Article Text

Abstract
Background/aims New antibiotic agents and changing susceptibility patterns may have changed the empirical treatment of bacterial keratitis. Our objective in this study was to survey cornea specialists’ practice patterns in the initial treatment of bacterial ulcers.
Methods This study consisted of a short online survey emailed to members of the Cornea Society listserv for an international sample of cornea specialists. Data collection began July 2014 and ended October 2014.
Results A total of 1009 surveys were emailed, and we received 140 (14%) responses. The majority of US clinicians surveyed (n=83, 80%) chose fortified antibiotics empirically, with 55% (n=57) selecting fortified vancomycin and 16% (n=17) using fluoroquinolone alone. International respondents were twice as likely to use fluoroquinolone monotherapy (31%, n=11, p=0.07) and less likely to use fortified vancomycin (33%, n=12, p=0.03). Forty-five per cent (n=46) of US respondents reported that their initial antibiotic choice covered methicillin-resistant Staphylococcus aureus, compared with 22% (n=8) of international respondents (p<0.01). Overall, respondents who were concerned about availability of antibiotics and toxicity were 20.86 (p<0.001) and 7.48 (p<0.001) times more likely to choose fluoroquinolone monotherapy, respectively. If respondents’ primary considerations were broad spectrum coverage or antibiotic resistance they had 7.10 (p<0.001) and 12.51 (p<0.001) times the odds of using fortified vancomycin, respectively.
Conclusion Practice patterns for the initial treatment of bacterial keratitis vary with clinicians in the USA being more likely to use fortified antibiotics versus fluoroquinolone monotherapy and more concerned with resistant organisms than their international peers.
- Cornea
- Infection
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
There is debate over the best empirical treatment for bacterial keratitis, and there are regional variations in practice patterns of corneal specialists.
This survey demonstrates that practice patterns are influenced by concern over availability and toxicity versus broad spectrum coverage and resistance. Overall, respondents in the USA were more likely to treat with fortified antibiotics than their international peers.
A well-designed clinical trial on the treatment of bacterial ulcers is needed to help clinicians initiate the best treatment and ultimately reduce morbidity.
Introduction
In the literature and at our own institution, there has been debate about the use of commercially available fourth-generation fluoroquinolones versus compounded fortified antibiotics such as vancomycin and tobramycin for the initial treatment of bacterial corneal ulcers. Determining the best treatment depends on the causative organism; however, Gram stain and culture results are not available for hours to days, and initial therapy is commonly empirical. Several randomised controlled trials have shown equivalency between the fluoroquinolones and fortified antibiotics.1–5 In the recent Steroids for Corneal Ulcer Trial, no bacteria were resistant to moxifloxacin.6 Despite this, the use of fortified antibiotics remains quite common.7 8 Of note, most of these studies occurred in developing countries where bacterial resistance patterns are likely to be quite different from the those in developed countries such as the USA.
New antibiotic agents, such as topical linezolid, and changing susceptibility patterns may have altered the empirical treatment of bacterial keratitis.9 Here we assess corneal specialists’ current practice patterns regarding initial treatment of severe central bacterial ulcers.
Materials and methods
An international survey was distributed via email to members of the Cornea Society listserv. Participation was completely voluntary and anonymous, and no identifiers were collected including name, age or sex. The survey was initially distributed on 21 July 2014 via the internet survey tool SurveyMonkey (surveymonkey.com; Palo Alto, California), with one reminder on 26 August 2014. Data collection was closed in October of 2014.
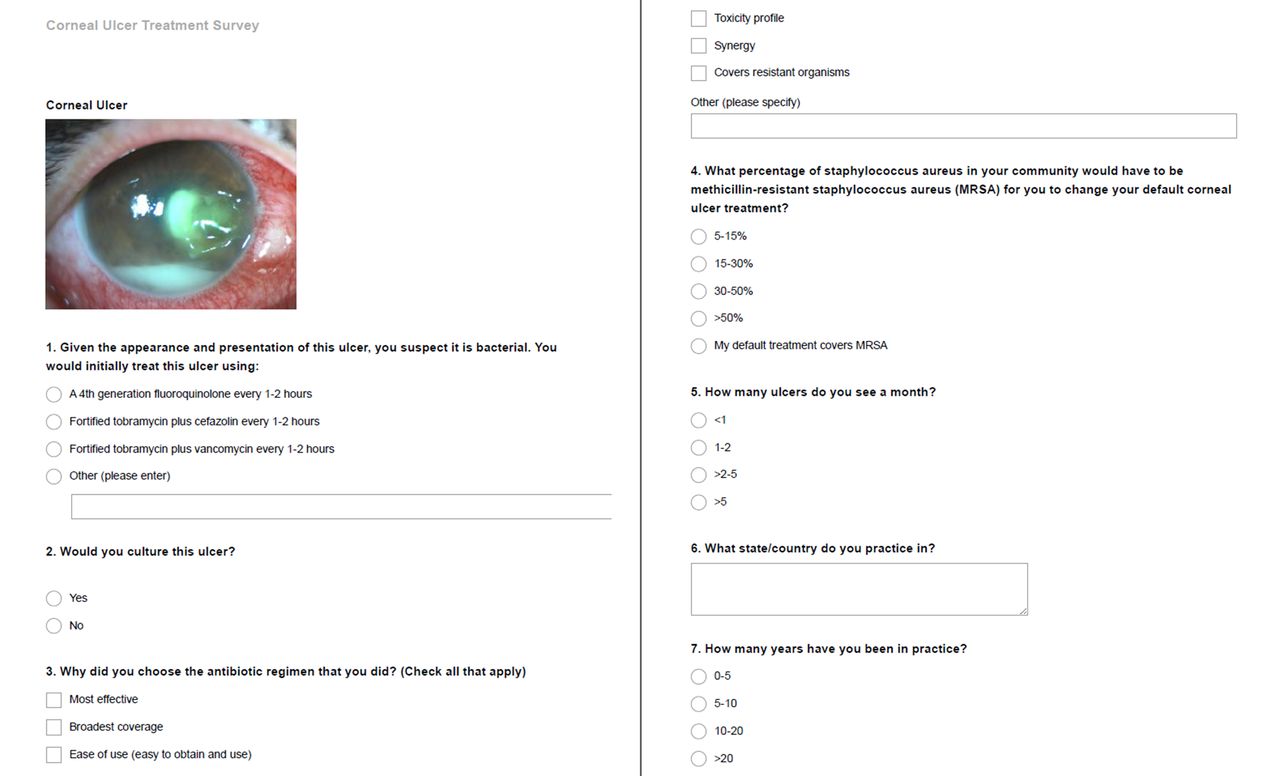
The survey consisted of seven questions (figure 1). Respondents were presented with the clinical scenario of a patient with a large, central, bacterial corneal ulcer and were asked what their empirical antibiotic treatment would be, why they chose that regimen and whether they would obtain cultures prior to instituting treatment. Specific antibiotic regimens given as options included fourth-generation fluoroquinolones (such as moxifloxacin and gatifloxacin) and fortified antibiotics (including tobramycin, vancomycin and cefazolin). Respondents were also queried regarding their demographics including their geographic location, the average number of corneal ulcers seen per month as well as the number of years they had been in practice.

Survey distributed to corneal specialists via email.
Finally they were asked what percentage of Staphylococcus aureus in the community would have to be methicillin-resistant Staphylococcus aureus (MRSA) for them to cover MRSA empirically.
Responses were collected and analysed using descriptive statistics with Stata V.14.0. χ2 test was used to compare responses between international and US respondents, and logistic regression models were used to assess the relationship between specific concerns, such as toxicity or antibiotic resistance and choice of antibiotic. Institutional review board exemption was obtained from the University of California, San Francisco Committee on Human Research. The study adhered to the Declaration of Helsinki and all federal and state laws.
Results
A total of 1009 cornea specialists were members at the time the survey was sent out. One hundred forty responses to the survey were received, for a response rate of 14%. Respondents were mostly from the USA (n=104), with the remaining international respondents (n=36) coming from 17 countries on six continents (table 1). Many respondents had greater than 20 years of clinical experience (n=62, 44%), followed by 10–20 years in practice (n=33, 24%), 5–10 years in practice (n=30, 21%) and 0–5 years in practice (n=15, 11%). In general, the international respondents encountered more cases of infectious keratitis per month, with 42% seeing more than five cases per month versus 24% of US respondents (p=0.05). When asked if they would culture a large central ulcer, all international respondents (n=36) and 98% (n=101) of US respondents reported that they would (two US respondents, or 2%, said they would not).
Geographic distribution of respondentsl
Respondents were asked about their empirical treatment of bacterial keratitis, and their responses revealed marked differences in practice patterns between clinicians in the USA and in other countries, as seen in figure 2. In the USA, the majority of clinicians surveyed (n=83, 80%) chose fortified antibiotics as their initial treatment, with 55% (n=57) choosing fortified vancomycin. Sixteen per cent (n=17) of US clinicians surveyed chose to initially treat with fourth-generation fluoroquinolones alone. International respondents were twice as likely to use fluoroquinolone monotherapy (31%, n=11, p=0.07) and were less likely to use fortified vancomycin with 33% reporting it as their empirical choice (n=12, p=0.03).

{kind=link}
{kind=link}
Graph showing antibiotic choice of US and international cornea specialists for empirical treatment of bacterial keratitis.
Reasons for selecting their chosen initial antibiotic were largely similar across US and international sites. Clinicians reported desiring broad-spectrum antibiotic coverage most often, with 78% (n=81) of US respondents and 89% (n=32) of international respondents citing this as a reason for their antibiotic choice. Both groups also reported the following reasons with similar frequency: most effective (n=43, 41% US vs n=15, 42% internationally), availability (n=33, 32% US vs n=12, 33% internationally), synergy (n=15, 14% US vs n=6, 17% internationally) and toxicity profile (n=13, 13% US vs n=5, 14% internationally). US respondents were more concerned about covering resistant organisms, listing this as a reason for their empirical antibiotic choice more than twice as often as international respondents (n=41, 39% vs n=7, 19%, p=0.03).
Forty-five per cent (n=46) of US respondents reported that their empirical antibiotic regimen covered MRSA, compared with 22% (n=8) of international respondents. Table 2 contrasts US and international clinicians’ threshold for empirical MRSA coverage, showing that international clinicians had a lower threshold for empirical MRSA coverage than did US clinicians (p<0.01).
Threshold for empirical methicillin-resistant Staphylococcus aureus coverage (MRSA). Percentage of MRSA in the community necessary to change the default corneal ulcer treatment to include MRSA coverage.
Table 3 shows the relationship between the different reasons for choosing a particular antibiotic and the likelihood of selecting fluoroquinolone monotherapy or fortified vancomycin, correcting for location (defined as US or international). Respondents who listed availability as a primary consideration had 20.86 times the odds of choosing fluoroquinolone monotherapy (p<0.001). Concern over ocular surface toxicity was also predictive of choosing fluoroquinolone monotherapy (OR=7.48, p<0.001). Not surprisingly, respondents concerned about resistance had 12.51 times the odds of choosing fortified vancomycin (p<0.001), while broad spectrum coverage was also a statistically significant predictor for selecting vancomycin (OR=7.10, p<0.001).
Reasons for antibiotic of choice. Logistic regression models predicting likelihood of choosing fluoroquinolone monotherapy and fortified vancomycin, correcting for location.
Discussion
In this study, we report the results of an international survey of cornea specialists regarding their empirical treatment of large central corneal ulcers. We found that practice patterns differ between US and international sites, with US clinicians more likely to use fortified antibiotics as their initial treatment. They were also approximately twice as likely to use fortified vancomycin empirically. Prior surveys have found that cornea specialists are more likely than general ophthalmologists to treat bacterial keratitis with fortified antibiotics.7 10 US respondents were more concerned about resistant organisms and also more likely to include coverage for MRSA in their default treatment.
Concern about the availability of antibiotics was the greatest predictor of fluoroquinolone monotherapy. Fortified antibiotics require a compounding pharmacy and can be difficult for clinicians to access. Concern over ocular toxicity was the second strongest predictor of fluoroquinolone use in our study. Fortified antibiotics and in particular fortified vancomycin are known to cause significant ocular surface toxicity, such as increasing epithelial defect size or conjunctival injection, which can sometimes be difficult to distinguish from progression of the corneal infection. Some have advocated using topical linezolid as an alternative to vancomycin, which has less toxicity but still covers resistant organisms including MRSA.9 Interestingly, no one in our survey reported using linezolid. Our observation that those concerned with broad-spectrum coverage were more likely to choose fortified antibiotics and those favouring a low toxicity profile were more likely to choose a single agent could be influenced by the availability of particular antibiotics.
Fluoroquinolone antibiotics penetrate ocular tissues well and have good safety profiles with minimal toxicity to the ocular surface. They also exhibit broad coverage of bacterial organisms implicated in bacterial ulcers. The primary target of fluoroquinolones is DNA gyrase, an essential bacterial enzyme. There is reason to believe that because of this mechanism of action, they may be more susceptible to the development of resistance than other antibiotics.11 Rates of MRSA infection have been increasing in North America, and ocular isolates in the USA have been reported to be resistant to fluoroquinolones approximately 80% of the time.12–14 In our study concern for antibiotic resistance and broad spectrum coverage were highly predictive of choosing fortified vancomycin after controlling for location. The fact that international cornea specialists both have a lower threshold for MRSA coverage and are less likely to be using fortified antibiotics suggests that they consider the prevalence of MRSA to be relatively low in their population.
The strengths of this study include the geographic diversity of respondents, providing both US and international perspectives and representing a broad range of experience. In addition, a large number of our respondents were experienced physicians and seeing ulcers frequently in clinical care. Limitations include the fact that we only surveyed members of the Cornea Society listserv, therefore our results may not be generalisable to all ophthalmologists. Additionally the survey did not ask respondents about their practice setting, which may be related to empirical antibiotic choice since those in academic settings may have more access to fortified antibiotics. Another limitation would be the multiple-choice format of our question about antibiotic preference because other options such as vancomycin monotherapy were not listed (in this case, we listed vancomycin only in conjunction with other antibiotics because it only covers Gram-positive bacteria). We attempted to address this by giving respondents the option to write in their own preferred antibiotic, but it is possible the question format affected responses given.
Practice patterns for the initial treatment of bacterial keratitis vary with clinicians in the USA more likely to use fortified antibiotics versus fluoroquinolone monotherapy and more concerned with resistant organisms than their international peers. These differences may be due to multiple factors, including varying prevalence of resistant organisms, lack of availability of fortified antibiotics and concerns for ocular toxicity. Determining which of these factors impact clinical outcomes, such as visual acuity, should be an important focus of future research.
References
Footnotes
Acknowledgements Individual support for this study came from K23 EY025025 (JRN), an unrestricted grant from the Peirles Foundation (JRN) and an unrestricted grant from Research to Prevent Blindness (JRN).
Contributors Corresponding author JR-N contributed to study design and implementation, data analysis and writing of this manuscript. AA contributed to data analysis and writing of the manuscript. JS and MG were involved in design and implementation of this study. MM contributed to study design and implementation as well as editing of the manuscript. TL contributed to the design of the study, data analysis and editing of the manuscript.
Funding There are no conflicts of interest to declare. Corresponding author Dr Jennifer Rose-Nussbaumer contributed to study design and implementation, data analysis, and writing of this manuscript. Ariana Austin contributed to data analysis and writing of the manuscript. Dr Julie Schallhorn and Dr Mike Geske were involved in design and implementation of this study. Dr Mark Mannis contributed to study design and implementation as well as editing of the manuscript. Dr Tom Lietman contributed to the design of the study, data analysis, and editing of the manuscript.
Ethics approval University of California, San Francisco Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.