Article Text

Abstract
Purpose To present the results of a community-based screening programme for diabetes, diabetic retinopathy (DR) and childhood blindness (CB) in District Hyderabad, Pakistan
Methods Prospective cross-sectional data collection from January 2014 to December 2015 of screening for diabetes, DR and CB in Hyderabad District. Female health workers were trained to identify high-risk (potential) patients for diabetes and childhood eye disorders to undertake preliminary screening and refer patients to basic health units. The patients were further assessed by medical officers with the support of qualified optometrist, after which they were referred to Sindh Institute of Ophthalmology and Visual Sciences, Hyderabad, Pakistan for management.
Results A total of 995 244 population was covered in this screening programme during which 2622 children (0–≤15 years) were screened for CB while 16 760 adult patients (>15 years) were screened for diabetes. Random blood glucose level of 3075 patients was >140 mg/dL. Out of these patients, 17% were diagnosed with DR. Refractive error (42%) was the most common cause of childhood visual impairment.
Conclusion The diabetic screening programme detected a high prevalence (17%) of retinopathy in patients with diabetes living in Hyderabad District. The most common cause of childhood visual impairment was refractive error (42%), which was successfully managed due to timely diagnosis. A large number of patients benefited from this community-based screening programme.
- child health (paediatrics)
- epidemiology
- public health
- retina
- vision
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
With a population of over 188 million, Pakistan has no approved screening programme for diabetic retinopathy or childhood blindness. Thus, putting a large number of vulnerable people at risk of threatening vision problems and even blindness. We found a high incidence of diabetic retinopathy and preventable causes of childhood visual impairment in Hyderabad District. This study has set an example of a workable mass screening programme which can be put into practice to identify and treat vision-threatening problems in Pakistan. On the basis of this study, a national screening programme can be initiated and implemented, therefore decreasing the load of blindness and reaching out to the poor people who can otherwise not get diagnosed or treated in a timely manner.
Introduction
Diabetes mellitus (DM) is one of the most common non-communicable diseases globally. It affects over 415 million adults worldwide and is projected to increase to 640 million by 2040.1 Drifting from stereotypical concepts that DM is more prevalent in developed countries, it is now evident that 80% of patients with diabetes live in low-income and middle-income countries.2 DM is the most common cause of legal blindness in the working age group (20–64 years) presenting as the greatest health challenge in 21st century.3
Prevalence of diabetes in Pakistan is about 7.89%,4 with over 5.2 million people affected in year 2000 while 14 million are estimated to be affected by 2030.5 A quarter of these have potential threat from sight-threatening diabetic retinopathy (DR). The incidence of blindness is 25 times higher in people with diabetes than in the general population. One per cent of avoidable blindness worldwide is due to DR.6
Recommended guidelines for the prevention of vision loss due to diabetes include early identification and well-managed DM, an annual eye examination to screen for DR in people with diabetes and treatment for DR by an ophthalmologist as required (laser treatment, vitreoretinal surgery or anti-vascular endothelial growth factor injections when available).7
Childhood blindness (CB) is an important and avoidable public health problem in developing countries. A recent estimate showed that 19 million children are visually impaired; refractive errors being the the most common cause found in 12 million of these, which can be easily diagnosed and treated.8 Irreversible blindness made up 4% of these causes, which will have significant impact on the psychological and personal development of these children.6
There are four main components of healthcare system in Pakistan namely;
Community level—this is covered by female health workers (LHWs) who are responsible to offer preventive awareness and provide first aid in case of emergencies.
Primary level—at this level, basic health units (BHUs) and rural health centres are present across the country, where primary health services are offered. Majority of these centres are maned with medical doctors.
Secondary level—at this level, all specialties are available which treat referred cases from primary level and also accept walk in patients.
Tertiary level—these are teaching-level hospitals offering specialised services. The tertiary level not only treats the complicated cases but also undertakes teaching and training to graduate and postgraduates levels.
In Pakistan, the healthcare delivery system suffers at all levels due to economic burdens on the country in general and in the health sector in particular. The tertiary level has somehow managed to take the impact as it is well equipped with trained personnel and facilities. But it is the district level primary and secondary levels that suffer from severe administrative, managerial flaws in addition to lack of trained individuals. This has led the population in these areas to be deprived of proper healthcare thus increasing the burden of disease on the already burdened economy of the country. Therefore, there is a dire need of coordination between different healthcare programme at all levels of healthcare system. The main purpose of this programme was to provide health education at all levels particularly at the community and primary level to strengthen the referral pathways from community to tertiary level for DM, DR and CB in Hyderabad District, Pakistan. All the referrals were actively monitored by Sindh Institute of Ophthalmology and Visual Sciences (SIOVS), Hyderabad, Pakistan. We present the results of this community-based screening programme.
Methods
In this prospective cross-sectional data collection, screening for diabetes, DR and CB in Hyderabad District, was performed from January 2014 to December 2015. Pakistan has four provinces, Sindh being the second largest province by population. Hyderabad is the second largest district of Sindh Province, with a population of 2.8 million. It is further divided into four administrative divisions (Talukas): Hyderabad City, Hyderabad Rural, Latifabad and Qasimabad. A total of 1101 LHWs from two divisions (Hyderabad Rural; 0.65 million population and Latifabad; 0.7 million population) were trained and sensitised in community mobilisation and awareness-raising about the DM, DR and CB. They were trained in recognising signs and symptoms of the eye-related disease and identifying high-risk potential patients with diabetes and referring them. The LHWs were trained 2 weeks prior to the starting of the screening programme. Follow-up visits to BHUs were carried out by the project team (community mobiliser, optometrist and ophthalmic technologist) to examine and treat/refer screened out patients and inspect the progress of LHWs. Proper record keeping of patients referred and treated was maintained at all levels.
The project design included: capacity building of LHWs at primary level to identify potential high-risk patients with diabetes and common eye diseases in children and refer them to nearby BHU. At BHU, the project team visited at the designated day to treat the referred patients and also offered hands on training to BHU doctors. LHWs were assigned to provide verbal awareness about visual health issues, data collection of the population and regarding the project to the population which was screened. As it was a mass screening programme, it was not feasible to obtain individual consent from each patient due to time and work force constraints but the patients were made aware that they were being screened as a part of this project. For diabetes and DR, all patients who were ≥40 years having family history of diabetes, obesity (body mass index (BMI) was used as a screening tool for overweight or obese in adults; BMI >30 was considered as overweight) or polyuria and those with impaired random blood glucose (RBG) level were included for funduscopy to detect any diabetic changes in their retina. However, those with normal glucose level were excluded from the study. For CB, all children from day 1 up to 15 years of age having any eye problem were recruited in the study. LHWs are the first point of contact to the health system for integrated model of care for the identification of DM and screening of DR and CB within the health system of Pakistan. They screened and referred potential patients to BHUs, where they were further assessed by medical officers (MOs) with the support of qualified optometrist and referred to tertiary care eye hospital, SIOVS, Hyderabad for advanced treatment and management (figure 1).

Integrated model of screening programme for DR and CB. BHU, basic health unit; CB, childhood blindness; DR, diabetic retinopathy; LHW, female heath worker; SIOVS: Sindh Institute of Ophthalmology and Visual Sciences.
LHWs were trained in the basic eye diseases and for this purpose a course was designed which included priority eye diseases, their signs, symptoms and management. The LHWs were expected to raise awareness and refer patients to nearest BHU.
At BHU level, the project team (manned with qualified optometrist) during the life of the project visited each BHU on pre-planned schedule and checked patients who were referred by the LHWs. Patients were treated and complicated cases were referred to SIOVS, Hyderabad for further management on tertiary level. During these visits, the team also offered orientation to the MOs at BHU. The BHU once oriented was expected to offer primary eye care at BHU level and refer complicated cases to tertiary level, that is, SIOVS. The BHU staff was also expected to manage diabetes.
SIOVS was expected to receive and offer tertiary-level care to the referred patients of DR and childhood eye diseases.
The strategy
This project improved access for vulnerable groups to high-quality diabetic and paediatric eye care services. Strengthening capacity of the community healthcare workers/LHWs for community mobilisation and awareness-raising about DM, DR and CB:
Strengthening capacity for screening DM, diabetes related and CB at the primary-level health facilities.
Strengthening referral pathways from community to primary to secondary/tertiary levels.
Strengthening capacities for service delivery at all levels of health system; the community primary, secondary and tertiary levels.
A large part of our effort was concerned with early detection and management of eye disorders thus developing on preventive ophthalmology.
Programme orientations and training of trainers (TOT programme)
The objective of the TOT programme was to enhance the capacities of the MOs, female health supervisors (LHSs) and the LHWs working at the grassroot levels under the Department of Health and National Programme for Family Planning and Primary Healthcare, commonly known as LHWs programme:
The MO training was followed by a 1-day ToT session for LHSs. The ToT was followed by training workshops of LHWs associated with each BHU.
LHWs were given orientation on: DM, its identification, complications, prevention and referring high-risk individuals (family history, weight and lifestyle), DR, its possible treatment and end referral points and CB.
Training packs
Each LHW was given a training pack consisting of the following items:
A booklet (Urdu/Local Language Sindhi) on DM, DR and common eye diseases in children.
Triplicate referral slips for referring patients from communities to the BHU.
LHW monthly activity report.
Printed Information, Education and Communication material on DM, DR and CB.
Tertiary referral
The high-risk patients of DR and CB were referred to SIOVS, where they underwent full ophthalmological examination by consultant vitreoretinal surgeon and paediatric ophthalmologist, respectively. They had the necessary management according to the severity of DR which included fundus fluorescein angiography, pan retinal photocoagulation or surgery. The children with treatable problems like cataract, glaucoma, squint and trauma were surgically managed.
Awareness raising campaigns were carried out at all 11 BHUs of the two divisions, Hyderabad Rural and Latifabad. Community support groups associated with each BHU were used to spread awareness about DM, DR and CB. In addition, billboards, banners, TV talk shows, community awareness walks, newspapers, cable TV messages and World Sight Day were used for the same purpose.
LHW refresher trainings were conducted in seven BHUs to review LHWs performance and coverage of their respective service communities. Follow-up was done on non-complying patients through telephone by the project team, through LHWs, providing transport facility resulting in increasing compliance up to 66%.
Data analysis
The data regarding different diseases in the screening project was arranged and analysed using SPSS for Windows software (V.19, SPSS). Frequency and percentages were calculated on the basis of age, gender and year.
Results
A total of 995 244 (74%) population was covered in this community-based screening programme during which 45 first level care facility trainers, 50 LHSs and 1101 LHWs were trained. A total of 31 812 (80%) houses were visited by the LHWs. Orientation in Primary Eye Health, DM, DR and CB was given to all the 60 MOs based in the 11 BHUs at the two divisions: Hyderabad Rural and Latifabad.
DR screening results
Total 16 760 adult patients (>15 years) were screened for diabetes in 2014 and 2015. RBG level of 3075 (18%) patients was >140 mg/dL. Out of these patients, 17% were diagnosed with DR. The details of diabetic screening is given in table 1. Majority of the patients were referred to the BHUs by LHWs. The details of referral to the BHUs is given in table 2.
Details of diabetic screening in 2014 and 2015
Details of referral to BHUs in 2014 and 2015
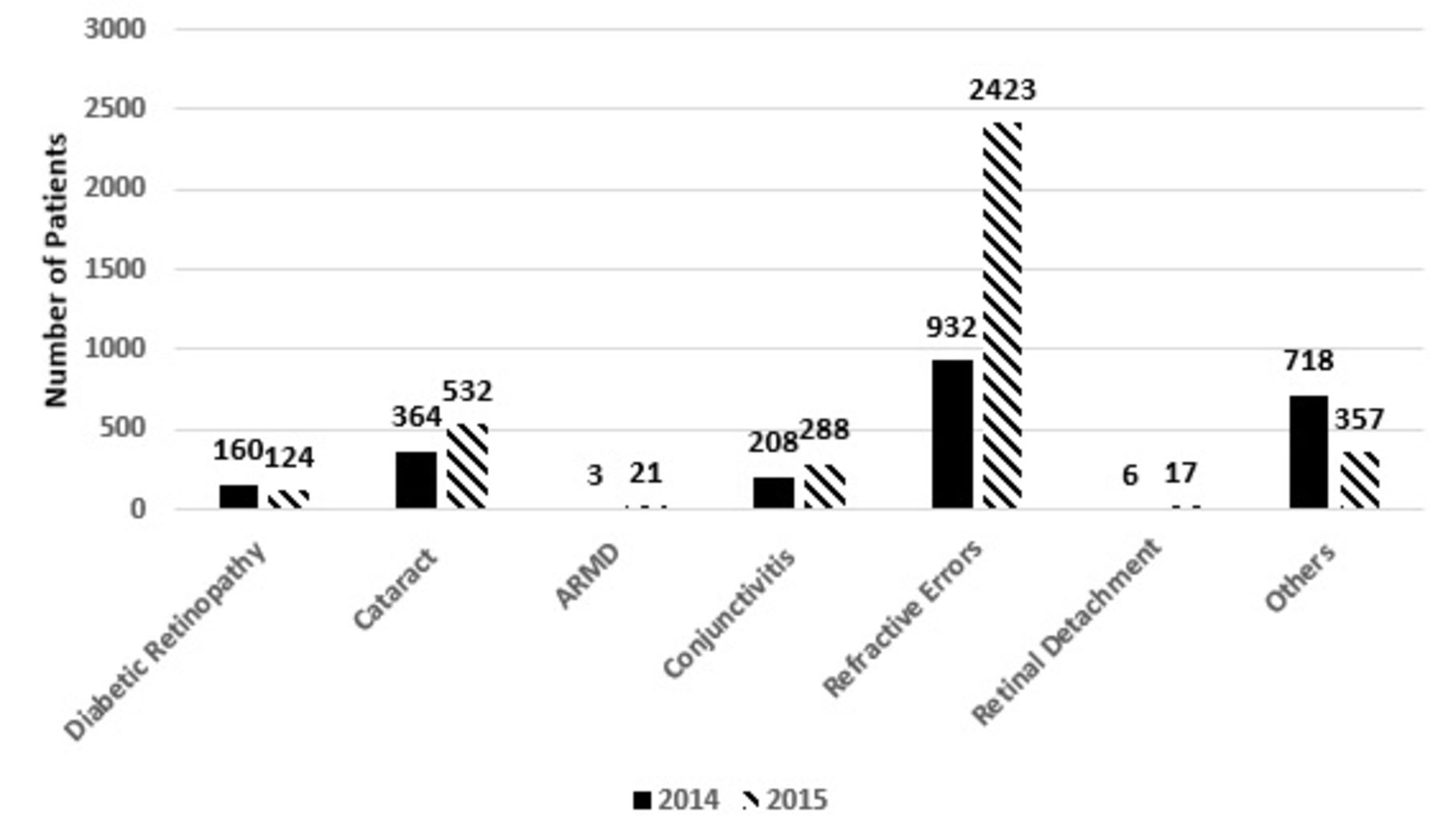
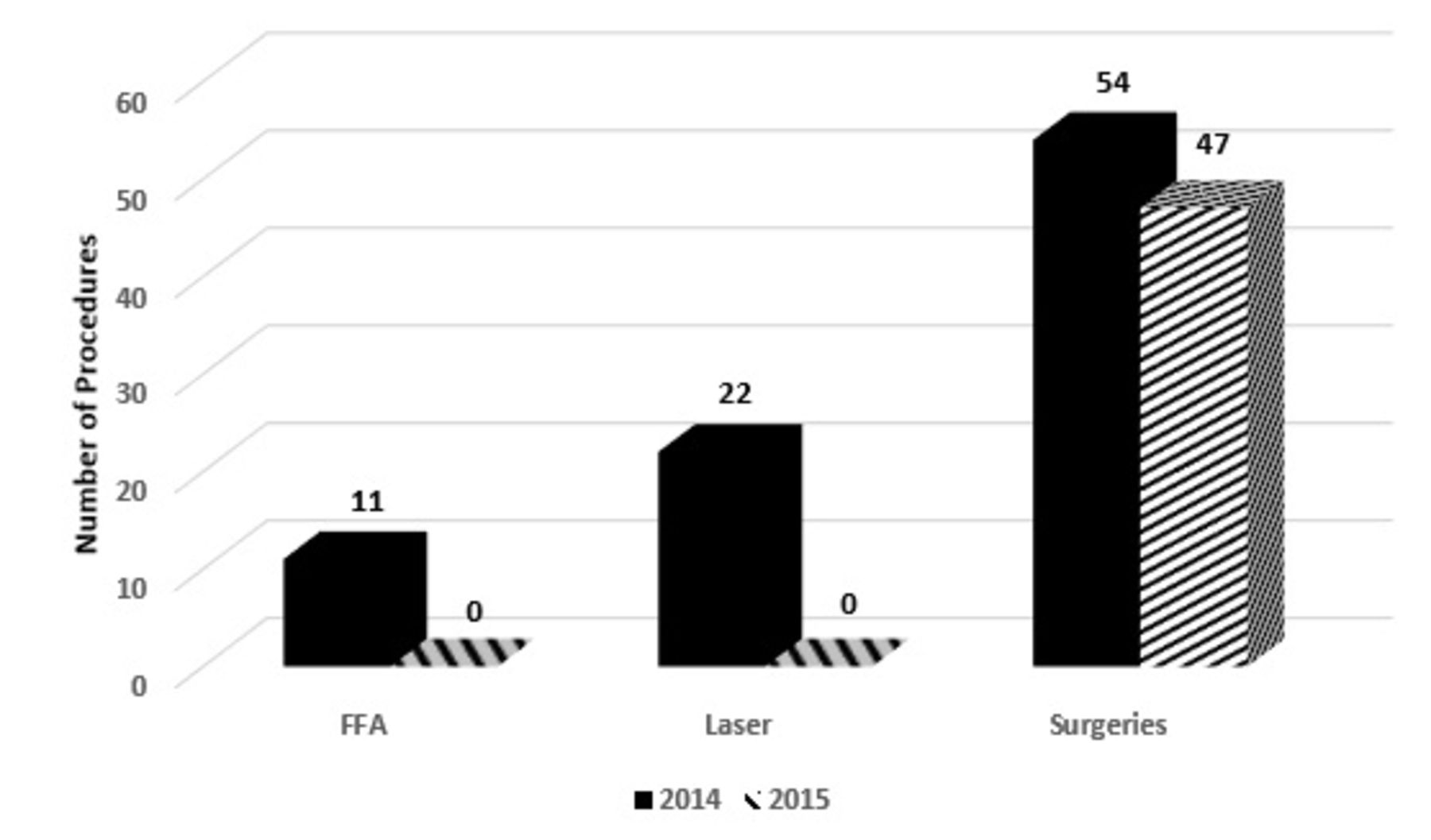
Refractive errors were the most common disease diagnosed among adults during screening for DR, followed by cataract, conjunctivitis and DR (figure 2). Various diagnostic and therapeutic procedures performed for managing DR at SIOVS are shown in figure 3.

Clustered column chart showing frequency of various diseases diagnosed in 2014–2015 in adults during screening for DR. ARMD, age-related macular degeneration; DR, diabetic retinopathy.

Various procedures performed for managing DR at SIOVS. DR, diabetic retinopathy; FFA, fundus fluorescein angiography; SIOVS, Sindh Institute of Ophthalmology and Visual Sciences.
CB screening results
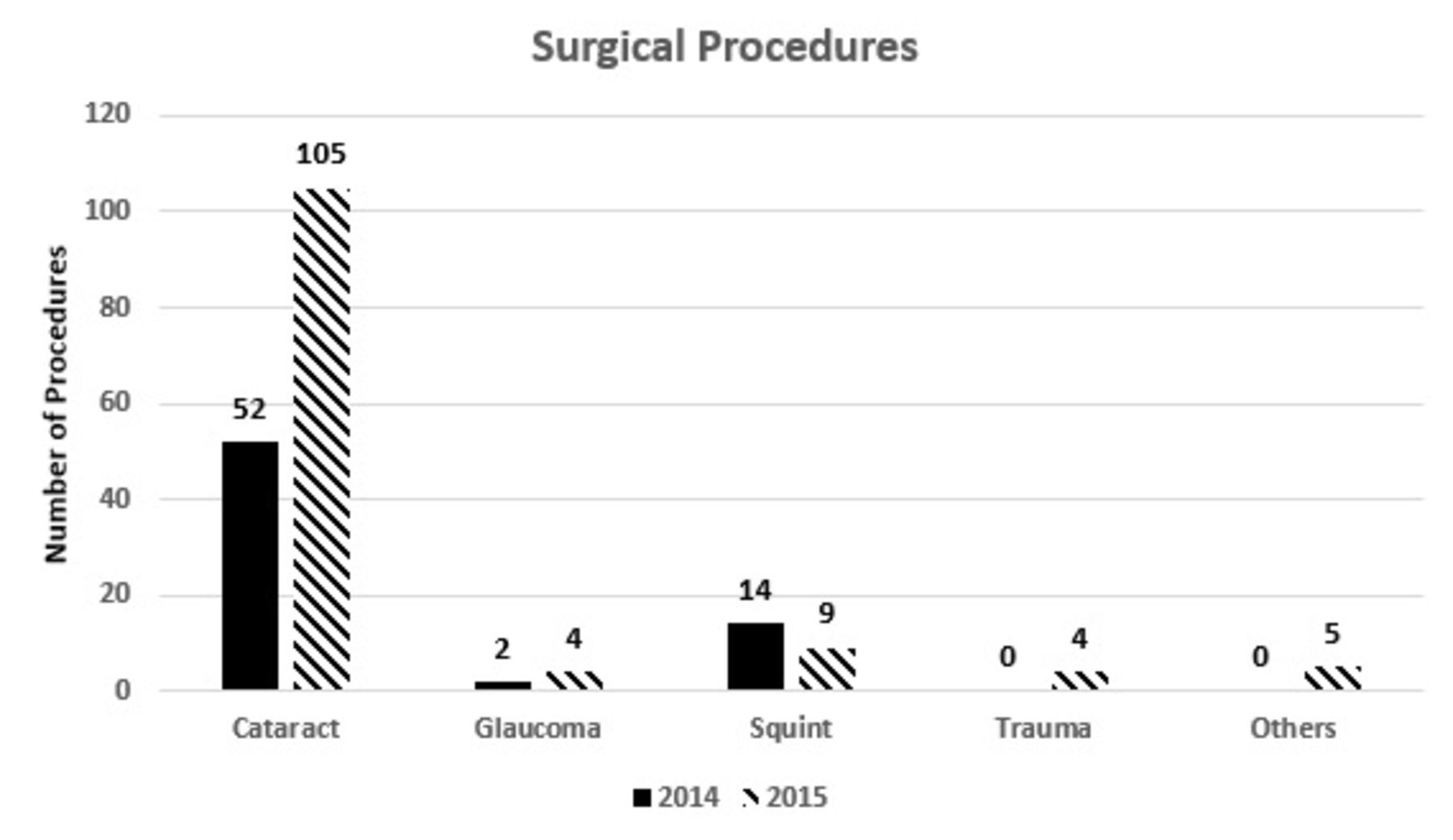
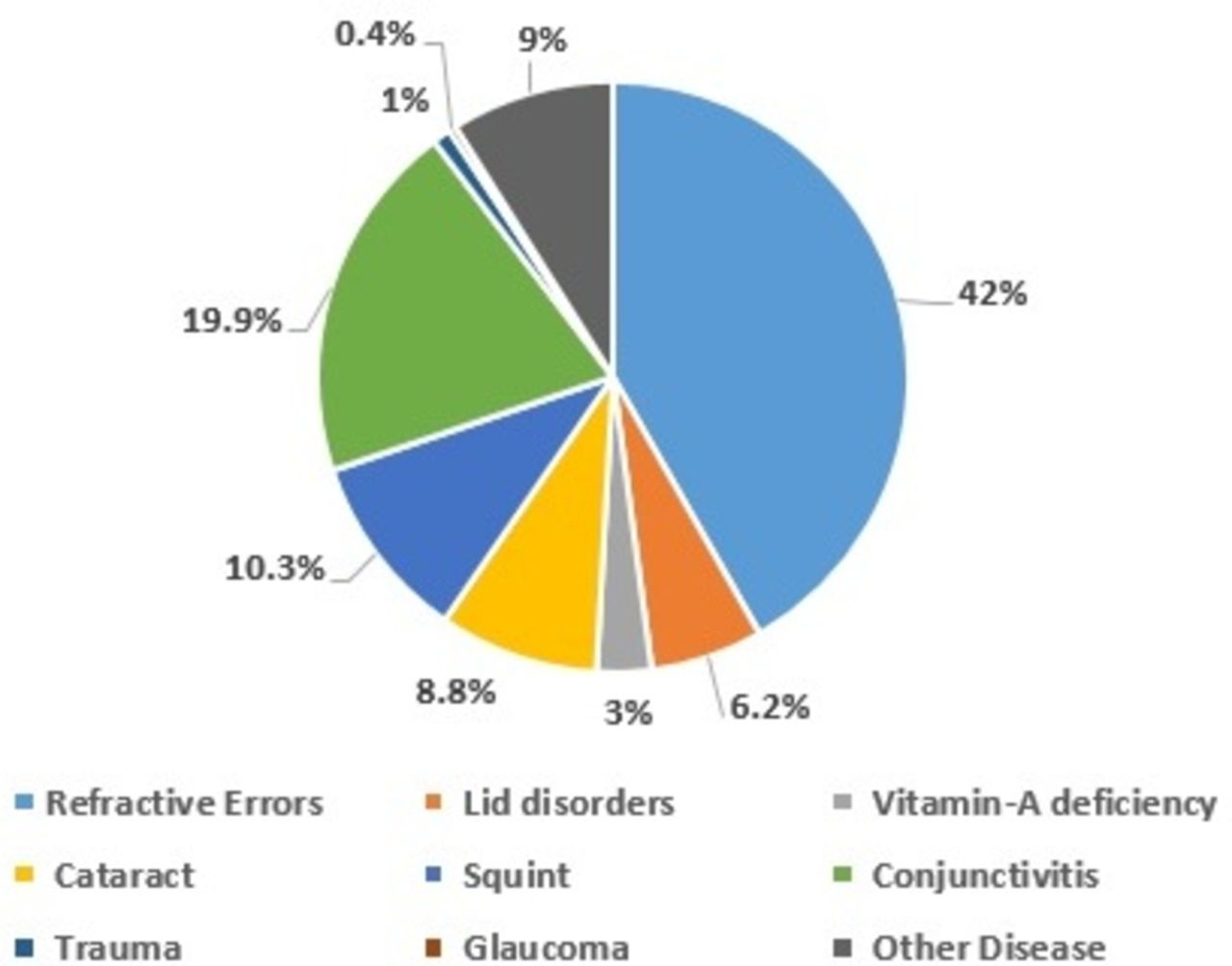
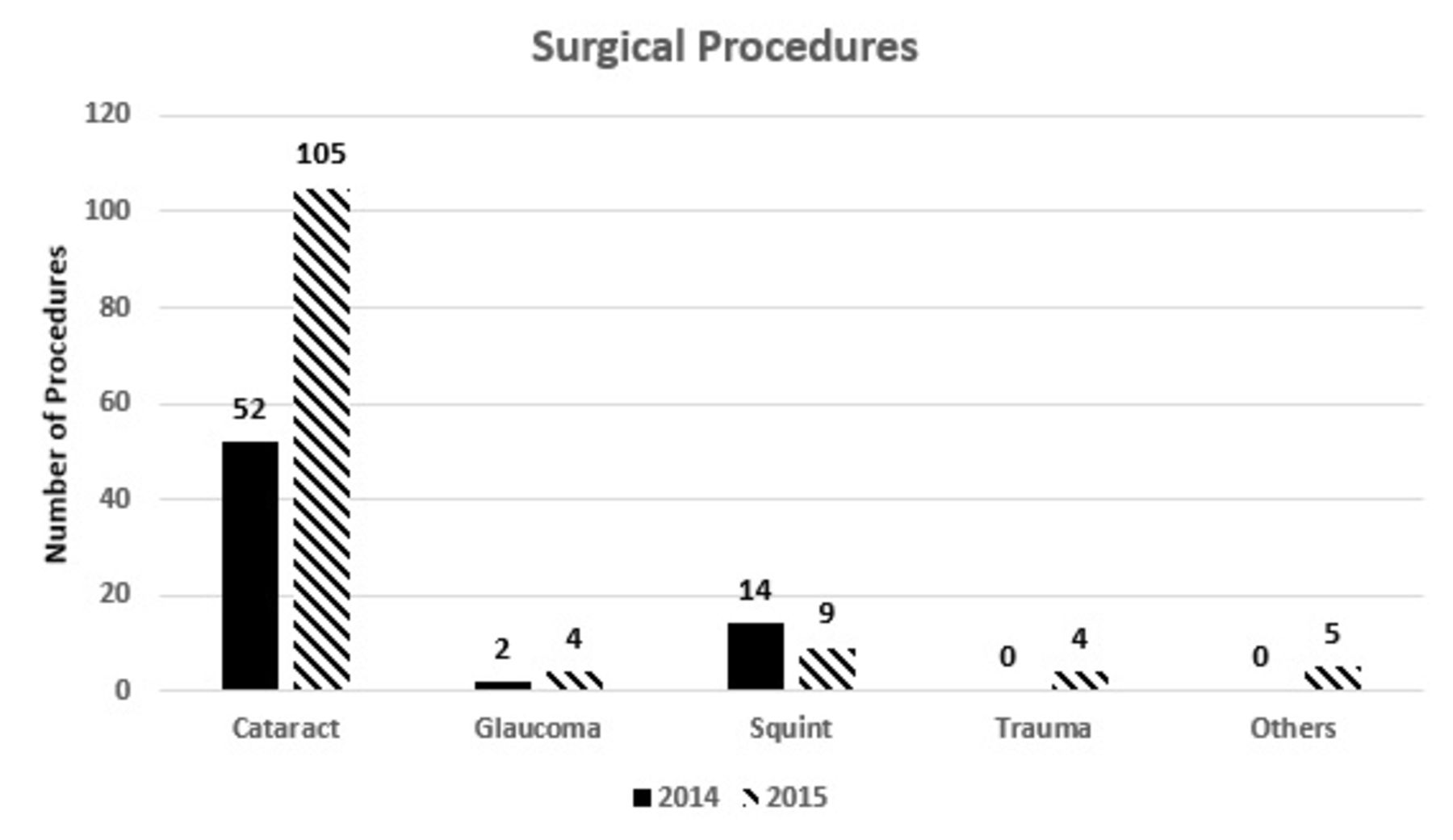
Total 2622 children (0–≤15 years) were screened during 2014 and 2015; out of these children, 1272 (49%) were boys and 1350 (51%) were girls. The frequency of various diseases diagnosed in 2014 and 2015 among children during screening for CB is shown in figure 4. Refractive error (42%) was the most common cause of childhood visual impairment, while 8.8% had cataract and 3% were found to have vitamin A deficiency (figure 4). Cataract surgery was the most common surgical procedure performed in children (figure 5).

Pie chart showing percentages of various diseases diagnosed in 2014–2015 among children during childhood screening for blindness.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Surgical procedures performed in children during 2014–2015.
Discussion
In our study, over 18% adult patients were found to have impaired RBG levels, which is probably due to ignorance, illiteracy and poor financial conditions. In 2015, there were over 7 million cases of diabetes in Pakistan which is expected to double to 14.4 million by 2040. The prevalence of diabetes was 6.9% in the adult population (20–79 years), while it is estimated that 3.5 million were undiagnosed.1 Globally one in two adults is unaware that they have diabetes, most of these patients have type 2 diabetes. Most of these undiagnosed cases will not take any measures to manage their condition and therefore end up with serious complications like heart failure, DR and chronic renal failure.9–11 There was a dire need of a screening programme for early diagnosis and management of diabetes. This is particularly true in a developing low-income country like Pakistan, where people are reckless about their health due to poor economic conditions and lack of awareness. Our screening programme therefore not only aimed at the screening of diabetes but also creating awareness about the disease and educating people at the lower level. This created better chances of management and preventing complications of diabetes.
Hyderabad is the second largest district of Sindh Province, with a population of 2.8 million. It is estimated that there are 195 000 persons with diabetes in District Hyderabad (6.8% of the population aged 20–79 years). Previous Fred Hollows Foundation (FHF) projects and other studies have demonstrated that DR is present in up to 30% of persons known to have diabetes. Therefore, it is estimated that in District Hyderabad, there are approximately 58 000 persons at risk of vision loss from DR.12
There has been a variable prevalence of DR in national studies ranging from 15% to 58%, probably due to the different sample sizes and most of the studies being hospital based.12–14 In our study, the prevalence of DR was 17% which is comparable to the data available. But our sample size was larger than most of the studies as we screened a large population which has not been done before.
Like any community the most common cause of visual impairment in children in our community was refractive errors (42%). There has been a wide variability in the prevalence of refractive errors worldwide. In Pakistan, majority of the studies have reported a prevalence of 1%–15% which is quite low compared with our study.15–17 This may be due to a very selected sample size of ethnic group or school going children which resulted in under reporting of the actual number. While in our study we selected a large population based on age group only which reduced the bias. Furthermore our outreach programme accessed those children who would otherwise not visit a tertiary healthcare facility, thus resulting in actual presentation of prevalence of refractive errors. Our results are congruous with WHO results of visual impairment due to refractive errors (42%).6 While some other screening programme reported an even higher prevalence of refractive errors of up to 68%.18 Childhood visual impairment is a serious issue worldwide particularly in developing countries where due to large families children often face neglect especially regarding their health. Illiteracy, poor socioeconomic conditions and lack of basic health facilities all add up to the already magnanimous issue of visual impairment in children of third world countries. All these factors lead to irreversible blindness in many a times preventable conditions. The key to prevention is early screening, diagnosis and management of these potentially preventable problems. The other causes of visual impairment among children included cataract (8.8%) and vitamin A deficiency (3%). The prevalence of these two was comparable to other studies in Pakistan.17 Due to our screening programme most of these children had a timely diagnosis of preventable visual impairment and were successfully managed at SIOVS, which would have not been possible otherwise. The key to manage blindness in patients with diabetes and children is early diagnosis. This is only possible by mass screening programme like ours which covered a large population.
At community level, the referral system in Pakistan has been deficient since a long time. Bhutta et al19 and Siddiqi et al20 have reported the ineffectiveness of the referral pathways. With our community-based screening programme we not only screened the patients but educated the staff at community level to actually strengthen the referral pathways thus the healthcare system. Our results clearly reflect the effectiveness of proper education and awareness in proper functioning of the referral system. This screening programme did not end here, as the education imparted to the staff remains and they have been actively referring more patients to tertiary levels for management. So it is safe to say that this is an ongoing cycle of referral which continues to strengthen the healthcare referral system.
Recommendations
Like any other department in Pakistan, healthcare is predominantly dependent on the non-governmental organisations (NGOs) to fill the crevices which the Government or public sector fails to address. Due to economic, financial, physical, geographical constraints and poor distribution of resources, the public sector has been struggling to achieve its goals of providing quality healthcare to all. Our results reflect the effectiveness of merging the NGOs with the public sector. It is unjust to wholly place the burden of healthcare on either private or public sector. We live in an era of ever developing health problems and issues which need proper diagnosis, referral and management which cannot be achieved solely by any one sector. We recommend that the government work on more health development projects with the NGOs to strengthen the existing healthcare system.
Conclusion
The diabetic screening programme detected a greater prevalence (17%) of retinopathy in patients with diabetes living in Hyderabad District. The most common cause of childhood visual impairment was refractive error (42%), which was successfully managed due to timely diagnosis. A large number of patients benefitted from our community-based screening programme, particularly patients with diabetes and children with preventable visual impairment due to timely diagnosis and proper management. Screening programme are the most cost-effective answer to preventing blindness in low-income countries like Pakistan.
Acknowledgments
The authors thank Sindh Institute of Ophthalmology and Visional Sciences (SIOVS), Hyderabad, Pakistan for implementing this project in Hyderabad district; Mr Asfandyar Khan, Project Officer, The Fred Hollows Foundation for supporting this project from FHF country office; The Fred Hollows Foundation through its DFAT support PAPAB Project (2013-2016) for providing the human resources and training to carry out the screening. They also acknowledge the efforts of all the LHWs, LHSs, MOs, trainers, facilitators and the staff of SIOVS.
References
Footnotes
Contributors NBN, Drafted the manuscript, statistically analysed data and reviewed literature. KIT, designed the study, statistically analysed and critically reviewed the manuscript. FA, conceptualised the study and approved the final version. MAK and MNM, diagnosed the cases, collected data and did critical appraisal of findings.
Funding The Fred Hollows Foundation through its DFAT funded Pakistan Australia Prevention of Avoidable Blindness (PAPAB) Project.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval Ethical Review Committee Sindh Institute of Ophthalmology and Visual Sciences, Pakistan.
Provenance and peer review Not commissioned; externally peer reviewed.