Article Text

Abstract
Limbal stem cell damage after chemical injury, autoimmune disorders or iatrogenic trauma leads to corneal conjunctivalisation with new vessel formation, epithelium instability and visual loss. Limbal stem cell transplantation includes reconstructive surgical procedures to restore a corneal epithelium. The recognised options are: conjunctival limbal autograft, in which stem cells are taken from the patient’s healthy eye; conjunctival limbal allograft, in which stem cells are taken from a living, related or dead donor and the keratolimbal allograft. Each of these procedures has some drawbacks; in particular, the conjunctival limbal autograft needs a relatively healthy fellow eye and needs a relatively large amount of donor tissue from the healthy eye (about one-third of the healthy limbal stem cell tissue) with potential risks to the donor eye. In the case of keratolimbal allograft transplants, the recipient needs an immunosuppressive treatment to reduce the risk of rejection with the associate possible side effects. More modern treatment options are reviewed. Cultivated oral mucosa epithelial transplantation success rate can vary between 50% and 70% at 3–4 years of follow-up. Simple limbal epithelial transplantation results show a success rate from 75.2% to 83.8% after 1 year of follow-up. Inclusion criteria for autologous cultivated limbal epithelial transplantation as approved by the National Institute of Health and Care Excellence are also shown in this paper. On the basis of these more contemporary treatment options, a stepladder approach to evaluate which procedure is most appropriate and personalised to the patient’s conditions is proposed.
- ocular surface
- cornea
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The corneal epithelium is renewed by stem cells located at the limbus. A loss or deficient function of these so-called limbal stem cells results in the disease of limbal stem cell deficiency (LSCD). This is characterised by persistent epithelial defects and conjunctivalisation of the corneal surface. Limbal stem cell deficiency is a rare disease that results in both visual impairment and chronic ocular surface pain.
Although there have been several advances in the field in the last 20–30 years, the management of LSCD remains a challenge. These advances include whole tissue transplantation of the limbal epithelium (autografts and allografts); the developments of cultivated limbal epithelial transplantation (CLET) and cultivated oral mucosal epithelial transplantation (COMET) and simple limbal epithelial transplantation (SLET).
Due to the availability of several different management options for LSCD and as a result of recent guidance from the National Institute for Health and Care Excellence (NICE), it is important to develop a treatment algorithm for LSCD. This forms the main aim of this review. Treatment options will be discussed in the context of their availability and efficacy.
Key milestones in limbal stem cell biology
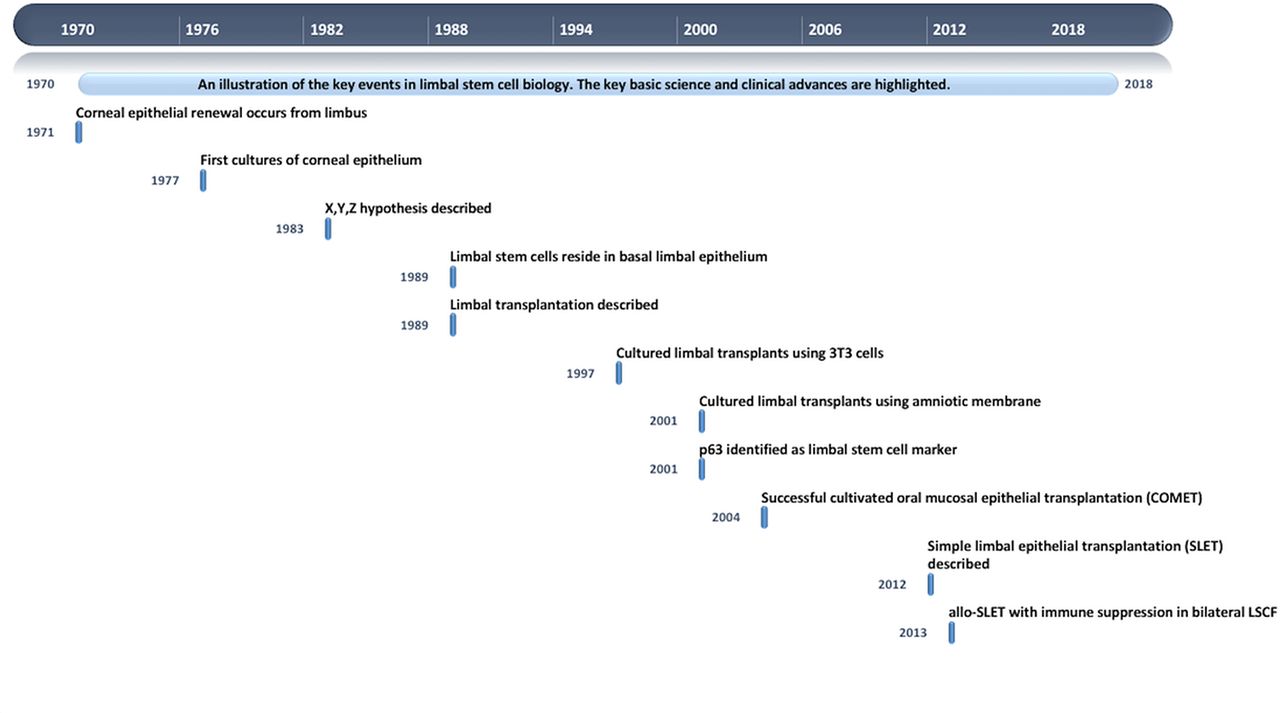
The current management of patients with LSCD results from approximately five decades of research associated with therapeutic advancement. There are several key milestones that will be highlighted (figure 1).1 Davanger and Evensen2 in 1971, by studying guinea pig eyes, were the first to propose that the limbus was the source of corneal epithelial regeneration. Later on, in 1977, Sun and Green3 were the first to successfully culture corneal epithelial cells by co-culturing them with mitotically inactivated 3T3 mouse embryonic fibroblasts. Prior to this, corneal epithelial cultures could not be established as contaminating corneal fibroblasts outgrew the epithelial cells.

Illustration of the key events in limbal stem cell biology. This figure shows the most important advances in limbal stem cell biology in a schematic way.
In 1983, Thoft and Friend4 proposed the X, Y, Z hypothesis for corneal epithelial maintenance. The two main principles of this hypothesis are that: (1) the corneal epithelial structure maintains homeostasis by equal replacement of cells that are shed from the corneal surface and (2) the corneal epithelial cell replacement begins from the basal epithelial layer of the corneal periphery. Cotsarelis and his co-workers5 in 1989, using radiolabelling studies in mice, confirmed the former hypothesis. They showed for the first time that cells within the basal layer of the limbal epithelium were the source for corneal epithelial cells. These corneal epithelial stem cells have since become commonly known as limbal stem cells due to their anatomic location.
In 1989, Kenyon and Tseng6 were the first to show that LSCD could be reversed by the transplantation of healthy limbal tissue. This was initially described as an autograft for unilateral disease but allografts from living related donors and from cadaveric sources were subsequently performed with some success.7 Utilising culture methods for corneal epithelium developed in the 1970s, Pellegrini and co-workers8 in 1997 were the first to show that smaller amounts of donor limbal epithelium could be co-cultured with 3T3 fibroblasts and then this cultivated expanded limbal epithelium could be transplanted successfully in patients with unilateral LSCD (auto-CLET). Subsequent to this, human amniotic membrane culture methods avoiding 3T3 fibroblasts have been developed and successfully used to treat patients with LSCD and allo-CLET procedures have been successfully used to treat bilateral LSCD.9–11
In 2004, Nakamura and co-workers12 showed that cultured oral mucosal epithelium on human amniotic membrane could be used to successfully treat patients with LSCD. Due to the autologous nature of this, immune suppression was not needed.
Finally, in 2012, Sangwan and co-workers13 showed that the direct transplantation of small amounts of autologous donor limbal epithelium could be used to successfully treat unilateral LSCD. This new technique called SLET overcomes the expense and hurdles involved in culturing epithelial cells for transplantation as a result of the need for specially developed clean laboratories and the regulatory approvals required. In 2013, the same team showed that allo-SLET with immune suppression was also possible in bilateral LSCD.14
Each of the above milestones is key to how we are able to manage LSCD today. The aforementioned clinical options is a viable therapeutic consideration in patients today depending on their individual circumstances and underlying disease process.
Principles of management
There are many causes of LSCD, including genetic and acquired causes. Genetic causes include aniridia-related keratopathy (ARK) caused by PAX6 mutations and ectodermal dysplasias caused by p63 mutations. Acquired causes are formed by the 3 I’s: injury such as chemical and thermal burns; inflammation such as mucous membrane pemphigoid, Stevens Johnson syndrome and graft versus host disease and iatrogenic causes such as limbal surgery for ocular surface tumours, topical chemotherapy (mitomycin C) and radiation. Knowledge of aetiology is important in determining the management pathway as will be discussed below.
There are still several limitations that need to be mentioned. First of all, there are not clear criteria for the definition of LSCD. Limitations in diagnosing LSCD with current techniques are evident too. Indeed, there is currently no unifying limbal stem cell marker available that could help to diagnose and grade the LSCD in a reliable and objective way. Consequently, it is difficult to know the number of limbal stem cells that need to be transplanted in every single case in order to achieve a successful outcome in the long term.
Limbal stem cell deficiency treatment is usually complex and varies a lot among patients. Therefore, although it is difficult to summarise the treatment, in our view, there are at least five main principles in the management of LSCD:
Understanding and controlling inflammation: it is important that ocular surface inflammation is controlled prior to any surgical management, using either topical or systemic immune suppression. After an acute chemical burn, inflammation can take as long as 12–18 months to control. Patients with mucous membrane pemphigoid will require systemic immune suppression.
Correcting lid malposition and fornix adhesions: these are important factors that contribute to ocular surface trauma and inflammation that exacerbate the disease process and prevent successful ocular surface reconstruction.15 These therefore need to be corrected in the first instance, prior to any surgical procedure for the LSCD.
Managing dry eye disease: LSCD is not uncommonly associated with tear film abnormalities. This can be as a result of obstruction of lacrimal duct outflow such as in mucous membrane pemphigoid; loss of goblet cells such as in Stevens Johnson syndrome or meibomian gland dysfunction resulting from any cicatrising conjunctivitis. These abnormalities need to be improved as much as possible prior to consideration of any ocular surface reconstructive procedure. Surgical measures such as punctal occlusion and permanent partial tarsorrhaphies may also be needed to achieve this.
Partial versus total LSCD: one of the main goals of ocular surface reconstruction is to improve vision. In both partial and total involvement of the limbus and therefore corneal surface, central corneal involvement is an important reason for surgical reconstruction. There are many patients with partial LSCD who do not have central corneal involvement and some patients with total LSCD with central corneal sparing who do not need ocular surface reconstruction procedures. It must also be noted that in partial LSCD, healthy portions of the limbus can be utilised for surgical reconstructive methods (either auto-CLET or auto-SLET).
Unilateral versus bilateral LSCD: knowledge of aetiology in LSCD is important in determining the surgical options, mainly whether autograft or allograft procedures should be employed. In unilateral disease, most commonly in injurious or iatrogenic causes of LSCD, an autograft procedure would be employed. In bilateral disease, such as genetic and inflammatory diseases, COMET or allograft procedures would be utilised.
Following the principles above in managing each patient individually enables successful determination of which surgical ocular surface reconstructive procedure to employ.
As whole tissue limbal epithelial transplantation and CLET have been reviewed numerous times previously, remaining aspects of this manuscript will discuss further surgical advances within the field.
Cultivated oral mucosal epithelial transplant
A significant proportion of patients with LSCD have bilateral disease. In these cases, there is most often no area of healthy limbus in either eye to use a source of donor limbal stem cells. Therefore, limbal allograft procedures (allogeneic whole limbal tissue grafting, allo-CLET or allo-SLET) become the only valid treatment options. However, these procedures are accompanied by the risk of rejection and the requirement of potent systemic immune suppression. The rationale of COMET is to overcome these drawbacks by means of using autologous mucosal epithelium of non-ocular surface origin.
Early studies
The use of oral mucosa for ocular surface reconstruction was first attempted in 1963 by Ballen and co-workers.16 These oral mucosal grafts included both epithelium and subepithelial tissues and developed early fibrosis and intense corneal vascularisation. Later on, in 1986, Gipson and co-workers17 used oral epithelium (freed of connective tissue to avoid vascularisation), but they found that these epithelial cells could not survive in central avascular areas of the cornea.
The development of COMET
Taking into consideration the issues of these previous studies, Nakamura and co-workers,18 developed a method to culture rabbit oral mucosal epithelial cells on amniotic membrane as a carrier. Small oral biopsies (approximately 2–3 mm) were obtained from the oral cavity. The biopsy specimens were then incubated with enzymatic reagents to separate epithelial cells from the underlying connective tissue. The resultant single-cell suspensions of oral mucosal epithelial cells were co-cultured for 2–3 weeks on a denuded amniotic membrane carrier, with inactivated 3T3 fibroblasts. Towards the end of the culture period, an air-lifting technique was used to facilitate epithelial differentiation and stratification. The resulting cultured grafts were transplanted in rabbit studies. The eight rabbit corneas studied were all clear and epithelialised 10 days after surgery. The oral mucosal epithelial cells showed 5–6 layers of stratification and appeared very similar to in vivo normal corneal epithelium. The authors detected the presence of non-keratinised, mucosal-specific keratins 4, keratin 13, and importantly corneal epithelial-specific keratin 3, whereas, keratinisation-related keratin 1 or keratin 10 was not detected. Epithelial cells were very similar in appearance to those of normal corneal epithelium, had numerous desmosomes and were attached to a basement membrane with hemidesmosomes. These phenotypic characteristics were also confirmed in other studies later on.19 20
Clinical results of COMET
Re-establishment of a stable and transparent corneal epithelium, regression of corneal conjunctivalisation/vascularisation and resolution of persistent epithelial defects (PEDs) have been considered as criteria for clinical success in LSCD. In a short-term follow-up study, 10 eyes with PED due to LSCD from several ocular surface chronic conditions were transplanted with COMET. At the fourth postoperative week, seven eyes (70%) had achieved complete epithelialisation and three eyes showed a small epithelial defect. At the 24th postoperative week, PED had improved in all patients except one patient who did not undergo the 24th week visit.21 In another study with longer mean follow-up of 25.5 months, 40 eyes underwent COMET surgery. Corneal surface stability revealed an early decline in transplanted COMET over the first 6 months, remaining stable thereafter (1 year: 64.8%; 2 years: 59% and 3 years: 53.1%). Complications like melting, perforation or infectious keratitis occurred in 10 eyes, and all of these eyes had PED despite the COMET treatment.22 Nakamura and colleagues23 reported better results in 19 eyes after a longer mean follow-up of 55 months. All of the cases demonstrated total re-epithelialisation of the corneal surface within 2–7 days after surgery. All eyes manifested various degrees of postoperative corneal neovascularisation, but it gradually abated and its activity was stable at 6 months after surgery. The overall success rate, as measured by the improvement of visual acuity, was 53%. Other authors reported similar outcomes in 20 eyes with a clinical success (defined as stable ocular surface) rate at 4 years of 70.5%. Best corrected visual acuity improved in 70% of the eyes.24
Simple limbal epithelial transplantation
SLET is a novel surgical technique of in vivo expansion of limbal epithelial cells first described in 2012 by Sangwan and co-workers.13 It combines the advantages of conjunctival-limbal autograft (CLAU) and CLET, while addressing the limitations of both these earlier techniques. SLET is a single-stage, easily affordable procedure which obviates the need of specialist laboratory support for ex-vivo cultivation of limbal epithelial cells while retaining the benefit of CLET by taking smaller amounts of donor tissue and minimising any risks to the donor eye. Moreover, SLET may be safely repeated as most of the donor limbus is left undisturbed, and can be offered virtually anywhere by a trained corneal specialist.
The technique
In brief, the surgical technique is similar to that of CLET for harvesting the limbal biopsy (2 mm by 2 mm) usually from the superior limbus of the contralateral donor eye. The recipient eye is prepared as for all ocular surface reconstruction procedures for LSCD by performing a 360-degree peritomy followed by removal of the conjunctivalised fibrovascular pannus covering the cornea. Human amniotic membrane is then secured over the bared corneal surface with fibrin glue. The donor tissue is subsequently cut into 8–10 small pieces and these limbal transplants are fixed on the amniotic membrane using fibrin glue, epithelial side up, in a circular fashion sparing the visual axis.
Clinical results of auto-SLET
In their original case series, Sangwan and co-workers reported a completely epithelialised, avascular and stable epithelium within 6 weeks of auto-SLET that was maintained in all six patients at a mean follow-up of 9 months. In addition, there was an improvement in visual acuity in 66.6% of eyes without any donor site complications.13 Subsequent to the original description of autologous SLET, a few more favourable results were reported in individual case reports25–29 and small case series30–33 for unilateral LSCD secondary to severe ocular surface burns, mostly derived from the centre where the technique originated. Validation of these initial results was achieved by means of two large case series of auto-SLET for unilateral chemical and thermal burns which included 125 eyes from a single centre34 and 68 eyes from multiple centres,35 respectively. At a median postoperative follow-up of 1.5 years, reversal of ocular surface failure and a two-line improvement in visual acuity were seen in 76% and 75.2% of eyes studied by Basu and co-workers. Similarly, multicentre results presented by Vazirani and co-workers showed a successful outcome in 83.8% at a median follow-up of 12 months35. The presence of symblepharon, simultaneous keratoplasty, acid injury and postoperative loss of SLET transplants were associated with a significant risk of failure of SLET.34 35 Clinical success rates for auto-SLET are therefore broadly similar to those of previous corneal surface reconstruction techniques which range up to 87% for CLAU36 and 76% for auto-CLET.37
Clinical results of allo-SLET
In cases of bilateral LSCD, the patient can be offered allo-SLET from living donors or cadavers. Limbal stem cells from cadavers have been shown to possess a lower proliferative rate in vitro38 and a slower corneal epithelialisation rate in vivo.39 Thus, living donors may be more desirable for allo-SLET if possible. However, larger cadaveric limbal explants (≥0.5 mm2) may achieve a growth rate and proliferative potential similar to live tissue.40 41 Cadaveric SLET has been successfully used in a case of bilateral LSCD caused by an alkali burn to restore a stable corneal surface and improve vision. However, continued systemic immunosuppressive therapy was necessary to prevent allograft rejection.14 In contrast, a case of modified allo-SLET using larger donor tissue explants glued directly on the cornea followed by keratoplasty obtained a successful outcome without the need of any systemic immunosuppression.41 Recently, Iyer and co-workers performed allo-SLET from a cadaveric donor eye to achieve rapid epithelialisation in the early stages following severe ocular chemical injuries.42 Complete epithelialisation was seen in 94.11% (17/18) of eyes within a mean time of 22.5±9.14 days, and visual acuity improved in 72%. The authors argue that the aim of using allo-SLET at 1 month was to hasten epithelialisation, not for long-term survival. Thus, no systemic immunosuppression was used.
Commercially available auto-CLET and NICE guidance
Since 1997, Pellegrini and co-workers8 have been developing their auto-CLET product for regulatory approval and to make it commercially accessible to centres within the Europe. The product is the first stem cell-based product to receive European Medicines Agency (EMA) approval and is now commercially available as an orphan medicinal product within Europe for the treatment of LSCD from chemical burns. The aim of this therapy is to have a central production facility but to have several centres within Europe providing the treatment (a hub and spoke model). This has enabled CLET to emerge from a research-based setting to one that can be used readily within specialist corneal centres. As part of the regulatory approval process, the company is currently conducting a multicentre European phase III clinical trial.
Within the British healthcare system, NICE has issued guidance for the treatment of CLET with the EMA-approved commercially available auto-CLET product. This is based on the clinical results available to date and the cost implications of the culture process. In 2017, 20 years after CLET was first described, the NICE committee approved this licensed auto-CLET based on the following criteria:
It is only used to treat one eye.
The eye to be treated has moderate to severe LSCD after eye burns.
The eye to be treated has already had an attempted alternative reconstructive procedure (such as CLAU or auto-SLET).
Current treatment algorithm for LSCD
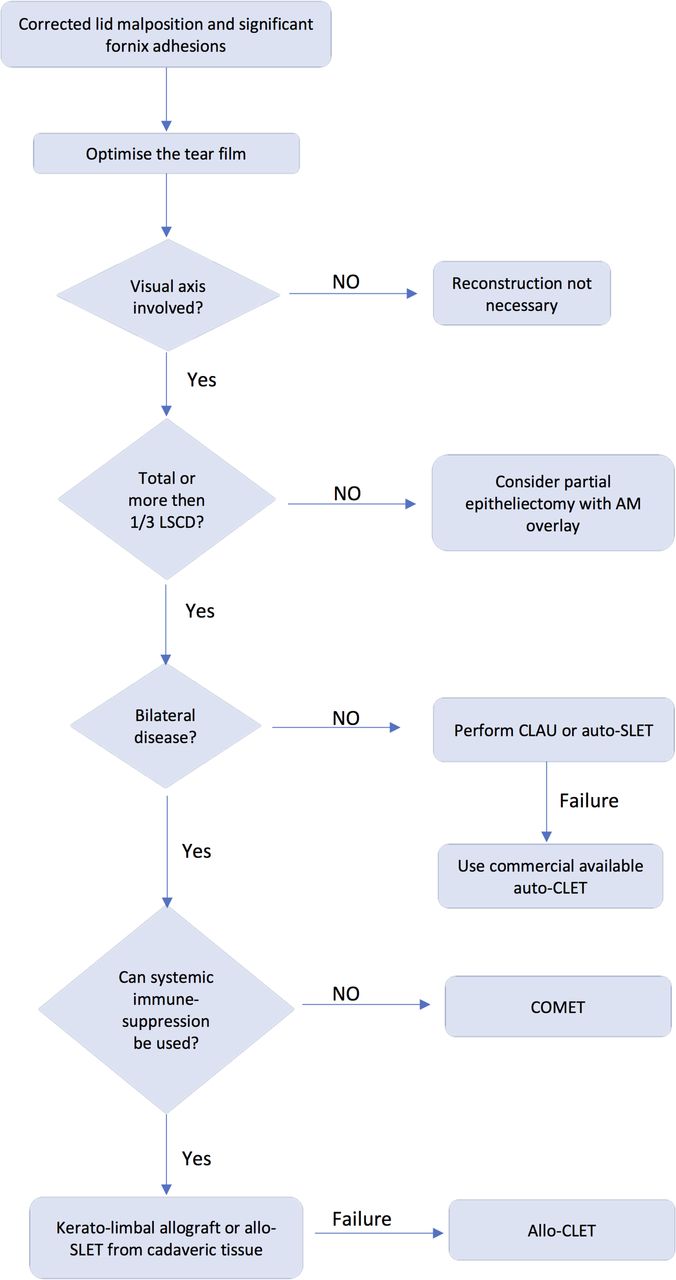
Based on the current treatment options available and the regulatory guidance, treatment algorithms for the management of LSCD within the UK have evolved. On this basis, our research group recommends the following 10 steps to be used in the decision-making process (figure 2):
Lid malposition and significant fornix adhesions should be corrected, as the presence of these is known to be significant for failure of ocular surface reconstructive procedures.
The tear film should be optimised as much as possible.
The first decision to take is whether the visual axis is involved. If it is not, then reconstruction is not necessary in most circumstances.
If the visual axis is involved, the extent of LSCD should be determined, that is, whether it is partial or total LSCD.
If LSCD is partial and involves approximately a quarter to a third of the limbus, then a partial epitheliectomy with amniotic membrane overlay should be considered.
If there is significant visual axis involving partial (more than a third of the limbus involved) or total LSCD, it is then important to know whether the disease is unilateral or bilateral. This enables determination of donor source for reconstructive techniques.
For unilateral disease, as per NICE guidance, CLAU or auto-SLET should be performed first. If these are not successful then commercially available auto-CLET should be performed.
For bilateral disease, it is important to know whether the patient can take and if they are willing to take systemic immune suppression. If the patient cannot be immune suppressed, then COMET should be performed.
For bilateral disease and if the patient can be immune suppressed, a whole tissue keratolimbal allograft or allo-SLET from cadaveric sources should be performed. If these fail and if it is available, allo-CLET should be performed.
Following any form of ocular surface reconstructive procedure, corneal surface normalisation is the main endpoint. Vision may or may not improve following such procedures. If there is involvement or scarring in deeper layers of the cornea, at approximately 12 months postocular surface reconstruction, a deep anterior lamellar keratoplasty or penetrating keratoplasty should be considered for visual rehabilitation. When a corneal graft is not an option due to previous failures, Boston keratoprosthesis could be considered in one eye, in those patients with bilateral involvement and very low vision with both eyes.

{kind=link}
{kind=link}
Proposed decision-making flow chart. This algorithm shows our research group recommendations based on our laboratory and clinical experience.
In conclusion, LSCD is a very complex condition as there are many different aetiologies, different grades of clinical involvement and it can be unilateral or bilateral. Furthermore, we still have evident limitations in its diagnosis and also monitoring the treatment outcome. On the other hand, this review shows that LSCD management has evolved very significantly in the last 20 years thanks to the development of new stem cell transplantation techniques that are definitely a source of hope for both patients and clinicians.
References
Footnotes
Contributors FA submitted the review. RFB, FA, SSZ and AG conducted the survey. SA planned the review and corrected and supervised it. RFB, FA, SSZ and AG wrote part of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.