall sensitivity was 67.9% with a significant delay of the time to detection of microbial growth for all tested microorganisms except for AB. In accordance with previous results using RESEP tube for removal of antibiotics, we found a fast and high absorbance of penicillin G, streptomycin and amphotericin B within 20 min.23 Within 10 min after RESEP treatment, both streptomycin and amphotericin B were totally eliminated and only traces of penicillin were confirmed by UHPLC time-course studies. We selected 20 min of RESEP incubation at room temperature as optimal treatment for both elimination of antimicrobials from CM and compatibility with the routine procedures in the cornea bank.
We found no inhibitory effect of microbial growth by the treatment with RESEP, as shown in a previous investigation of Lindsey and Riely in which resins did not trap, inhibit or kill bacteria.24
Schroeter et al showed a reliable detection of PA, CS, CA and AB in BACTECTM Plus blood culture bottles with 10 mL of the same cornea organ CM and a limited detection of BS.12 The higher detection rate of that study compared with our group B might be due to the inoculation of the microorganisms into the blood culture bottles after the medium was already added, thus diluting them. We inoculated the microorganisms into the CM directly before transferring them to the blood culture bottles to simulate a contaminated CM.
Thomasen et al examined a protocol for microbiological testing of corneal CM, using BacT/Alert resin containing blood culture bottles and penicillinase for antibiotic degradation.14 They found no significant difference in time to detection between spiked samples and the positive controls except for BS.14 In contrast to our method, Thomasen et al added the test microorganisms after 1 hour of preincubation of the CM together with the penicillinase and used only 5 mL medium.14 Therefore, and looking at their results for BS, we believe that an additional resin treatment of the cornea CM may increase the test sensitivity more than an enzymatic degradation.
We used the same resin containing blood culture bottles for group A and B for better comparison. Therefore, we cannot conclude whether the resins in the blood culture bottles are necessary to obtain the sensitivity shown after treatment with RESEP. Additional tests with blood culture bottles without resins and specific clinical microbial isolates should be performed in order to further characterise the sensitivity of the microbiological testing system using RESEP. Recently, Mistò et al reported on the use of RESEP for removal of antimicrobial agents from corneal storage and transport media (CARRY-C and TISSUE-C, AL.CHI.MI.A. S.r.l.) before microbial growth was read by an different test system, an automated light scattering culture system (HB and L, Alifax, Polverara, Italy) within 48 hours. They also showed that the sensitivity could be increased to 100% doing that.25
From the presented data, we conclude that the CM sample treatment with RESEP increases the sensitivity of the microbiological testing with BACTECTM Plus blood culture bottles in compliance with EP method suitability test and with that reduces the risk of FN test results.
References
Footnotes
Contributors AP: had the idea. ZS, LG, CG and JDT: planned and designed the study. ZS, LG and CG: performed the experiments. ZS, LG, CG, JDT and JS: analysed and interpreted the data. ZS, LG, JDT and JS: drafted the manuscript. ZS: wrote the manuscript. JDT, AP and JS: critically revised the manuscript. ZS: submitted the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests LG, CG and JDT are employed by the company which was involved in the development of the medical device discussed in the present paper.
Provenance and peer review Not commissioned; externally peer reviewed.